
This is Ken Perrott’s response to Paul Connett’s first article – Fluoride debate Part 1: Connett.
Paul’s first article appears to be a general overview and not detailed consideration of the ten points he makes. I will be similarly brief in my response to each point. Paul may wish to go deeper into specific issues in later contributions and I will respond in more detail then.
The medical argument
Paul’s first 3 arguments rely on defining fluoridation as a medical treatment. This is a common anti-fluoridationist approach. I have no wish to argue about that definition as it is really just a matter of semantics. You could use a weak definition of “medicine” which can include practically anything in your diet the body uses and may tolerate over a wide range of intake without harm. Or a tighter definition implying a drug with some sort of marked effect in the body and requiring relatively careful control of intake. But whatever definition is used should be openly declared and applied consistently.
Opponents of fluoridation usually apply their definitions of “medicine” inconsistently and the argument becomes a classic bait and switch tactic. It uses a weak definition of “medicine” to capture fluoride and then switches to a tight definition to argue that use of fluoride requires rigid controls. This presents them with a number of problems because a weak definition of “medicine” must also include “natural” as well as “artificial” fluoride at natural levels in water a food. (A weak definition may also include many other elements – perhaps even water itself). There is no such thing as a “fluoride-free” water supply. If we exclude natural levels of fluoride (and most other elements) from our definition of “medicine” then why should we treat levels for artificially fluoridated water any differently?
Connett’s point 1: Why should we not be concerned about controlling the dose of natural levels of fluoride (or many of the other elements we consume) while only be concerned about the fluoride added as a “top up?” The are no differences between the “artificial” and “natural” fluoride anions in drinking water. In reality most elements like this have a sufficiently wide range of concentrations and intakes for efficacy that it is just ridiculous to treat them like powerful drugs which need accurate dosage.
Connett’s point 2: Similarly why make charges of indiscriminate intake only for artificially added F and not for natural levels of F and other elements? The small number of people, if any, who may have problems with fluoridation levels of F will also have the same problems with natural levels of F. Such people, if they real exist, will need individual responses to either natural or artificial levels of F and possibly other elements. These people will need individual responses whether their water supply is artificially fluoridated or not.
Connett’s point 3: Why demand “informed consent” for situations where natural levels of fluoride have been “topped up” and not require it for natural levels of fluoride – which in some situations may actually be higher than for fluoridated water supplies.
Is fluoride a nutrient?
Connett’s point 4: This also reduces to semantics – how should “nutrient” be defined? Paul restricts his definition only to elements involved in “biochemical processes” – a definition confidently excluding the role of F in bioapatites – bones and teeth. Yet bones and teeth are important to organisms – so the strengthening of bioapatites, and the reduction of their solubility, by incorporation of fluoride is important.
Perhaps we can agree that F is at least a beneficial element, even if we can’t reach agreement on the use of terms like “nutrient” and “essential.”
Biochemical processes and fluoride
Connet’s point 5: It is easy to cite literature references showing negative effects of fluoride but we should not ignore the conditions used. Most such studies refer to much higher concentrations than used in water fluoridation and this is also true for the review by Barbier et al, 2010 Connett cites.
Let’s not forget that community water fluoridation describes “topping up” fluoride concentrations to about 0.7 ppm F. Yet reviews of negative effects on biochemical process will quote studies which have used 50 ppm, 100 ppm or even greater concentration of F in drinking water. Opponents of fluoridation often seem completely oblivious of these huge differences in concentration when they present a long list of claims about the ill effects of fluoridation.
Another confusion readers often have with such reviews is the use of different units. The sensible reader must often apply a few conversion factors when checking the fluoride concentrations used in the reviewed studies. 1 mM = 19 ppm (or mg/L) for fluoride.
It is possible to find similar evidence of harmful effects of essential elements when present in high concentrations. Selenium is an example of such an essential element. This graph illustrates the situation for fluoride and is common to many elements.

Diagram from Ethan Seigel’s blog Starts with a Bang (see Weekend Diversion: Fluoridated Water: Science, Scams and Society).
I am not denying the usefulness of these studies of negative effects of fluoride. Researchers and policy makers should continuously assess research findings for their relevance to the fluoridation issue and guidelines used in regulations. But this assessment must be critical and intelligent – not simply a search to confirm biases.
Health authorities should not be swayed by populist naive interpretations of research.
Naturalistic fallacies
Connett’s point 6: Sure, organisms evolve to fit the parameters of their environment. But to say “it is more likely that nature knows more about what the baby needs than a bunch of dentists from Chicago or public health officials in Washington, DC” is really not a good way of deciding this issue. Do we really want to argue that the situations in which marine animals evolved are the best to aim for in a society which has undergone so much cultural and intellectual evolution? Are we to reject the idea that society should task experts to consider possible approaches for our future by the argument that “nature knows best” and give up all rights for humanity to improve its condition? Do we really think that the environment that ancestral species experienced millions of years ago are necessarily the best for us today?
Modern humans live in environments offering a range of natural dietary fluoride intakes. We know that very low or very high intakes present problems for our bones and teeth. We should not avoid the problems this presents by saying “nature knows best.”
The very low levels of F in breast milk may have more to do the with inorganic role of F in animal bodies than any wisdom that “nature” has.
Fluorosis
Proponents of fluoridation do acknowledge dental fluorosis in a negative, although minor, aspect of fluoridation.
Connett’s point 7: Opponents of fluoridation will often quote high values of the incidence of fluorosis which ignore the fact that much of it is “questionable” and/or “very mild.” These grades are really only cosmetic and usually can only be detected by a professional. Opponents may also hide the fact that the incidence of fluorosis for children living in fluoridated may often be the same as, or only slightly greater than, the incidence for children living in non-fluoridated areas.
The graphs below shows the situation reported for New Zealand in the 2009 New Zealand Oral health Survey (see Our Oral Health).
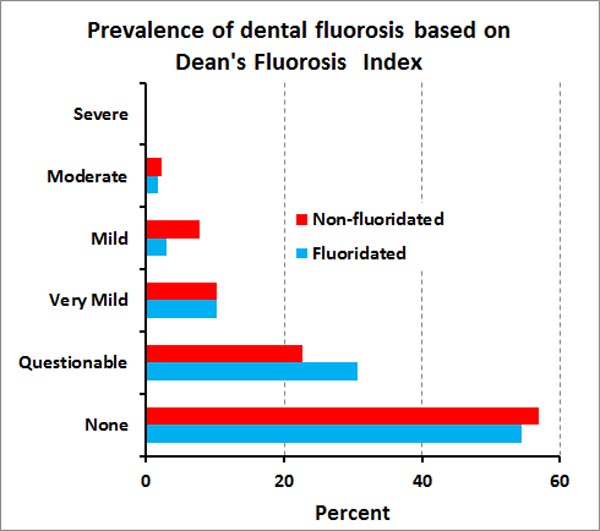
See Wikipedia for a brief description of Dean’s Fluorosis Index.
Health experts have generally concluded that the apparent rise in the incidence of fluorosis is caused by increases in other forms of fluoride intake, such as from eating toothpaste, and not from fluoridated water.
Fluorosis could well have been a normal feature of teeth and bones for a very long time. Remember many areas of the world are high in natural forms of fluoride and the body does not seem to have a process for fine regulation of blood and plasma fluoride concentrations. Perhaps we should consider very mild and questionable levels of fluoride as cosmetically perfectly acceptable. Considering the natural variation in fluoride intakes some people might argue that “nature knows best.”
Nature of fluoridating chemicals
Connett’s point 8: Anti-fluoridationists make wild claims about fluoridation chemicals. “They are industrial waste products, loaded with heavy metals and fluorosilicates are toxic and/or untested for toxicity!”
Claims of contamination with toxic elements are easily, and often, made but are never justified with any evidence. So lets look at the reality.
By-products that are used are not waste products – and surely we should aim for the efficient use of natural resources. The purchaser of any product will sensibly make sure it is suitable for their requirements – and these are rigidly defined for water treatment chemicals.
Suppliers are required to provide certificates of analysis and maximum values for contaminants in chemicals used for water treatment. Those regulations are determined from the maximum concentrations of contaminants allowed in the finished water for human consumption. Safety factors are also involved as well as allowance for contribution from other sources.
The table below contains analytical data for contaminants taken from certificate of analysis for the last batch of fluorosilicic acid used in the Hamilton, New Zealand, water treatment plant (see FSA column). I compare the data with the maximum allowed impurity levels of fluorosilicic acid defined in the regulations (Impurity limits column) and with an example of the contaminant concentrations in finished water (Drinking water column).
| Toxic Element | Impurity limits* | FSA** | Drinking water** |
| Sb (ppm) | 40 | <0.09 | – |
| As (ppm) | 132 | 0.4 | <0.002 |
| Cd (ppm) | 40 | 0.11 | <0.001 |
| Cr (ppm) | 660 | 0.8 | <0.001 |
| Hg (ppm) | 26 | < 0.05 | <0.001 |
| Ni (ppm) | 264 | < 1 | <0.001 |
| Pb (ppm) | 132 | 0.8 | <0.001 |
* Maximum acceptable contamination.
** From Certificate of Analysis
***For Gear Island Treatment Plant, Greater Wellington region.
There are several points to make.
1: These concentrations are extremely low, meaning that the final concentrations in the finished water are insignificant.
2: For comparison, column one provides the maximum permissible concentrations allowed for fluorosilicic acid used for water treatment ( NZ Water and Wastes Association Standard for “Water Treatment Grade” fluoride, 1997. ).
3: The NSF,which regularly monitors contaminants in water treatment chemicals says in this year’s NSF Fact sheet on fluoridation:
“In summary, the majority of fluoridation products as a class, based on NSF test results, do not contribute measurable amounts of arsenic, lead, other heavy metals, radionuclides, to the drinking water.”
And the NZ Waste Water Association’s report says:
“Commercially available hydrofluorosilicic acid, sodium fluoride and sodium silicofluoride are not known to contribute significant quantities of contaminants that adversely affect the potability of drinking water.”
Brown, Cornwall & McPhee, 2004 say in their review paper, Trace contaminants in water treatment chemicals: sources and fate:
“ Coagulant chemicals are the main source of trace metal contamination in water treatment.”
4: Some people seem to think that simply quoting concentration of contaminant species is proof of contamination – irrespective of the actual magnitudes. I have seen speakers flash up a slide listing heavy metal contents without bringing notice to the actual concentrations. That is silly. Our environment, no matter how “natural,” will always contain some amount of contaminant chemicals – it is the actual amount that is important – not that it can be, or is, measured.
Arsenic in community water supplies
Paul raises the problem of arsenic and this provides an opportunity to put the contaminants in fluorosilicic acid into context. The table shows that As levels are typically very low in fluorosilicic acid used for water treatment (0.4 ppm As). In my article “Hamilton – the water is the problem, not the fluoride! “ I show that in the local Hamilton, New Zealand, situation the source water from the Waikato River is the major source of As in the finished water – several orders of magnitude greater than for than from treatment chemicals.
Anti-fluoridationists often rely on a recent paper by Hirzy et al. (2013) for their claims about As in fluoroslicic acid and it’s effect on the incidence of cancer. Hirzy has since acknowledged errors in his calculations and described himself as embarrassed by them and his mistake about cancers. A petition to the EPA which used his data to argue against use of fluorosilicic acid in water treatment was rejected partly because of these errors (see Anti-fluoridation study flawed – petition rejected).
Fluoridation data around the world
Connett’s point 9: Yes, a few countries do not fluoridate their water community supplies for political reasons, but decisions against water fluoridation can depend on a range of factors including size and centrality of water treatment plants, widespread use of bottled water, naturally sufficient water fluoride concentrations, etc.
Paul refers to a plot used by Cheng et al (2007) – which is similar to this one:

This and similar plots are much beloved but anti-fluoridation propagandists. But while the plots do show improvements in oral health for countries irrespective of fluoridation they say nothing about the effect of fluoride. Simple comparison of countries obscures all sorts of effects such as differences in culture, history, social and political policies, etc. Such plots are also influenced by changes and differences in dental treatment and measurement techniques.
However, there are some within country data within the WHO data set Cheng et al used which can give a better idea of the beneficial effects of fluoridation. This plot shows the results for the WHO data for Ireland. A clear sign that fluoridation has played a beneficial role.

Political and scientific arenas.
Connett’s point 10: The debates around fluoridation involve both scientific and political issues. Inevitably this leads to the separate issues being mixed. I find, for example, that attempts to discuss the ethical aspects always get diverted into differences in understanding of the science. For example the paper Ethics of Artificial Water Fluoridation in Australia by Niyi Awofeso is meant to be a description of the ethical issues. However, it assumes mistaken ideas about the science – that fluorosilicate species are present in fluoridated drinking water. Without the correct science it is so easy to end up with invalid ethics.
Appeal to authority is also a problem. Connett does this, for example, in his reference to Prof. James Summer, Nobel prize winner. Similarly wild claims are often made about Nobel prize winners and “top scientists” opposing community water fluoridation – these are really not valid arguments.
I feel that opponents of fluoridation commonly rely more on confirmation bias than critical and objective assessment when referring to the scientific literature.
There is also a reliance on conspiracy theories and poisoning of the well. We have seen personal attacks on scientists and health authorities in New Zealand when they have spoken up to defend the science. Childish name calling, accusations of being paid to make incorrect claims, charges of being “shills” for industry, etc. This is simply “playing the man and not the ball” and makes good faith discussion of the science impossible.
This even gets into peer-reviewed scientific literature. The authors of the paper Connett refers to, Cheng et al 2007, do this when they accused one side, that of health authorities, of “questionable objectivity.” Pots and kettles?
All of these problems are probably inevitable for an issue like this where political and ideological interests operate. But they are an anathema to proper scientific consideration.
Professor Gluckman, the NZ Prime Ministers Chief advisor on Science commented that fluoridation controversies were an example of science being a proxy for values/political issues. This leads to misrepresentation of the science, cherry picking of data, and relying on confirmation bias and google for literature searches. Ideology and values are the motivating factors but a caricature of science is used in the debate.
Good faith discussion of the scientific issue around fluoridation requires much more objectivity than is usually demonstrated by the opponents of fluoridation.
Anyone wanting to follow the debate and/or check back over previous articles in the debate can find the list of articles at Fluoride Debate.
See also:
Similar articles on fluoridation
Making sense of fluoride Facebook page








Pingback: Fluoride debate Part 1: Connett | Open Parachute
Ken . . . your graph of DMFT for Ireland shows both lines falling at about the same rate . . . which indicates more that fluoride has not had any effect . . . well it does according to the statistics I learned anyway . . . :}
LikeLike
Tricia, the difference between the lines (about 0.7 I think) is the effect of fluoridation. The declines in both the lines with time demonstrates that there are other independent effects.
LikeLike
Ken . . . please think again . . . if there is a difference to start with and it doesn’t change then whatever has been added has had NO EFFECT!
LikeLike
Correct me if I am wrong, Trica, but didn’t fluoridation in Ireland start well before 1984 where the first point in the graph is? Early 1960s or before?
>
LikeLike
Mark Petersen, you comment was abusive so has been sent to spam. Please note the points in comment moderation made in the introduction https://openparachute.wordpress.com/2013/10/29/the-fluoride-debate-introduction/
You are welcome to submit your comment in a civil form but continued abusiveness will lead to automatic sending to spam.
LikeLike
Well you would need to start the tale back there with those 2 populations and show the improvement . . . as it stands the fluoridated population started better off and haven’t improved any more than the non-fluoridated population.
If you compare that with the NZ year 8 % caries-free data from 1999 to 2010 you will find a greater improvement in the non-fluoridated children which suggests that not only is fluoride not effective but actually inhibits healthy dentition.
LikeLike
Tricia – where is your evidence that the non-fluoridation population “started better off” at the beginning of fluoridation? I don’t think you are correct – and if you were then there is some explaining to do. Why should that particular group be “better off?”
I have compared the fluoridated and non-fluoridated data for NZ from 2002-2011 (no ethnic data was collected before 2002). See my articles Fluoridation – it does reduce tooth decay and Cherry picking fluoridation data.
LikeLike
Tricia – there is a clear and consistent difference between the unfluoridated areas and the fluoridated areas in the Irish data (which was disguised in Cheng’s figure). If you deny that is due to fluoridation then how do you explain it?
LikeLike
If rates of fluorosis are nearly the same in fluoridated and non-fluoridated communities, wouldn’t that indicate that people in communities without fluoridation are already getting enough (and sometimes too much) fluoride in their diet from other sources?
LikeLike
There is concern that some people may be getting excessive F by intake from sources other than water. One possibility is from eating toothpaste.
However, as we don’t see any cases pf severe fluorosis this is probably not too common. Some of the anti-fluoridation opposition relies on the data for “questionable” grade fluorosis.
However, if there were other dietary sources that everyone was using and these were adequate that would be an argument against the necessity of fluoridation of water supplies. I don’t think that is the case yet and the apparent decrease of dental differences between fluoridated and unfluoridated areas probably has more to do with mobility and the “halo effect.” The introduction of the” hub and spoke” model for school dental clinic in NZ from 2004 could be an example of this.
>
LikeLike
Ken . . . your graphs say it all . . . . can’t you see it? Maori fluoridated % caries free have actually dropped in the fluoridated and risen in the non-fluoridated so at 5 years there is virtually no difference.
At year 8 the gap has narrowed from 2002 to 2011 exactly as I said indicating that teeth in non-fluoirdated areas have improved MORE than those in fluoridated regions . . . again I suggest that indicates that not only is artificial fluoridation ineffective in preventing tooth decay but could actually inhibit healthy dentition.
You can try to explain it away with your hubs and halos but this is exactly what Dr John Colquhoun BDS DipEd MPhil PhD, Honorary Research Fellow, University of Auckland, Former Principal Dental Officer, Department of Health, Auckland, revealed after travelling the world in search of evidence that artificial fluoridation was working, only to find exactly what these graphs reveal, that the rates of decay were falling just as fast, and in many cases faster in non-fluoridated regions.
I don’t understand how you can possibly keep denying the evidence before your eyes, graphed by yourself presumably, just as I did after realising what a devastating effect the artificially fluoridated Auckland tap water had had on me for the previous 35 years, and going straight to the only source of data that appears to be available in NZ on the Min of Health’s web site.
Thank you for confirming that my graphing efforts were accurate – presuming that yours are too – now take a VERY GOOD LOOK!
LikeLike
Perhaps you should present you own graphs and analysis, Trisha – I don’t think your conclusions are warranted with the data I have presented.
The apparent closing of the gap in recent years, if it is real, is easily explained by the mobility of children and the mixing of those from unfluoridated and unfluoridated areas encouraged by introduction of the “hub and spoke model” of dental clinics from 2004 onwards. Unfortinately this is the sort of thing that happens with epidemiological data – they must always be approached intelligently and critically – not just to confirm biases.
You have done nothing to explain the large differences between children from fluoridated and unfluoridated areas of the whole period – it is a diversion to concentrate just on the last few years, especially as the halo effect easily explains it.
I suggest you take the hard look, but look at all the data, try to explain the consistent differences between children from fluoridated and unfluoridated areas, and avoid latching on to just a few data points to avoid those issues.
LikeLike
…but this is exactly what Dr John Colquhoun BDS DipEd MPhil PhD, Honorary Research Fellow, University of Auckland, Former Principal Dental Officer, Department of Health, Auckland, revealed….
Good grief. What a mouthful. Diploma of Education? Masters of Philosophy?
What the…
No. That won’t do.
9. Climate Change – Meet the Scientists
LikeLike
How about we use the New Zealand Medicines Act (1983) or the Canadian Food and Drugs Act definition?
“Meaning of medicine, new medicine, prescription medicine, and restricted medicine
(1) Subject to subsection (2), in this Act, unless the context otherwise requires, the term medicine means any substance or article, other than a medical device, that is manufactured, imported, sold, or supplied wholly or principally — (a) for administering to 1 or more human beings for a therapeutic purpose; or…” – New Zealand Medicines Act (1983)
Just in case you forgot what therapeutic meant…
Definition of THERAPEUTIC
1: of or relating to the treatment of disease or disorders by remedial agents or methods
2: curative, medicinal
– Merriam Webster Medical Dictionary
“”Drug” includes any substance or mixture of substances manufactured, sold or represented for use in the diagnosis, treatment, mitigation or prevention of a disease, disorder or abnormal physical state, or its symptoms, in human beings or animals…” – Canadian Food and Drugs Act
“… we can classify the two major oral health conditions – periodontal (gum) disease and dental caries [cavities](tooth decay) – as both chronic and systemic diseases.” – Public Health Agency of Canada, Chronic Diseases in Canada Volume 30, no. 4, September 2010
If fluoride looks like a drug, swims like a drug and quacks like a drug…
…then it is obviously is a drug. Ken, fluoridation agents qualify as drugs according to the Canadian Food and Drugs Act. If fluoride looks like a drug, swims like a drug and quacks like a drug… …then it obviously is a drug. This is their “drug” definition and they classify dental caries (cavities) as both chronic and systemic diseases yet fail to acknowledge the obvious as you do. Ken do you know what a duck looks like?
LikeLike
Myles, I think you illustrate the problem I referred to. You have cobbled together definitions from different sources and locations to justify an argument up which is preconceived. Legislation in each jurisdiction must be consistent, one can’t suddenly switch countries to justify a position.
The very fact that countries like Canada and New Zealand do not include F at fluoridation levels in their definitions of medicine shows the flaw.
And then again, given the reality of the chemistry and low risks involved why should they? legislation has to be realistic and workable – even if it doesn’t satisfy your own ideological or political our purposes.
And enough of the ducks.
LikeLike
@ Myles26
Whatever.
As Ken says it’s semantics.
Water “cures” thirst.
Food “prevents the abnormal physical state, or its symptoms, in human beings or animals”, known as malnutrition.
Both are drugs I take daily.
LikeLike
I calling fowl.
LikeLike
Yes Cedric . . . shows that John was a well rounded scholar, and a gentleman who had the courage of his convictions to stand up to the health bullies of the day . . . a true whistle blower that got rewarded with early retirement on a reduced pension.
LikeLike
This is the point I was making in the last section of my article, Tricia. Appeal to authority and qualifications are not evidence or argument. They are a fallacy. Similarly applying titles and honourifics/qualifications to people on only one side of the discussion is not credible evidence. Nor is it appropriate to advance conspiracy theories, labelling people (bullies), etc.
If the anti-fluoridationists have a scientific or ethical case they should make it – not report to such fallacies.
I really want to avoid the discussion deteriorating into such pointless and irrelevant claims. >
LikeLike
Yes Cedric . . . shows that John was a well rounded scholar…
Oh what gullible bullshit you spout.
You’re touting a logical fallacy.
Just because you are bedazzled by some guy with letters after his name, it doesn’t send a thrill up my leg.
Oooh!! Err!! He’s got a Phd in basket weaving.
So what?
In science, only the work counts.
Science Works! How the Scientific Peer Review Process works
LikeLike
Funny how Ken allows such blatant rudeness from pro-fluoridationists but puts anything like the rubbish you just spouted in the spam file from anyone else . . . :{
LikeLike
Tricia, don’t have an attack of the vapours. I implore you.
We are all out of smelling salts around here.
Loosen the laces on your girdle.
Oh and your bullshit is still worthless bullshit.
I’m not the one with the logical fallacy. You are.
LikeLike
So why do you put up Professor Gluckman with another load of derogatory comments regarding people who disagree with your views?
When you point your finger Ken remember there are 3 fingers pointing back at you.
You have failed to answer my valid points but instead resort to rudeness and ridicule.
You say that the halo and hubs explain the graphs but to me it smacks of the same manipulation of data that occurred in the Napier / Hastings experiment where the control was dropped because it was performing better and then the method of reporting was changed to get the desired result.
The simple fact is that rates of tooth decay have fallen just as much, and in many cases more, in non-fluoridated areas as in artificially fluoridated ones.
Dr Colquhoun’s qualifications are entirely relevant because they are impeccable and rather than dismiss his findings as conspiracy theories it would add to the discussion if you looked seriously at his revelations concerning the reduction in tooth decay right across the board which fell dramatically from 1930 to 1940 and continued to steadily decline right through to the present day without any noticeable effect from the introduction of artificial fluoridation from the 1950’s;
until the present day where the difference between fluoridated and non-fluoridated communities have become statistically insignificant.
I consider the use of the term ‘bullies’ to be entirely appropriate given that rather than seriously investigate the situation he revealed ‘health authorities’ put him into early retirement with a reduced pension.
What term would you use then?
LikeLike
Ken are you going to continues to allow Cedric to be rude and insulting?
You considered Mark Petersen’s comments to be unacceptable but I consider Cedric’s to be far more personal and not addressing the arguments at all . . . please explain.
LikeLike
I consider Cedric’s to be far more personal and not addressing the arguments at all . . . please explain.
Tricia, it’s nothing personal. It’s your argument.
It’s bullshit. Gullible bullshit.
Dr Colquhoun’s qualifications are entirely relevant because they are impeccable…
Babble. How exactly does “impeccible” translate into “relevent”?
Speak English.
A Phd in basket weaving may be completely impeccible but…doesn’t mean it’s at all relevent.
You are committing a logical fallacy. There’s no getting around that.
Fallacies: Appeal to Authority
LikeLike
I’m confused about why the comments aren’t being moderated. This is not helpful for people who were hoping for a scientific discussion. Ken, could you explain more clearly what the rules are for commenting? For example, it would be helpful to hear an explanation from Cedric for why the arguments presented by Trisha are illogical, rather than simply classifying them as “gullible bullshit”. Let’s look at the arguments on their merits.
LikeLike
For example, it would be helpful to hear an explanation from Cedric for why the arguments presented by Trisha are illogical,…
Let me break it down for you in simple steps.
You can wear a nice hat. A very nice hat.
Yet you can be completely wrong about the advice you give on cancer treatments.
Even, and I want to make it very clear, if you really do have a nice hat.
You can have a B.A….or an MBA…or a dozen Phds. All from Oxford.
Yet you can be completely wrong.
Being bedazzled by the baubles on the end of someone’s name is really bad thinking.
Conmen do this trick all the time.
Tricia said…”You can try to explain it away with your hubs and halos but this is exactly what Dr John Colquhoun BDS DipEd MPhil PhD, Honorary Research Fellow, University of Auckland, Former Principal Dental Officer, Department of Health, Auckland, revealed…”
The idea is that you are supposed to be awed by this.
The BDS, the Diploma of Education, the Masters of Philosophy etc, etc.
Trust this man. Look at his baubles!!!!
It’s bullshit.
It’s a logical fallacy.
“…shows that John was a well rounded scholar, and a gentleman who had the courage of his convictions to stand up to the health bullies of the day . . . a true whistle blower..
Tricia decided to dig the hole deeper.
He’s not just a scholar. Oh no. He’s a well rounded scholar.
Did she say scholar? Sure but he’s also a gentleman.
With courage of conviction. A whistle blower.
Are you in awe yet?
Can she ladle on any more sugar?
It’s a stupid argument.
There’s even a name for it.
It’s called a faulty appeal to authority.
I didn’t make it up. You can google it for yourself and see that there really is this thing called a faulty appeal to authority.
Tricia is making one. In spades.
Faulty Appeal to Authority
LikeLike
Ken, is there a place where you have laid out the “case FOR fluoridation” in a comprehensive way? In other words, rather than an overview of the inconsistencies of the anti-fluoride argument, what is the detailed argument that convinced you of the safety and efficacy of fluoridation? Or maybe others can point out what they believe is the “best case for fluoridation”, such as a detailed review of the literature…
LikeLike
Cedric, what convinced you? I agree with your wariness of appeals to authority; would you mind sharing where I could find the comprehensive argument that convinced you? What I mostly hear from people is an appeal to the endorsements of authoritative medical and dental organizations.
LikeLike
I agree with your wariness of appeals to authority…
To be precise, a faulty appeal to authority.
That is….Tricia’s faulty appeal to authority.
Not just vague appeals.
Tricia’s.
Hers.
What I mostly hear from people is an appeal to the endorsements of authoritative medical and dental organizations.
Do you understand why that’s different?
(Hint: The videos)
LikeLike
How about you start with an agreed upon ” terms and definitions” of words to avoid obfuscation and enhance clarity? I’ll start if I may?
Fluorosilicates…anthropogenic compounds containing fluoride used to fluoridate treated drinking water.
Get the idea…?
LikeLike
Ok, fine, Cedric. I’m really not concerned with dissecting Trisha’s point. I’m asking you or whomever else wants to chime in, where can one find a high quality, comprehensive argument supporting fluoridation? What convinced you? Or are you undecided?
LikeLike
No idea why my original post is coloured blue half way down. It was not like that initially. Anyways, I submitted a couple of definitions and could have added the united states Food, Drug and Cosmetics Act aswell in showing that even by their own definitions and classifications, fluoride qualifies as a drug/medicine regardless of which country you’re in. The acts all say the same thing. Fluoride used for/in the therapeutic/treatment/diagnosis/mitigation or prevention of a disease is a drug or medicine. So no Ken I did not illustrate a problem that you referred to. I illustrated a problem of the proponents not acknowledging by their own definitions and classifications fluoridation agents being drugs/medicine.
@ Richard Christie
“Whatever.
As Ken says it’s semantics.
Water “cures” thirst.
Food “prevents the abnormal physical state, or its symptoms, in human beings or animals”, known as malnutrition.
Both are drugs I take daily.”
You sure do make a strong argument there Christie. “whatever”?
Oh Ken said it’s semantics so it must be semantics yet we have clear definitions all saying the same thing. Fluoridation chemicals are drugs/medicine. Love your definition too. “Water “cures” thirst. Food “prevents the abnormal physical state, or it’s symptoms in human beings or animals”, know as mulnutrition.” So “thirst and hunger” are diseases according to Christie. Wow. Christie I think you should review what a disease is before you submit this one to Websters or Merriam’s.
LikeLike
Alison
Start with a good, modern textbook of epidemiology or dentistry. Read the chapters on fluoridation. Check out the references.
You will then have a good baseline from which to investigate more recent peer reviewed articles.
Asking for a single review article is asking someone else to cherry pick. That is not appropriate in science and isn’t going to be done.
If you want to understand the arguments, both pro and anti, you have to do the reading yourself.
LikeLike
The point about the “drug” argument is that the term is used by fluoride opponents as if the simple labeling of a mineral as being a “drug” somehow instantly transforms it into a negative, all of a sudden invoking claims of “forced medication”, “informed consent”, “uncontrolled dosages”, and the like. The fact is, as Ken has pointed out already, that fluoride added to a system to supplement the existing level, is identical to that which already exists in water. A fluoride ion is a fluoride ion regardless of its source. So, when fluoridation opponents fail to express the same concerns of “forced medication”, “uncontrolled dosages”, etc., about the existing fluoride ions in water, they are clearly demonstrating that that their objections have nothing to do with concerns of fluoride being a “drug”, but are simply the same objections that are grounded in personal ideologies as have been around since the inception of this public initiative 68 years ago. Any valid fears or concerns for health in regard to the miniscule few parts per million fluoride ions added to raise the existing level to 0.7 ppm, would also be expressed for the identical fluoride ions which already exist in water. That they are not, exposes the fallacy of attempting to use semantics to condemn this beneficial public health initiative.
Steven D. Slott, DDS
LikeLike
Could we please avoid the personal one on one bitching? The little exchange between Cedric and Tricia really adds nothing – it’s a diversion.
So far I have only has to remove one comment because it was abusive. I think both Cedric and Tricia have valuable points to make and have not been abusive so at this stage I will just encourage them to get back on track.
Alison, unfortunately while I am sleeping I really can’t do anything about moderation, short of holding all comments for approval. Don’t want to do that yet – but may have to.
I will respond to your request for my motivation in supporting fluoridation later.
LikeLike
Yes, Stuart. Thank you. Could you suggest a textbook? I have read through the CDC’s stuff and a number of government reviews. I’ve also accessed some peer reviewed journals and various articles, but I’m not sure I’ve seen the things that others consider to be most convincing. I’ve also reviewed the newspaper articles in my town back from back in 1969 when we approved fluoridation and the case was laid out for doing so. Most of the things that were said are no longer true. Most people felt that the primary benefit was systemic, that fluoride tablets were too expensive, and that fluoride was an essential nutrient in the same category as iodide. So I’m wondering what Ken or you or anyone views as the most convincing overview (whether that be an entire textbook, a list of articles, etc). I agree there are a number of problems with the anti-fluoride stuff and the people can be very extreme with a poor understanding of the math and units of measurement, but reading through Paul Connett’s articles, and some of his book, it doesn’t seem to fit into the conspiracy theorist category. I am a 29 year old mother of two young children and I grew up with a mixture of some fluoridated but mostly non-fluoridated water… I started with no real bias one way or another and I don’t believe fluoride has damaged my health in any way, but I’m also not sure it’s necessary anymore considering that I do know plenty of people who are self conscious about what appears to be mild dental fluorosis.
LikeLike
Alison, here but a few of the peer-reviewed articles which demonstrate the effectiveness of water fluoridation. I’ll be glad to provide more if anyone would like.
1). http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2925001/
Results
Children from every age group had greater caries prevalence and more caries experience in areas with negligible fluoride concentrations in the water (<0.3 parts per million [ppm]) than in optimally fluoridated areas (≥0.7 ppm). Controlling for child age, residential location, and SES, deciduous and permanent caries experience was 28.7% and 31.6% higher, respectively, in low-fluoride areas compared with optimally fluoridated areas. The odds ratios for higher caries prevalence in areas with negligible fluoride compared with optimal fluoride were 1.34 (95% confidence interval [CI] 1.29, 1.39) and 1.24 (95% CI 1.21, 1.28) in the deciduous and permanent dentitions, respectively.
——Community Effectiveness of Public Water Fluoridation in Reducing Children's Dental Disease
Jason Mathew Armfield, PhD
2) http://www.ncbi.nlm.nih.gov/pubmed/23550501
CONCLUSIONS:
Children with severe dental caries had statistically significantly lower numbers of lesions if they lived in a fluoridated area. The lower treatment need in such high-risk children has important implications for publicly-funded dental care.
——Community Dent Health. 2013 Mar;30(1):15-8.
Fluoridation and dental caries severity in young children treated under general anaesthesia: an analysis of treatment records in a 10-year case series.
Kamel MS, Thomson WM, Drummond BK.
Source
Department of Oral Sciences, Sir John Walsh Research Institute, School of Dentistry, The University of Otago, Dunedin, New Zealand.
3). http://www.ncbi.nlm.nih.gov/pubmed/23488212
CONCLUSIONS:
The survey provides further evidence of the effectiveness in reducing dental caries experience up to 16 years of age. The extra intricacies involved in using the Percentage Lifetime Exposure method did not provide much more information when compared to the simpler Estimated Fluoridation Status method.
—–Community Dent Health. 2012 Dec;29(4):293-6.
Caries status in 16 year-olds with varying exposure to water fluoridation in Ireland.
Mullen J, McGaffin J, Farvardin N, Brightman S, Haire C, Freeman R.
Source
Health Service Executive, Sligo, Republic of Ireland. joej.mullen@hse.ie
4) http://www.ncbi.nlm.nih.gov/pubmed/8500120
Abstract
The effectiveness of fluoridation has been documented by observational and interventional studies for over 50 years. Data are available from 113 studies in 23 countries. The modal reduction in DMFT values for primary teeth was 40-49% and 50-59% for permanent teeth. The pattern of caries now occurring in fluoride and low-fluoride areas in 15- to 16-year-old children illustrates the impact of water fluoridation on first and second molars.
—-Caries Res. 1993;27 Suppl 1:2-8.
Efficacy of preventive agents for dental caries. Systemic fluorides: water fluoridation.
Murray JJ.
Source
Department of Child Dental Health, Dental School, University of Newcastle upon Tyne, UK.
5). http://www.ncbi.nlm.nih.gov/pubmed/23252588
CONCLUSIONS:
Data showed a significant decrease in dental caries across the entire country, with an average reduction of 25% occurring every 5 years. General trends indicated that a reduction in DMFT index values occurred over time, that a further reduction in DMFT index values occurred when a municipality fluoridated its water supply, and mean DMFT index values were lower in larger than in smaller municipalities.
—-Int Dent J. 2012 Dec;62(6):308-14. doi: 10.1111/j.1875-595x.2012.00124.x.
Decline in dental caries among 12-year-old children in Brazil, 1980-2005.
Lauris JR, da Silva Bastos R, de Magalhaes Bastos JR.
Source
Department of Paediatric Dentistry, University of São Paulo, Bauru, São Paulo, Brazil. jrlauris@fob.usp.br
Steven D.Slott, DDS
LikeLike
Tricia, qualifications do not trump evidence. But consider this, if you want to use Colquhoun’s qualifications then you are morally obliged to also refer to the qualifications of others, including those you disparage. If you wish to use titles for Colquhin, isn’t it disrespectful not the use titles for me? If you respect Colquhin’s arguments because of his degrees, then you should give the same respect to my own arguments because of my degrees.
Far safer to ignore the titles and qualifications and deal with the evidence. That is what happens in the scientific community where titles only get used in formal situations.
I can understand why you use Colquhoun’s arguments as he places the same interpretation on the improving oral health irrespective of fluoridation you do, but he also ignores, or tries to, the clear evidence of differences in oral health between fluoridated unfluoridated communities as you do. If you cannot explain why there is a difference between the unfluoridated and fluoridated Irish data then you have a problem relying on the original graph that Cheng, Connett and many others do which uses the averaged Irish data.
Similarly use of terms like bullying and reliance io conspiracy theory is another way of avoiding evidence. Why not stop diverting this way and deal with the actual evidence?
My reference to Gluckman’s comment has nothing to do with his title or position, just the simple truth of his comment. Very often activists use a distorted and selective version of the science because they are ideologically driven. They are using science as a proxy for their values/political arguments. Far better, and more honest, to accept the science, stop distorting it, and argue the ethical/values/political case instead.
Now, I do not know what points of yours I have failed to answer. Perhaps you should review my comments to see if in fact you have missed something. If I have not responded to a specific point let me know what it is and I will do so.
>
LikeLike
Glad we have cleared up that little matter of qualifications and ‘authority’ and I will no longerbe subjected to ‘Professor Gluckman says . . . . . “etc . . . :}
LikeLike
@myles26
Love your definition too. “Water “cures” thirst. Food “prevents the abnormal physical state, or it’s symptoms in human beings or animals”, know as mulnutrition.” So “thirst and hunger” are diseases according to Christie. Wow.
They are your definitions Myles.
You offered them.
Not me.
Own them.
I’m pleased you can see how weak your argument was.
LikeLike
So back to the science. Any basic textbook on biochemistry will identify the fluoride ion as an inhibitor of enzyme activity and particularly of a crucial step in the Krebb’s or Citric Acid cycle.
Before I waste any more of my time may I ask – Do you agree?
LikeLike
Alison, it has been my experience in a long career of research (I am now retired) that single papers or books do not have the influence you imply. Or if they do it is because one is immature or naive and therefore open for changing ones view as one learns more.
Most of my research has been in soil chemistry so I have been aware for a long time of the important role F plays in apatites, hardening them and lowering their solubility. So the beneficial role of fluoridation has never been a surprise to me – it kept on being reinforced as I learned more about apatites in soils. And about the efficacy of rock phosphates as fertilisers and the surface reactions inhibiting their solubility.
One road to Damascus moment did come when I did some research in fluorosilic acid 10 years ago and my analysis of the material showed concentrations of contaminant heavy metals to be very low. Until then I had believed contamination was a problem with the chemical. This fact made me realise there were some porkies being told in this fluoridation debate and since then I have always checked out the claims made by the anti people. Often finding them completely wrong – dishonestly so.
Similarly in the biochemical claims I have actually checked out the original papers where possible and become aware that studies done with relatively high concentrations of F were dishonestly being used to argue cases about low concentrations.
All this material must be approached critically and intelligently with account being taken of concentrations, conditions and so on. Unfortunately the anti people so not do this. They are armed only with confirmation bias and cherry pick studies which they then distort to support their argument. I find that jars with the scientific ethos.
>
LikeLike
It would be very helpful if commenters would stay focused on that which is relevant to fluoride at the concentration of 0.7 ppm. Presenting arguments based on fluoride without regard to concentration levels is meaningless. All substances are toxic at improper levels. At what concentration of fluoride, for instance, does Tricia have concerns about inhibition of enzyme activity? Is there valid, peer-reviewed evidence of enzyme inhibition by fluoride at 0.7 ppm about which she has concerns?
Steven D. Slott, DDS
LikeLike
Tricia, could you give a citation (and link if possible) and let us know at what concentration F acts as a specific enzyme inhibitor? I am not doubting your claim, just want to look at the details (where the devil resides). 🙂
LikeLike
Andy, I have sent your comment to spam – it was entirely unrelated to the post or discussion and aimed only at causing trouble.
LikeLike
Peter Van Caulart, as a chemist fluorosilicate has a specific meaning to me which is not covered by your definition. Why not just use the chemically acceptable definitions for terms? I do not think there is any reason for people to be confused about fluorosilicate – especially as it can easily be checked.
LikeLike
Christie, I didn’t offer up any definitions of my own. I clearly quoted and sourced drug/medicine definitions from the New Zealand Medicine and Canadian Food and Drug Acts. These countries and others have defined what a drug/medicine is. These same organizations who have defined drugs/medicine also classify caries (cavities) as a systemic and chronic disease. I pointed out the obvious which is fluoridation agents qualify as drugs/medicines under their own definitions and classifications. Again, just in case you missed it, “their definitions”, not mine. You can own up to your ridiculous definition and I will continue to point out that fluoridation agents qualify as drugs/medicine according to the various health organizations own definitions and classifications. Proponents understand that if they acknowledged fluoridation agents were drugs/medicine then they would not pass the rigourous scrutiny that other drugs/medine go through. As fluoridation agents stand, they do not pass the scientific/legal determination of safety. So big surprise here you are trying to obfuscate the meaning of the definitions.
LikeLike
@Myles26.
You offered the definitions.
When the same were applied to other substances you scream and mock the use of the definitions.
Using your definitions (or, if that description makes you unhappy, the definitions that you supplied), in the manner I did merely illustrates the irrelevancy of this avenue of argument.
Definitions change. Definitions differ upon who makes them.
The action of fluoride doesn’t change. The salient issue is whether fluoridation is safe and beneficial as a public health measure.
Ken’s post made reference to bait and switch tactic. Your use of definitions and your subsequent insistence upon subsequently applying testing standards developed for manufactured drugs, rather than those for environmental trace elements is case in point.
Wikipedia states that iodine deficiency affects 2 billion people worldwide and that fully two thirds of the world’s population enjoy the use of iodized table salt. This *drug* administered in their food helps supply the recommended daily intake of 1.1mg . Wikipedia: The lethal dose [iodine] for an adult human is 30 mg/kg, which is about 2.1–2.4 grams Toxic chemicals/drugs administered to foodstuffs or a re-balancing of dietary trace element?
LikeLike
You state Ken that It is easy to cite literature references showing negative effects of fluoride but we should not ignore the conditions used. Most such studies refer to much higher concentrations than used in water fluoridation and this is also true for the review by Barbier et al, 2010 Connett cites.
Let’s not forget that community water fluoridation describes “topping up” fluoride concentrations to about 0.7 ppm F. Yet reviews of negative effects on biochemical process will quote studies which have used 50 ppm, 100 ppm or even greater concentration of F in drinking water. Opponents of fluoridation often seem completely oblivious of these huge differences in concentration when they present a long list of claims about the ill effects of fluoridation.
Here are some studies using low levels of fluoride showing harm, let’s not forget all sources of fluoride consumed each day! Please Ken refute these studies below:
A study by Procter and Gamble showed that as little as half the amount of fluoride used to fluoridate public water supplies resulted in a sizable and significant increase in genetic damage. It is generally accepted that if a substance can induce genetic damage there is a heightened risk that it could cause cancer as well. Even minute doses of 1 ppm of fluoride could prevent essential biological reactions from taking place. Proctor & Gamble, makers of Crest toothpaste also found that 1 ppm of fluoride could cause genetic damage in Chinese hamsters’ ovary cells. The lowest dose of fluoride inducing genetic damage in human white blood cells was found to be 0.6 ppm which is below the level we currently fluoridate at. In science there are margins of safety, for an adverse affect such as the one listed above it was found that fluoride caused genetic damage in human white blood cells at 0.6 ppm so a margin of safety would be to divide the dose by 10 to protect people from the adverse effect so the margin of safety would be 0.06 ppm to protect the public.
A study by Ellise Bassin showed a correlation between osteosarcoma a rare bone cancer and water fluoridation. People with osteosarcoma usually need amputation, and it can lead to death.
In 1991 a UNICEF funded research team in china found that humans with iodine deficiencies may be affected by fluoride levels as low as 0.9 ppm. Fluoride also is used to treat people with hyperthyroidism and it is no wonder that so many people in fluoridating countries have hypothyroidism. Margin of safety for this adverse effect would be 0.09 ppm.
A study by Masters and Coplan showed that children living in fluoridated areas using inorganic fluoride chemicals namely hydrofluosilicic acid and silicofluorides have higher levels of lead in their bloodstream.
Fluoridated water should not be used or added to infant formula, foods, or drinks intended for babies 12 months of age or younger in order to avoid dental fluorosis. Fluoride can cross the blood brain barrier which can cause lower iq and behavioral problems in children.
Hip fractures were caused inadvertently in a study designed to prove fluoride prevented osteoporosis. In the trials elderly women were given 75 mg per day of sodium fluoride and compared to a control group. The study ended abruptly with the horrifying discovery that fluoride caused these fractures. In light of this study another study looked at low levels of fluoride in drinking water at the optimal level of 1 ppm. Hip fractures were 27% higher in women and 41% higher in men living in Brigham City, the largest fluoridated community in Utah, compared to non-fluoridated Logan and Cedar City. These studies were verified in five additional studies including the French study (JAMA 1995; 273:775) that showed an 86% increase in hip fractures in fluoridated communities. Additionally, Toronto which has been fluoridated for 35 years has twice the hip fractures as Quebec which has never been fluoridated.
In 2009, the Iowa researchers published the long-awaited data on the effect of total fluoride exposure on tooth health after 9 years of the children’s life. Much to the disappointment of fluoridation advocates, daily fluoride intake was found to be significantly associated with dental fluorosis, but not tooth decay.
The lack of effect between fluoride intake and tooth decay can be visually seen in the above figure that the authors published, which shows that children with no cavities have ingested almost identical amounts of fluoride at each year of life as children with cavities. According to the authors:
“These findings suggest that achieving a caries-free status may have relatively little to do with fluoride intake, while fluorosis is clearly more dependent on fluoride intake.” (Warren 2006)
LikeLike
Also Ken as you state most such studies refer to much higher concentrations than used in water fluoridation, why aren’t more studies done at 0.7ppm for each and every health effect that is mentioned? Without these studies being done you cannot just say fluoride is safe because studies are done at higher levels.
LikeLike
Trevor, many of the studies do include a low concentration of F – mainly 0. But the effects generally only show at high concentrations.
It is straw clutching to say that because no effects were seen at low concentrations, or reported at low concentrations, that things aren’t safe. Science doesn’t work that way – it attempts to find the situations which are unsafe.
LikeLike
Trevor, your comment is composed of extensive copy and paste – for example much from this article “The Dangers of Fluoride and Fluoridation”
In future I will send such comments to spam as they are disrespectful – you are doing no work for yourself yet you expect others to answer you. That is not the sort of discussion I want here. It is disrespectful and only demonstrates you are not able to put a cogent argument together by yourself.
I will not respond to your copypasta at the moment, Trevor – but if you genuinely want to discuss the issues then provide the citations (and links if possible) to the articles you refer to. I am happy to read such studies – they might even convince me to change my mind. But copypasta won’t.
Other commenters be warned – extensive copy and paste is disrespectful and will be treated as spam.
LikeLike
In my province of Manitoba the law states: WHEREAS Manitoba law recognizes that mentally capable individuals have the right to consent or refuse to consent to medical treatment;
AND WHEREAS this right should also be respected after individuals are no longer able to participate in decisions respecting their medical treatment;
“treatment” means anything that is done for a therapeutic, preventive, palliative, diagnostic, cosmetic or other health-related purpose, and includes a course of treatment. (« traitement »)
Since fluoride is used for a preventing tooth decay would make it a medical treatment.
http://web2.gov.mb.ca/laws/statutes/ccsm/h027e.php
LikeLike
As Paul Connett states on his website regarding iq studies there have been iq reductions at levels of 0.88ppm among children with iodine deficiencies. Also Ding 2011 shows iq reductions at 0.3-3ppm. When you calculate the margin of safety it is below the “optimal” 0.7ppm fluoride concentration. Do you think that the fluoride levels should be reduced then to protect people from these health effects?
http://fluoridealert.org/studies/brain01/
LikeLike
Thank you, Ken, for the sincere, helpful response…. and with regard to the comments, I’m sorry… I forgot about the time difference, as I am in the United States. I agree, best not to make all comments wait for moderation, if possible. I’m looking forward to the continued debate.
LikeLike
At the link below shows fluoride is a drug: http://napra.ca/pages/Schedules/Search.aspx
LikeLike
Here is another link showing fluoride is a new unapproved drug according to Health Canada http://www.hc-sc.gc.ca/dhp-mps/prodpharma/applic-demande/guide-ld/newdrug-drognouv/ndrugs_ndrogue-eng.php
LikeLike
For example, it would be helpful to hear an explanation from Cedric for why the arguments presented by Trisha are illogical,…
(…but then later…)
Ok, fine, Cedric. I’m really not concerned with dissecting Trisha’s point.
How extraordinary.
LikeLike
You state Ken: Perhaps we can agree that F is at least a beneficial element, even if we can’t reach agreement on the use of terms like “nutrient” and “essential.” I think that fluoride may be a beneficial element for certain industrial processes and things in that nature perhaps but I am in the opinion that fluoride is not beneficial for any health related purpose including preventing tooth decay. Fluoride is definitely not a nutrient as no disease occurs from deficiency of it Weston Price studied many indigenous tribes and found diet plays a major role in tooth decay. In British Columbia they have the best tooth decay rates in all of Canada and they are mostly unfluoridated there. Dr. Gray was former chief dental officer in BC Canada and was fired when he released his study revealing the fact that unfluoridated areas have less cavities. A.S. Gray, Canadian Dental Association Journal, October 1987, pp. 763.
Dr. Colquhoun in New Zealand was fired as well after he published his results showing the unfluoridated areas have better teeth.
A study by the New York State Department of Health, showed after 50 years of fluoridating Newburgh’s children had more cavities and more fluorosis than never-fluoridated Kingston.
New Studies cast doubt on fluoridation benefits,” by Bette Hileman, Chemical & Engineering News. Vol 67, No. 19, May 8,1989).
LikeLike
Trevor, you claim that John Colquhoun was “fired” from his position. However, he actually retired as Principal Dental Officer in the Auckland department of Health in 1984 – according to the tribute on his death in Fluoride 32: 134-136 1999. He was the. Editor of Fluoride, the anti-fluoridation journal. No mention of him being fired.
Did you make that up, Trevor?
LikeLike
Might Trevor interpret the WHO graph in Ken’s post for us please.
Specifically interested in the 0.7 DMFT difference between the two curves.
LikeLike
(… for the Irish data.)
LikeLike
I didn’t make it up Ken it is on this article from Gary Null. http://www.tldp.com/issue/157-8/157fluor.htm Source for that part says it is from 31. Gary Null interview with Dr. John Lee, 3/10/95.
LikeLike
Yes, I offered the definitions. Glad we got that straightened out. Much happier now. I never screamed. I don’t understand how you percieved that when I did not use any punctiation marks in my previous post. I did mock your silly definition though. You illustrated nothing other than you don’t understand the definitions set out by your health authority or any other health authority for that matter. Yes definitions change but we’re not talking about old definitions, we’re talking about current definitions set out by the authorities. These drug/medicine definitions are relevant because the same people who created these definitions, classify cavities as a systemic and chronic disease and don’t acknowledge that fluoridation chemicals qualify as a drug under their own definitions are the same people who endorse water fluoridation. I agree with you on your point of the importance of whether fluoridation chemicals are a safe and beneficial health practice but would also add ethical to your list. The ethicality of water fluoridation is the most blatantly obvious issue of water fluoridation. Let’s not forget that one. You are abosolutely right about more safety studies needing to be conducted, no argument here but if the authorities/proponents refuse to acknowledge that fluoridation chemicals are drugs/medicine when they obviously are according to their own definitions then the process of properly scrutinizing the safety, ethicality and benefit or detriment is hindered. You said it yourself, we need to understand whether this stuff is safe and beneficial or not. Well let’s start by acknowledging that fluoridation chemicals and are in fact drugs/medicine according to the definitions set out by the New Zealand Medicine Act and Canadian Food and Drug Act. Why are we so afraid to acknowledge the the blatantly obvious? What would be the harm in acknowledging that fluoridation chemicals are drugs/medicine? If you could address any one point, commnet or question of mine could you please address this one. What would be the harm in classifying fluoridation agents as drugs/medicine?
P.S. Have no idea why you mention iodine. We’re talking about fluoridation chemicals. Did wikipedia mention anything about how many people suffer from fluoride deficiency around the world? I’m guessing probably not because you can’t be deficient in something that is not essential. Canada acknowledged fluoride is not an essential nutrient back in 1990.
LikeLike
Dr. Gray was former chief dental officer in BC Canada and was fired
…Dr. Colquhoun in New Zealand was fired as well
Conspiracy alert.
LikeLike
Dr. William Marcus was fired as well over the fluoride cancer study but was reinstated after winning his lawsuit. Phyllis Mullenix was fired also over her work on fluoride and the brain. The WHO graph in Ken’s post 0.7 DMFT difference between the two curves could be from any confounding factor. Canadian studies done by the government show that when fluoride was removed from towns in BC decay rates improved and fluorosis went down as well.
LikeLike
As Myles mentioned fluoride violates our right to informed consent which is why certain countries and cities have ended the practice. Fluoridation is unethical. in Calgary Alberta this is one of the main reasons why they stopped fluoridation there. Water should not be used as a delivery method for drugs. There are more countries that do not fluoridate than countries that do. More studies do need to be conducted especially at least one randomized double blind cinical trial that proves fluoride is safe and effective. Also As the York Review noted: “No randomised controlled trials of the effects of water fluoridation were found. . . . None of the included studies were of evidence level A. The reason for this among the studies evaluating dental caries was that none addressed three or more confounding factors.”
LikeLike
You illustrated nothing other than you don’t understand the definitions set out by your health authority or any other health authority for that matter.
It’s simple Myles. I’ll walk you through it.
I took the test as offered in the definition supplied by you
“”Drug” includes any substance or mixture of substances manufactured, sold or represented for use in the diagnosis, treatment, mitigation or prevention of a disease, disorder or abnormal physical state, or its symptoms, in human beings or animals…” – Canadian Food and Drugs Act
Now, the “disease, disorder, abnormal state” part, well, that’s where I tested for “malnutrition”. It being an abnormal physical state, maybe even a disorder.
Then the “substance or mixture of substances” for “treatment, mitigation or prevention” part, that’s where I tested for eating food.
And the result was that food is consistent with the definition’s test for a drug.
Yes, it’s trivial. And so is the insistence upon calling fluoridation the administration of a drug when concentrations in water supplies are simply adjusted to a level which is common within the environment and is beneficial to dental health.
The only reason you insist on this is to subsequently demand tests are applied in the same manner as applied to other newly discovered (usually) and manufactured drugs with unknown effects. Fluoride does not fit into that category. Fluoride in a naturally occurring trace element with safe, beneficial action on human when ingested at optimal concentrations.
Have no idea why you mention iodine.
Because it is highly toxic at higher concentrations and beneficial at lower ones. Because I don’t hear complaints that its mass administration is outrageous and that it be classified as a dangerous drug.
Did wikipedia mention anything about how many people suffer from fluoride deficiency around the world?
No, but plenty of mention about how fluoridation has been a successful public heath measure in the reduction of dental caries.
To which
LikeLike
http://www.youtube.com/watch?v=ouu6Iuv1KRs&feature=youtu.be I found the interview of Dr. Lee with Dr. Gary Null talking about Dr. John Colquhoun, Dr. Gray and Dr. Marcus being fired it is around 6 minutes into the video.
LikeLike
Only calcium fluoride occurs naturally which is not the type of fluoride that is added to most cities water supply and calcium fluoride is not as water soluble as say sodium fluoride so it is more easily excreted from our system. Sodium fluoride is very water soluble. With Iodine you have a choice if you want to take it or not it is up to you whereas fluoride you cannot really avoid it if it is added to the water supply. You don’t have to buy iodized salt if you do not want it that is why people do not complain about it. Iodine as well is an essential nutrient whereas fluoride is not. Just because something is natural as well does not make it safe. Everything is toxic pretty much at some level, even too much water can kill you. People should have the right to chose. The fluoridating agents in most water supplies are a lot more toxic than naturally occurring calcium fluoride that is why a lot of people are against them. These chemicals do not react the same in our bodies and form other fluoride species. Also the fluoridation chemicals added to the water can leach more lead from lead pipes, read the research by Roger D. Masters on this topic.
LikeLike
The optimal fluoridation dose when it was first started was 1 ppm a day now it is 0.7ppm why the change? It was thought that only 10% of children would get fluorosis at this dosage. Fluorosis is not normal and the first sign you are getting too much fluoride I think an optimal dose would be one that does not cause any fluorosis at all in any child.
LikeLike
Clearly fluoride can be:
A natural mineral
A mineral nutrient
A water additive
An over the counter medication
A prescription medication
An industrial chemical
An industrial pollutant
A fumigant
A rat poison
All of these are true and there are important, critical distinctions between each use, each concentration, and the purity standards which define the various incarnations of “fluoride.”
The willful refusal to acknowledge these clear and easily understood distinctions is an important element in anti-fluoridation propaganda.
LikeLike
OMG! OMG!!! OMG!!!1111!!1!!!!!11!!!!
They’re putting rat poison in our water. The fiends. Those dastardly fiends.
LikeLike
Trevor, as Ken stated, you need to provide proper cites for the studies you wish him to evaluate such that they may be read in their complete and proper context. I can, however, respond to a couple of the studies with which I am familiar.
First, the Bassin study is the one which Connett has “cherry-picked” to further his claim of association of cancer to water fluoridation. He still does this in spite of the overwhelming consensus of valid science that there is no such association. Here is what Chester Douglass has to say:
Chester Douglass, principal investigator of the Harvard Study, advises readers to be cautious when interpreting the [Bassin] findings, noting the following reasons:
• The preliminary findings from the overall analysis of the cases identified between 1993 and 2000 (second set of cases) do not show an association between osteosarcoma and fluoride in drinking water.
– The cases had been identified from the same hospitals within the same orthopaedic departments and the same pathology departments diagnosing osteosarcoma, and similar methods of fluoride exposure
Bone specimens were also provided by many of the cases – preliminary analysis of bone specimens suggests fluoride level in the bone is not associated with osteosarcoma.
The 1990 NIEHS National toxicology Program study found an association with high levels of fluoride in drinking water and osteosarcoma in male rats. However, the findings of their second study did not find an association.
Some of the limitations noted by Bassin et al in their paper include:
The estimates of fluoride in drinking water at each residence do not reflect the actual consumption of fluoride.
The study did no obtain biologic markers for fluoride uptake in bone.
The actual amount of fluoride in a fluoridated supply may vary (within guideline levels).
Natural fluoride levels can vary over time (the researchers thought this unlikely for the time spent at each residence).
There is a lack of data on other potential confounders.
Fluoride may not be causative agent
– another factor in drinking water may be correlated with the presence of fluoride.
Data to assess fluoride exposure from diet, industrial sources of other sources such as pesticides was not available – cases may have been exposed to other unknown factors such as contaminants or carcinogens in the bottled or well water, with the fluoride in these products or natural sources irrelevant, regardless of the concentration.
——-Douglass, C.W. and K. Joshipura, Caution needed in fluoride and osteosarcoma study. Cancer Causes Control, 2006(17): p.481-482
Masters and Coplans’ attempt to correlate increased lead uptake with water fluoridation, was completely refuted by Urbansky and Schock.
“Overall, we conclude that no credible evidence exists to show that water fluoridation has any quantitatable effects on the solubility, bioavailability, bio- accumulation, or reactivity of lead(0) or lead(I1) compounds. The governing factors are the concentrations of a number of other species, such as (bi)carbonate, hydroxide, or chloride, whose effects far exceed those of fluoride or fiuorosilicates under drinking water conditions.”
—–Can Fluoridation Affect Lead (II) In Potable Water? Hexafluorosilicate and Fluoride Equilibria In Aqueous Solution
Urbansky, E.T., Schocks, M.R.
Intern. J . Environ. Studies, 2O00, Voi. 57. pp. 597-637
If you provide proper cites for your studies, I will be happy to address them as an adjunct to any information Ken may provide. In the meantime, what I have provided at least gives you an idea of the fallacy of the out-of-context information you copy from antifluoridationist websites.
Steven D. Slott, DDS
LikeLike
Trevor, here is some of the peer-reviewed science which Connett ignores when he attempts to use Bassin to further his claim of association of fluoridation with cancer:
A review of worldwide studies by The International Agency for Research on Cancer (IARC) concluded there was no evidence of an increase in cancer rates associated with fluoride in drinking water.
——International Agency for Research on Cancer, IARC Mondographs on the Evaluation of Carcinogenic Risks of Chemicals to Humans, Volume 27. 1982
• The San Francisco Department of Public HealthOccupational Health and Environmental Health Section states that within a search of relevant peer reviewed medical literature to September 2005, a total of seven (7) epidemiological studies were discovered, none of which showed a relationship between fluoride exposure and osteosarcoma
—— (Moss et al. 1995, Gelberg et al. 1995, Freni and Gaylor 1992, Grandjean et al. 1992, McGuire et al. 1991, Mahoney et al. 1991, Hrudey et al. 1990).
——San Francisco Department of Public Health, Current Scientific Evidence: Water Fluoridation is not associated with osteosarcoma. 2005, http://www.sfdph.org/phes/ water/fluoride/Osteosarcoma_fluoride fact_sheet.pdf
Three small case control studies of osteosarcoma (McGuire et al 1995, Gelberg et al 1995, Moss et al 1995) have been reviewed by the Australian National Health and Medical Research Council in 1999. None of these studies found any evidence of fluoride increasing the risk of osteosarcoma.
——-Ahokas, J., et al., Review of water fluoridation and fluoride intake from discretionary fluoride supplements: review for NHMRC. 1999. Available at http//www. nhmrc.gov.au/advice/pdfcover/fluocov. htm, Royal Melbourne Institute of Technology and Monash University: Melbourne.
The York Review (2000), a systematic review of 214 studies of varying quality, found no clear association between fluoridation of water and osteosarcoma.
——-McDonagh M S, et al., Systemic review of water fluoridation. BMJ, 2000. 321.
A study by Hoover et al found no relationship between osteosarcoma and fluoridation. This study is important because of the large numbers involved (125,000 incident cancers, and 2.3 million cancer deaths).
——Medical Research Council Working Group, Water fluoridation and health. 2002, Medical Research Council: United Kingdom.
In 2002 the British Medical Research Council agreed that overall, evidence does not suggest that artificially fluoridated water increase the risk of cancer.
——-Medical Research Council Working Group, Water fluoridation and health. 2002, Medical Research Council: United Kingdom.
A review of fluoride by the Scientific Panel on Dietetic Products, Nutrition and Allergies published by the European Food Safety Authority in 2005, found no increased risk of cancer from drinking fluoridated water.
——European Food Safety Authority, Opinion of the Scientific Panel on Dietetic products, Nutrition and Allergies on a request from the Commission related to the Tolerable Upper Intake Level of Fluoride. The EFSA Journal, 2005. 192: p. 1-65.
Steven D. Slott, DDS
LikeLike
What you’ve given Steve is a good run down on how much uncertainty there is surrounding the true picture and effects of fluoride and as such it should not be put in the public water supply.
LikeLike
Wouldn’t it be good if there was a study conducted to find out just how many people are adversely affected by drinking artificially fluoridated water – easy to do – and then determine why? Obviously if the initial survey found more than one person then the practice should cease immediately until the facts of the matter are unravelled.
LikeLike
These studies are happening all the time. At the moment, Tricia, the only credible evidence of negative effects of fluoridation is an increase in questionable and mild fluorosis. This is not considered at all harmful and extremely minor compared with the known benefits of fluoridat for oral health.
LikeLike
Sorry Ken – the only studies being done are on teeth and when someone like me comes along who suddenly finds that most of her health problems disappear when she stops drinking artificially fluoridated tap water NO ONE WANTS TO KNOW!
The implications are actually staggering considering the number of falls in older people, which is the major cause of hip fractures, 25% of which are fatal in the overs 65 year olds: and considering I no longer have to hang on for grim death in the shower for fear of losing my balance when I close my eyes to wash my face as I used to when drinking the tap water.
That is just one of a dozen complaints that have cleared up since I stopped drinking Auckland’s fluoridated tap water in October last year.
The GP, WaterCare, DHB, Min.of H Auckland Council, nor even the National Poisons Centre were not interested at all to even try to find out what was causing my problems and are therefore presumably quite happy for this to continue when thousands may be similarly affected to varying degrees.
Your graphs show that the so called ‘benefits of fluoride are highly questionable and don’t you think that the people with fluorosis even should have been asked whether they wanted to risk this disfigurement for the sake of 0.6 of one tooth surface when fluoride tablets are cheap and readily available for those who do want them?
LikeLike
Tricia, it is difficult to see how the peer-reviewed studies I cited in my previous comment could be interpreted as in any manner demonstrating “uncertainty”. However, you do provide an excellent example of how fluoride opponents twist scientific evidence to attempt to create “controversy” where none exists. This evidence makes clear the overwhelming scientific consensus that there is no correlation between water fluoridated at 0.7 ppm and cancer. There is no valid evidence that contradicts this.
Going on a “fishing expedition” in an attempt to find adverse effects of water fluoridation is not how science works. In order to demand proof that there is not a problem, there must first be reasonable evidence that one exists. There is no valid evidence of adverse effects of water fluoridated at 0.7 ppm. The only substances ingested as a result of fluoridating with HFA are fluoride ions identical to those which exist in water “naturally” and trace contaminants in barely detectible concentrations that fall far short of EPA mandated maximum levels of safety. When demanding test after test of water fluoridation, you are simply demanding testing of the fluoride ion which people have been ingesting since the beginning of time, and trace contaminants in trace concentrations which are harmless.
Steven D. Slott, DDS
LikeLike
Tricia, your health problems are unfortunate, but provide only anecdotal information. The placebo effect is probably the most accurate explanation for why your symptoms abated when you ceased drinking fluoridated water.
The only dental fluorosis which may occur in any way attributable to water fluoridated at 0.7 ppm is mild to very mild. This effect is barely detectable except by close examination by a dental professional, and has no adverse effect on cosmetics, form, function, or overall health of teeth. As Kumar, et al, have demonstrated mildly fluorosed teeth to be more decay resistant, mild dental fluorosis is considered by many to not even be undesirable, much less adverse. Nonetheless, for those parents who do not desire to risk even mild dental fluorosis in their children, in spite of the decay preventive benefit, the ADA and the CDC have suggested they use non fluoridated water to reconstitute powdered infant formula, or simply use premixed formula, most, if not all, of which is produced utilizing low fluoride content water.
—–http://jada.ada.org/content/140/7/855.long
The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren
Hiroko Iida, DDS, MPH and Jayanth V. Kumar, DDS, MPH
Steven D. Slott, DDS
LikeLike
Tricia, I think you have a strange understanding of the nature of scientific research. Personal anecdotal evidence is not scientific. But there has been research on the sort of personal phenomena you report which indicates it is basically all in the mind. For example there is a Finnish study where residents were misinformed about the date that fluoridation ceased in a town. Lo and behold the reported symptoms persisted even though fluoridation had already been stopped but citizens had not been told. And only disappeared when citizens were later informed that fluoridation had ceased! See Fluoride sensitivity – all in the mind?
As for hip fractures have a look at my article The hip fracture deception.
The graphs I presented are clearly consistent wih the beneficial role of F on oral health – I think your persistent denial of this is an example of confirmation bias and evidence selection on your part.
There seems to be a real determination on the part of anti-fluoridationists to misinterpret the scientific data, to use selective citations, and to actually misrepresent what the science is finding.
LikeLike
The funniest story of confirmation bias that I’ve read is the antifluoridationist tale of the race horses in Kentucky, or somewhere, that the owner was convinced had died of fluoride poisoning. She states that she had been told by 8 vets, including one affiliated with a university, who had examined her horses both when they were sick, and after they had died, that their cause of death was not fluoride related. She finally found a vet who had apparently written some pieces on fluoride poisoning, to whom she related the symptoms her horses had exhibited, or at least her perception of what the symptoms had been. This vet told her that the symptoms she described were consistent with fluoride poisoning. That’s all she needed! The previous 8 vets were, of course, all “incompetent”, with the final one very much “enlightened”, and the only one who had really understood the problem. This tale can probably be found on Google.
Steven D. Slott, DDS
LikeLike
Trevor, the Chinese studies that Connett uses to bolster his IQ claims are so flawed as to not warrant serious consideration. He finds one or two studies which seem to support his opinions, and ignores the volumes of peer-reviewed science which refute them. As far as fluoride effects on iodine, here is the opinion of a respected endocrinologist from the University of Florida:
August 27, 2013
To Whom It May Concern:
As a practicing endocrinologist, I was appalled at the claims that fluoridated drinking water causes clinically significant harm to the endocrine system.
Clinically, in more than 30 years of seeing patients, I have never seen any fractures or thyroid problems associated with fluoridated water. Early puberty is more associated with obesity than anything else, though there are many endocrine disrupters that have estrogenic effect. Fluoride has not been implicated, though lavender, tea tree oil and HCG, substances found commonly in hair products, have been.
I looked at the papers cited about the effects of fluoride on thyroid function and could find none that suggested any effect on thyroid at doses used in fluoridated water. A Review of the literature published in 1986 came to the same conclusion:
“The increasing use of fluoride for prevention of dental caries poses the problem as to whether this halogen has antagonistic properties towards iodine, whereby it could hamper the success of iodine prophylaxis of endemic goitre. Review of the literature shows that some authors have found an inhibition by fluoride of various steps of thyroid hormone biosynthesis in animal experiments. By and large, the inhibition was only slight and it was elicited only with fluoride doses greatly in excess of those recommended for caries prevention. The inhibition was not consistently present and other authors could not confirm it in comparable experiments. There is no convincing evidence that fluoride produces true goitres with epithelial hyperplasia in experimental animals. There are some reports based on casual observations that fluoride is goitrogenic in man. On the other hand, several good studies with adequate exposed and control populations failed to detect any goitrogenic effect of fluoride in man. It is noteworthy in particular that fluoride does not potentiate the consequences of iodine deficiency in populations with a borderline or low iodine intake.Published data failed to support the view that fluoride, in doses recommended for caries prevention, adversely affects the thyroid.”
I hope this clarifies the issues a bit more.
Sincerely,
Janet Silverstein, MD, FAAP
Steven D. Slott, DDS
LikeLike
Steve, I notice Janet Silverstein’s letter is very recent. Is a link available on the Internet yet?
LikeLike
Not to my knowledge, Ken, but I’ll see if I can arrange that.
LikeLike
Tricia, I also have a balance and dizziness problem, am in the age of concern range and conscious of the risk of falls and hip fracture. Actually my balance problems seems to have got a lot worse in the last few months – ever since Hamilton stopped fluoridation! Perhaps it’s the lack of F which causes it. 🙂 It’s been a bit of a mystery but I have concluded it was caused by inner ear damage from use of an antibiotic 20 years ago. That is the problem with anecdotal evidence – it can be used to support any claim.
LikeLike
. . . Oh great Steve DDS . . . why did Auckland’s fluoridated tap water make me so sick then?
LikeLike
…and when someone like me comes along who suddenly finds that most of her health problems disappear when she stops drinking artificially fluoridated tap water NO ONE WANTS TO KNOW!
Clearly, it’s all part of a larger conspiracy. You have the scientific community on the run and you know it. Or not.
The plural of anecdote is not data.
The Problem with Anecdotes by QualiaSoup
LikeLike
You are very arrogant to say:
‘Tricia, your health problems are unfortunate, but provide only anecdotal information. The placebo effect is probably the most accurate explanation for why your symptoms abated when you ceased drinking fluoridated water.’
I note dental fluorosis on a regular basis here in Auckland and I would not wish to have that either . . . even if you and all your learned colleagues told me it was ‘barely detectable except by close examination by a dental professional’ . . . I can spot it and no doubt those who have it wish they didn’t.
LikeLike
Scott has a go…..”Tricia, your health problems are unfortunate, but provide only anecdotal information. The placebo effect is probably the most accurate explanation for why your symptoms abated when you ceased drinking fluoridated water.”
Ken has a go….”Tricia, I think you have a strange understanding of the nature of scientific research. Personal anecdotal evidence is not scientific. But there has been research on the sort of personal phenomena you report which indicates it is basically all in the mind.”
Sadly, Tricia does not compute…
. . Oh great Steve DDS . . . why did Auckland’s fluoridated tap water make me so sick then?
How extraordinary.
LikeLike
Aukland’s fluoridated water did not make you sick, Tricia. Your perception of this is merely a placebo effect.
Steven D. Slott, DDS
LikeLike
Ken, the Finnish study only further proves that the fluoride industrial waste in the water was the cause of the reported symptoms.
Without assistance of black coffee enemas (arabica, not robusta), vitamin C mega-doses and/or crystal therapy the absorbed fluoride toxin takes at least a month to get flushed from the body and skeletal structures. Hence continued reports of illness after the poison was withdrawn from the supply.
You can’t fool us.
/satire
LikeLike
You are very arrogant to say:
Exactly what part was arrogant?
‘Tricia, your health problems are unfortunate
Was Scott being arrogant when he called your health problems unfortunate?
Surely not.
..but provide only anecdotal information.
Was Scott being arrogant when he pointed out you provided only anecdotal evidence?
(..re-reads what Tricia originally wrote…)
Nope. That was just a reality-based statement.
You really did only provide anecdotal evidence.
Nothing very arrogant there.
I note dental fluorosis…
Welcome to Anecdote City. Enjoy your stay.
LikeLike
I think you have a strange understanding of science Ken if you truly believe that personal anecdotal evidence is not ‘scientific’. Most scientific investigations have started through personal experiences where people seek to find out more and unravel the causes and effects . . . like what made the apple fall?
You have a rather bizarre interpretation of the Finnish study also and don’t appear to be able to look objectively at data at all.
When I stopped drinking Auckland’s artificially fluoridated tap water, and I changed nothing else, I had 12 complaints disappear, many of which have serious implications for the population as a whole and for the health budget in particular.
The dental fraternity have been shown to be the ones misrepresenting the data and in fact manipulating it outrageously, as Colquhoun and Mann have documented. On what do you base your claims? They sound merely a matter of opinion rather than documented fact as the instruction to change the way the dental nurses recorded the data in the Napier/Hastings experiment.
LikeLike
Well, Tricia, such is the mindset of fluoride opponents. When the science is presented to them, they simply deny it. This is clear demonstration that your objection has nothing to do with science. It is all grounded in personal ideology.
Steven D. Slott, DDS
LikeLike
Sounds pretty much like my experience of trying to find someone who will get to the bottom of why Auckland’s artificially fluoridated tap water has made me so sick for 35 years . . . only I’m still waiting . . . :{
LikeLike
If your mind is closed you won’t see anything that contradicts your beliefs Janet.
LikeLike
I find that very interesting Ken because that is exactly the symptoms that got worse before they got better and I can only assume that once the constant burden of fluoride was relieved and my body started to get rid of the accumulations of it that somehow the balance mechanisms registered it – they are very sensitive apparatus.
LikeLike
Sure, Tricia, one can start with anecdotal or personal evidence. But it is unscientific to stop there. One thing a research scientists has to learn to be any good is that they are often wrong. And they find that out by experiencing the evidence. This is very often the case at the start of an investigation when one has only personal or anecdotal experience. It is testing one’s ideas against reality which sorts out the mistakes. In my own career I often felt that when I discovered that Iw as worng, because of evidence, that it6 was a breakthrough because it enabled me to build a better model of what I was looking at.
AS for your 12 complaints – well go ahead and publish the data – did you take good records? And what do you think of my problem? – my balance problems have got worse since fluoridation stopped. Will you include that in your anecdotal evidence?
Tell me – in what way have I misinterpreted the Finnish study – especially as my perception as the same as the authors’ conclusions.
Both Mann and Colquhoun were ideologically driven and therefore their story, by itself, cannot be trusted. Even I was aware of a general change of dental procedures at the time – that I why I always raise it as one of the causes of the apparent improvement in oral health. Such “operator” effects are a trap that researchers always have to be aware of. But of course, if it confirms you own bias you can see it as a conspiracy.
It is a hell of charge to claim that “the dental fraternit6y” are misrepresenting the data – another conspiracy theory perhaps.
LikeLike
So, Tricia, are you saying that my worsening balance symptoms are actually caused by fluoride, even though fluoridation stopped months ago? Interesting bit of mental gymnastics – but I will keep an open mind to see what happens over the next few months, and if there are any changes when fluoridation restarts.
Personally I think the evidenced of an effect of a specific antibiotic on my inner ear is more compelling. Not that I lose any sleep over it these days.
LikeLike
As I said before you are so arrogant – I know what happened when I stopped drinking Auckland’s artificially fluoridated tap water for you to dismiss this as placebo is yet another example of not being able to see anything that challenges your pet theories because you mind is closed . . . probably sclerosed from drinking too much fluoridated tap water?
LikeLike
I think you have a strange understanding of science Ken if you truly believe that personal anecdotal evidence is not ‘scientific’.
Google it and stop behaving like an idiot.
Going “LALALALALALALALALALA” is not appropriate behaviour.
Google “Science” and then “anecdotes” or “anecdotal evidence”.
He’s not making it up all by himself.
The plural of anecdote is not data.
Honest.
…and when someone like me comes along who suddenly finds that most of her health problems disappear when she stops drinking artificially fluoridated tap water NO ONE WANTS TO KNOW!
(…)
. . . why did Auckland’s fluoridated tap water make me so sick then?
(…)
I note dental fluorosis on a regular basis here in Auckland and I
(…)
I can spot it and no doubt those who have it wish they didn’t.
(…)
When I stopped drinking Auckland’s artificially fluoridated tap water, and I changed nothing else, I had 12 complaints disappear…
Anecdote City. Some people stay….forever.
Michael Shermer: Baloney Detection Kit
LikeLike
Tricia, provide valid, documented medical evidence that your problems were caused by water fluoridation and you might have an argument. Anecdotes and opinion may seem real enough to you, but they are meaningless without valid evidence to support them. Accepted science has standards that must be met. This is the fact that fluoride opponents….including, somewhat surprisingly, Connett, himself……..do not seem to understand.
Steven D. Slott, DDS
LikeLike
Any true scientist would be wary of any ‘evidence’ that conflicts with clearly observed fact . . . unless their professional ideology precluded it of course.
LikeLike
What is a “clearly observed fact” Tricia? Was Galileo wrong to rely on his empirical evidence when he supported a heliocentric solar system, while the church relied on the “clearly observed fact” that the sun went around the earth? Because of their ideology?
How do we know what might be factual without collecting evidence? Humans are well known for confirmation bias and selective vision – without objective evidence we are continually making mistakes.
LikeLike
And Tricia, will you please refrain from accusations of arrogance. It is not arrogant to ask for evidence and to draw conclusions based on the evidence. If you can’t provide evidence then you have the problem, not others.
LikeLike
Not mental gymnastics at all . . . I have often observed symptoms getting worse before they get better as the body tries to clear up the problem and is given an appropriate stimulus.
Your problems may very well be from the antibiotic – I wouldn’t presume to make such a call as Steve obviously feels free to do with my experience: and I am impressed that you intend to keep an open mind and see what happens – as I have done throughout my saga.
A wee bit of investigation would go a long way to help though as the lady in Havelock North who found that her blood levels of fluoride were 250% higher than desirable after persuading her GP to test for it – she now drives 20 minutes to get water safe for her to drink – my GP made the astounding call that since all her staff drink the tap water and none of them are sick, that there was nothing to investigate!
LikeLike
Blood tests for F are a real trap? because the body has no way of regulating blood and plasma F concentrations there is a huge variation throughout the day in values. Any sensible interpretation would require intensive, and expensive, sampling over a reasonable amount of time.
LikeLike
As I have replied to Ken my GP took the outrageous stance that since her staff all drank the fluoridated tap water and none of them were sick that is didn’t warrant further investigation.
It is a bit difficult to get documented medical evidence when medical personnel have such an attitude.
To me it is akin to having diabetes before it was a recognised disease and going to your GP saying that as a baker you had to sample your chocolate cake several times a day but that it you were sure it was making you sick and having her turn around and say that they all ate chocolate cake and were perfectly fine so run away and stop wasting her time.
What you don’t seem to understand is that people are wising up to ‘accepted scientific standards’ and realising that they don’t tell the full story and that they need to be able to make up their own minds about what they choose to eat and drink because they have to live with the consequences . . . not just the ‘scientists’ who will just as quickly change their minds once the ‘latest’ study emerges . . . so I have to mention radium, DDT, thalidomide, even avocados and butter?
LikeLike
Tricia stated You [Ken] have a rather bizarre interpretation of the Finnish study also and don’t appear to be able to look objectively at data at all.
Ken asked in what way have I misinterpreted the Finnish study
Please clear this up for us Tricia.
LikeLike
Perfect example Ken because with Einstein and the theory of relativity etc we now can say that both ‘facts’ are correct depending on the point of observation and we need good science to accommodate the whole picture and not just the narrow focus of one particular discipline.
LikeLike
Steve wasn’t drawing conclusions based on the evidence he was simply dismissing my experiences as placebo – that is supreme arrogance.
LikeLike
So why isn’t that being done?
LikeLike
http://www.youtube.com/watch?v=7TwwNZyRVOA Here is a copy of the video regarding Cathy and Wayne Justus’ horses that were poisoned and harmed from water fluoridation. You will have to stop reading those pro fluoridation sites Scott as they are wrong about Cathy and Wayne Justus’ horses and about fluoride. They were from Pagosa Springs Colorado USA not from Kentucky. She took them to 6 different vets not 8 because none of them knew what was wrong with the horses. She met with Lennart Krook and he diagnosed her horses with Chronic fluoride poisoning. So you are saying Dr. Lennart Krook’s diagnosis was not correct? The horses started having problems ever since they started fluoridating the water supply. When she met with city council and the so called experts along with tons of other concerned informed citizens they stopped fluoridating the water supply and her horses symptoms got better, the ones that were still alive that did not die from fluoride.
In the USA Alcoa poisoned alot of cattle and crops and farmers sued them as they vented these dangerous fluordiation chemicals into the air, because of the lawsuits they now have to use wetscrubbers and cannot pollute the air anymore. In Australia alot of kangaroos are being poisoned now because of Alcoa.
Just like Tricia says you guys are so arrogant and think you are right and know everything but you do not. Just like when the fluoride was removed from the water supply in Pagosa springs Cathy Justus’ horses got better and when the fluoride was removed from Auckland Tricia got better as well. Dr. Krook did alot of tests and even published 2 peer reviewed studies about the Justus’ horses.
Pro fluoride reviews and studies are flawed as well and you guys cherry pick your data. Pro fluoridationists manipulated the NTP cancer study and Chester Douglas hid his students work and his recent study did not refute Bassin’s study. You ignore the studies I mentioned showing harm with low levels of fluoride and say the only negative effect is fluorosis. There is no randomized double blind clinical trial showing fluoride is safe or effective and no study that controls for 3 or more confounding factors. Unfluoridated areas have better teeth than fluoridated areas with less fluorosis as well. Fluoride does not help poor children as there are many poor areas with a tooth decay crisis. When fluoride was removed from the water supply cavities did not go up but rather went down and fluorosis went down also.
Kentucky is 100% fluoridated and they have the most toothless people! Fluoride causes tooth decay and does not remedy it. Fluoride is supposed to make teeth stronger but teeth with fluorosis are more prone to cavities and breaking just like bones with too much fluoride. Fluoride is not safe for babies and the water should be safe for all members of the community, since it is not safe for babies and other susceptible individuals fluoridation should be stopped! Weston Price’s studies show that you can be cavity free if you eat properly and do not eat processed food, the people in his studies did not use fluoridated water or fluoridated toothpaste showing fluoride is not necessary, cavities are a modern problem caused by processed foods.
LikeLike
How so, Tricia. I would have thought that Enisteinian relativity conflicted sharply with “clearly observed facts.” That is one reason so many people have trouble understanding it.
We do need good science – and anecdotal claims are not good science. You have done nothing to provide evidence for your claims about the role of F in your problems, nothing at all. At the moment it does look very much like a placebo effect – you noticed an improvement because you knew you had changed your water supply (did you even analyse your new supply for F?).
I get really pissed off with people who avoid a proper investigation and consideration of all the evidence and then call people who do consider the evidence arrogant. It just shows a desire to stick to ones own views despite the evidence. That is not healthy.
LikeLike
Ken, I’m curious if with your background in soil research you might be able to help answer a question I have about fluoride and plants.
From what I have read, it seems that certain plant varieties are quite sensitive to fluoride, depending on a variety of factors. In some cases, experts recommend avoiding the use of fluoridated water, and this doesn’t seem to be controversial at all. If fluoride sensitivity in plants is widely recognized, why is there so much resistance to the suggestion of fluoride sensitivity in certain people?
Here is the link to one of the articles I have read explaining the issue in plants.
http://pnwhandbooks.org/plantdisease/pathogen-articles/nonpathogenic-phenomena/fluorine-toxicity-plants
LikeLike
I think there is a flaw in drawing that parallel because you are comparing differences among different species of plants with differences among individuals of one species as humans. I am aware that F sensitivity occurs for some fish (some salmon for example) but other fish have a high tolerance – a species difference.
Seems like pot plant are most susceptible – then they are to many nutrients depending on feeding and watering conditions.
In general F is strongly bound to Al and Ca in soil, but is often present at higher concentrations in fresh superphosphate – enough to be toxic to animals. It is very unwise to allow animals to graze on freshly fertilised pasture.
So I can see why even fluoridated water would be advised against for sensitive plants in pots, but don’t see any problem in the garden. However, fresh fertiliser could be an issue there.
LikeLike
That’s exactly what I was saying . . . if it had been anything else implicated surely all the people I contacted would have taken it seriously and tried to find out why but as soon as the precious fluoridated tap water was mentioned everyone ran for cover &/or gave the circuitous argument that since the water met the drinking water standards it was safe to drink and couldn’t have made me sick . . . DUH!
I have already mentioned that my lack of balance on closing my eyes in the shower and dizziness actually got worse before they got better and it could be the same for you . . . wouldn’t it be interesting to find out why?
The people who did the Finnish study were no doubt coming from the same ideology as yourself and also failed to appreciate that not all symptoms would respond in the same time, and placebo or not, the fact remains that after 3 months there was a definite, and significant reduction in symptoms.
Furthermore a follow up study some years later showed that dental health had not plummeted as predicted by the fear mongers of the dental fraternity.
If you raised the matter of the change in reporting at the time how come it wasn’t taken into account and the trial declared a failure?
LikeLike
Tricia, you refer to a follow up study – could you please give a reference/citation and or link?
Have no idea what change of reporting you refer to – you have lost me?
LikeLike
By the way, with the Finnish study there were actually 2 groups. One was told about the cessation at the right time and the other a month or two later. The first groups reported their symptoms clearing up, but not the second. The symptoms were a matter of belief, not fact.
This sort of arrangement prevents ones own preferences overriding the facts. It helps objective assessment. That is one reason why such controlled experiments are so much better than relying in anecdotes.
LikeLike
The change in reporting where dental nurses were told to disregard minor decay that previously had been included in the DMFT data.
I will find the reference ASAP . . . or you can look it up using the authors of the original study.
LikeLike
So is it not possible for members of one individual species to differ in their sensitivities to various environmental conditions?
Even plants within a defined species can be affected differently by fluoride depending on calcium content or pH of the soil and/or water.
Might dietary factors in certain populations of people influence the amount of fluoride accumulating in the body?
LikeLike
I must reply further here since you have made a remarkable claim that ‘the body has no way of regulating blood and plasma concentrations and there is a huge variation throughout the day in values..’
I am surprised because my understanding was that despite quite wide variation in the amount of fluoride ingested by mothers that breast milk managed to deliver a consistent very low level of fluoride.
That blood and plasma concentrations can fluctuate so wildly begs the question that therefore concentrations delivered to vital processes, such as the Krebb’s or Citric Acid cycle may be far in excess of the 0.7 ppm?
I believe that latest studies indicate that Latin Americans uptake far more lead than European Americans, in the presence of fluoride: and Afro Americans even more.
So given that these wide fluctuations can occur, and may be influenced by your genetic inheritance, how can scientist truly claim that 0.7ppm is ‘safe’?
LikeLike
Alison, there is not resistance to the suggestion of fluoride sensitivity in humans, there is simply the request for valid evidence of it. Anecdotal information, such as what Tricia has been providing, is not valid evidence. It’s simply like the tale of the racehorses I commented on previously. When people are shown the scientific evidence and deny it, there is little else to be done. This does not mean that medical personnel are covering up anything or that they are incompetent. It simply means that they have provided the valid evidence which contradicts the belief of the person in question, and there is nothing else they can do. In the meantime, that person goes around telling anyone who will listen, that the medical personnel refused to listen, or refused to test properly, or were covering up for self-serving reasons, or whatever, when in reality it was just a matter of the person in question refusing to accept reality, and denying clear scientific evidence to the contrary of that which they believe.
Fluoridation opponents constantly make unsubstantiated claims of this problem or that which they claim to be associated with fluoridated water, then demand there be tests to prove these problems do not exist. Demanding proof of a negative is an endless process as there will always be unsubstantiated claims made by opponents, no matter how many times they are refuted. It’s an endless stalling tactic, and is not scientifically acceptable to do so. Therefore, there must be valid evidence of a problem before there can be legitimate demands to prove there is not one.
Water fluoridation has a 68 year history with no proven adverse effects, in spite of having the most tested public health initiative ever. During that time, were any of the claims made by fluoride opponents to have any validity, there would have been massive outbreaks of these disorders amongst the tens of millions who have ingested fluoridated water. There have not been.
Steven D. Slott, DDS
LikeLike
Sure, it is possible Alison, but I could not say how likely. There are two aspect here.
1: Is the sensitivity genuine? The placebo effect is very real and the Finnish study found that only one of a long list of symptoms were objectively based. They depended on what the person believed about the fluoridation, rather than what actually happened. In such studies a statistically significant result in one parameter of a long list is to be expected by chance.
I am not at all convinced by anecdotal claims from individuals. Sometimes they just come across as hypochondria.
2: If the sensitivity is genuine for a small number of people should that change a social policy? After all people have sensitivities to all sorts of things. Often the only practical solution is that the individual, their family or their support group, make specific arrangements. In our local situation 70% supported fluoridation. If one or two people have a genuine sensitivity then I think it is reasonable to expect them to make other arrangements.
But remember, that unfluoridated water also contains F – in our case it varies from 0.2 or 0.3 to 0.6 ppm. Surely sensitive people are going to have to take some sort of precautions to handle that because it is independent of fluoridation. If symptoms only start appearing with such a small top up then I am suspicious they really are psychosomatic.
LikeLike
Tricia, I am not saying that variability is genetic. That simply because the body does not regulate to maintain a constant concentration of F (maybe because the main benefits occur in inorganic parts) the blood and plasma levels will vary widely depending on time of intake, etc. There may be some rationale in taking samples a specific time after drinking and eating but I suspect it would be safer to take many at several times a day over several days to get a proper picture.
I would not trust people who make claims based on just one or two individual samples.
LikeLike
As you mention Ken fluoridation has been going on for a long time and there is still no randomized double blind clinical trials to prove it is safe and effective. I would like to know your thoughts Ken on the Fluoride Iowa study as fluoride intake did not have an effect on cavitiy rates but did on fluorosis rates?
LikeLike
It’s not me that has avoided a proper investigation Ken it is every ‘health authority’ that I have made contact with and taken my case before. I am the one saying that there should be a thorough investigation into how fluoride may be affecting parts of the body other than just teeth.
As for placebo I know that I bought the bottled water on a whim, because there was a free stand going with 4 bottles at Eric Rush’s New World and I had always tried to avoid the tap water believing that the long term effects could be harmful – hip fractures in particular as one got older and therefore the less I drank of it the better.
However I wasn’t prepared for the dramatic effect it had on my health and well being after just a day or so.
In the previous 35 years I had had various health regimes to try to feel better, and since most of them involved avoiding fluoride I generally succeeded – with organic, raw, 80% fruit and vegetable, macrobiotic, vegetarian, etc:
but this time the only thing I did was switch to Tongariro water.
By the next evening I was sitting in front of TV – as usually by the end of the day I was like a stunned mullet – and suddenly thought ‘Why am I watching this rubbish? I could be doing something useful’.
My energy levels changed dramatically and next time I was standing in a queue at the bank I thought how wonderful it was to not be wishing everyone would hurry up so I could get done and go and lie down.
That had been my mantra for years – get this or that done so I could go and lie down.
Then I realised I no longer ached all over – especially the next morning when I had noticed it more and got into the habit of stretching every part of me I could think of just to rev myself up for the day.
Then I realised that the outsides of my big toes no longer tingled painfully when I did this.
Other things I have noticed are the balance and dizziness as described previously and:
can stoop down to pick things up without discomfort:
can drink as much water as I please without feeling ‘waterlogged’:
the tops of my thighs no longer feel ‘wooden’ – that took about 3-6months to improve and then disappear:
clarity of thought and ability to once again assimilate information with relative ease – this is still not as prolific as it once was – up until 1967 – but there has been a vast improvement.
my hair has grown 2-3 inches after growing to it’s maximum and staying there.
If these sorts of things are happening to even just 1-5% of the population it means thousands of people putting themselves and others at risk and adding a significant burden to the health system – far more than the claimed ‘benefits’ to children’s teeth.
THAT IS NOT HEALTHY!!!!!
LikeLike
Tricia, I can’t understand your obsession with your own case but an anecdotal example for one person is not grounds for extrapolation to the whole population. Especially as the efficacy and safety if fluoridation is so well established.
LikeLike
Oh certainly. I agree. The vast majority of anecdotal claims that I hear sound like Trisha’s… well-meaning and sincere belief, but not scientific, and not compelling. But still, the studies are not really being done to examine the possibility, and the Finnish study was hardly a scientifically conclusive display. One could easily say that some symptoms took longer to diminish, explaining the change, and of course they didn’t follow up with the same survey a year later… Who knows, it may have revealed that all the symptoms continued to decline. Either way, you’d think that with all the effort put into promoting fluoridation, there would be a few more studies examining these issues. A Finnish study from 1997? Are there more out there examining and debunking hypersensitivity?
LikeLike
Trevor, I put you under moderation because of your refusal to provide references and citations, and the extensive copy and paste of your first comment.
You repeat the problem here – of you want my opinion on something for Christ’s sake provide the information. A simple citation, reference and link is not to much to expect. Your “Iowa study” is meaningless to me.
LikeLike
In the following studies from Canada listed below cavity rates went down and so did fluorosis don’t you think that if fluoride was effective at reducing decay the rates would have went up? You can view the entire study data here http://cof-cof.ca/convincing-canadian-studies-demonstrating-water-fluoridations-questionable-merit/
Maupome´et al, Patterns of Dental Caries Following the Cessation of Water Fluoridation Dec 31, 2001
Clark et al, Changes in Dental Fluorosis Following the Cessation of Water Fluoridation Dec 31, 2006
Locker et al, Benefits and Risks of Water Fluoridation – Report to Ontario Ministry of Health & Health Canada Nov 15, 1999
ITO, Caledon and Brampton Study, Peel Region (2757 Determinants of Caries in Adjacent Fluoridated and Non-fluoridated Cities) Mar 21, 2007
Azarpazhooh, Oral Health Consequences of the Cessation of Water Fluoridation in Toronto, MSc Thesis Report, Faculty of Dentistry – University of Toronto, City of Toronto Public Health Aug 31, 2006
LikeLike
By its nature, Alison, there was no possibility of a repeat a year later. There are also ethical restriction on deceiving the public.
But I disagree with your belief it was not conclusive. There was a clear effect of belief on declared symptoms. That is the symptoms corresponded to whether the individuals believed their water was still fluoridated. Not to the actual facts.
I have not particularly followed the hypersensitivity issue – so can’t comment in the availability of other studies. Someone should do a search. However, any sensitivity claims I have seen from anti-fluoridation people have never been backed by evidence and they never advance their own list of studies. They do really come across as hypochondria to me. But I am open to some good evidence.
LikeLike
Ken you can review the Iowa study here http://fluoridealert.org/studies/ifs/
LikeLike
Here is a list on FAN about hypersensitivity to fluoride: http://fluoridealert.org/studies/hypersensitivity03/
LikeLike
That’s rather rude of you to say I have an obsession with my own case Ken. In fact, apart from thinking it’s about time WaterCare provided a fluoride-free supply for those who wanted it if they are going to insist on dumping the toxic waste from the fertiliser factories into Auckland’s water supply; I am ecstatic that I have discovered this major benefit to my health and well being – even if it does cost me dearly to buy a safe supply.
My concern now is that my friends and family, and even the population at large may be being similarly affected without knowing why and therefore being subjected to ever more harmful chemicals:
e.g. my lethargy and brain fag could easily have been interpreted as ‘depression’ and Prozac given – being a fluorinated drug could easily have worsened my condition to the point of suicide?
How many people are driving around with blurred vision, brain fog and crippling fatigue to the point of falling asleep?
How much obesity is related to feeling that all you want to do is lie down the whole time?
The list is endless and from my perspective the society is only as good as how it looks after the worst off amongst us and I feel a responsibility to do all in my power to have it investigated thoroughly – as my GP, WaterCare, DHB, Auckland Council, National Poisons Centre and Ministry of Health should have done.
Of course the ‘efficacy and safety’ of artificial fluoridation will never be challenged if no body is prepared to step outside the comfort of their collegiate mantras . . . fluoride is safe, fluoride is good for teeth etc. . . . and properly investigate.
LikeLike
Don’t forget about people being misdiagnosed with Arthritis when in fact they have skeletal fluorosis Tricia.
LikeLike
I agree. There is a strong case for the vast majority of these symptoms being a case of fluoride induced hypochondria. However, they stopped only one month earlier than the people thought. The was only a small and statistically insignificant difference between December and November in the number of reported symptoms, but a large reduction between November and March. So, it could theoretically be that it took longer than the authors thought it would for the symptoms to disappear. Theoretically.
However, might we also conclude from the study that a highly significant effect may occur on “other skin rashes” for a small portion of the population?
LikeLike
Also, I did not mean “repeat the study”… just administer the survey one additional time to see what people are reporting for symptoms after being fluoride free for one year. Definitely possible, not necessarily worth doing.
LikeLike
Tricia, from your facebook link it appears that you are also anti-vaccination, is that correct?
And you endorse mega doses of vitamin C as a viable medical treatment, is that correct?
This is relevant, because if correct, both stances are strongly contrary to mainstream evidential based scientific, public health and medical recommendations. As is your objection to fluoridation.
Why is Ken’s interpretation of the Finnish study faulty? (again)
LikeLike
I am sorry, Trevor – seems to be difficult to get through to you. Referring to Fluoride Alert is not providing a citation or reference to the “Iowa study.” If you want me to comment you will have to provide reference, citation and/or link to the actual study. If you can’t do that then your comment has been a waste of time.
What this tells me is that you have not even bothered to check the study yourself, you don’t even know what it was about or what it found, you are relying only on Fluoride Alert. That is just not good enough. I am interested in genuine research, not a merry to around of internal citation.
Fluoride Alert is not a reliable source.
LikeLike
Alison, the statistically insignificant differences were between groups who both though the fluoridation had not ended, even though it had in one case. The big difference was between groups who did not know it had appended and who did. Clear indication that belief was the over risking factor – not fluoridation itself.
Yes, there was the skin rash problem where a significant difference was seen irrespective of belief. But, as I said, that could be chance because of the large number of symptoms considered. However, that could be worth investigating further.
LikeLike
Here is a link for you Ken regarding the Iowa study http://onlinelibrary.wiley.com/doi/10.1111/j.1752-7325.2008.00108.x/pdf
LikeLike
Thanks Trevor, if you could only had done that right at the beginning. I will have a read and probably comment tomorrow.
LikeLike
You are welcome Ken, I was not aware of the rules here and how it works.
LikeLike
Any true scientist would be wary of any ‘evidence’ that conflicts with clearly observed fact . . .
That’s correct. For facts.
Now let’s change it to your situation.
“Any true scientist would be wary of any ‘evidence’ that conflicts with my anecdote…”
Yeah, um, no.
I have often observed symptoms getting worse before they get better as the body tries….
The plural of anecdote is not data.
To me it is akin to having diabetes before it was a recognised disease and going to your GP saying that as a baker you had to sample your chocolate cake several times a day but that it you were sure it was making you sick and having her turn around and say that they all ate chocolate cake and were perfectly fine so run away and stop wasting her time.
Ah, I see your problem.
Allow me to translate.
To your GP it is akin to going to your GP saying that you ate/drank “X” several times a day but that you were sure it was making you sick and having her turn around and say that they all ate/drank and sampled “X” several times a day as did everybody else in the community and were perfectly fine so run away and stop wasting her time.
See?
…simply dismissing my experiences as placebo – that is supreme arrogance.
The arrogance comes from you.
Somehow you are superhuman.
Normal observed behaviour somehow doesn’t apply to you.
The possibility that you may be subject to a placebo effect just like anyone else doesn’t register with you.
You have some magical immunity or something.
Now that’s arrogance.
LikeLike
Sorry Charmaine. In the interests of authenticity and genuine open discussion I am not accepting large screeds of copy and paste. Such material is really just a waste of space, interferes with ongoing discussion and no one will bother reading anyhow. We want to encourage a better atmosphere for discussion of this debate.
I suggest you write your comment yourself and resubmit
LikeLike
Tricia, from your facebook link it appears that you are also anti-vaccination, is that correct?
Oh, missed that.
This is relevant, because if correct, both stances are strongly contrary to mainstream evidential based scientific, public health and medical recommendations. As is your objection to fluoridation.
Seconded.
Science isn’t a buffet where you get to pick and choose the science you accept.
Methodology is vital.
The same methodology that would allow you to reject the scientific consensus on the efficacy and safety of vaccines works lovely for rejecting the scientific consensus on climate change or evolution or the moon landings etc..
Science denialism is a thing.
It really happens.
Only the labels are different.
In your case, it’s fluoride. The way you got to where you are with fluoride is very likely the same way you got to where you seem to be with vaccines.
It’s a common pattern.
We see it all the time around these here parts.
When every single scientific community on the planet is telling you one thing and you’re relying on no-name blogs telling you “Nu Uh”, then it pays to double-check your position and make sure you’re not copying the same playbook as the nutters out there.
If you are, then something is very badly wrong.
It inevitably devolves into global scientific conspiracies.
Behold….
Penn & Teller – Anti-Vaccinations Crazies
LikeLike
Trevor, I stand behind my statements on the horse tale. That is the most hilarious example of confirmation bias that I have come across yet. Too, I didn’t read it on a “pro-fluoride site” , whatever that means. It was a link from some antifluoridationist site or another. Your defense of the story makes it all the more funny. Ironic that you ask if I’m questioning the “diagnosis” of the vet who told her what she wanted to hear, apparently based solely on what she told him, after she had rejected the opinions of the other 6, 8, or however many others who had examined her horses and had told her that fluoride poisoning was not the cause of death. That, in itself, is an excellent example of how antifluoridationists reject the volumes of valid evidence which refute their ideology, in favor of the one, dubious piece that they finally find to “support” their belief.
You still fail to cite valid evidence for any of the claims you make. Until you do, they are meaningless.
Steven D. Slott, DDS
LikeLike
Thank you Charmaine that link to Bruce Spittle’s book is invaluable and so well researched there was no reason to not include it Ken.
LikeLike
Tricia, Charmaine is quite welcome to comment here, and refer to Spittle’s book, but as a matter of policy I am moderating to exclude extensive copy and paste. If she has any argument she will make it in her own words. If she hasn’t any argument I guess she won’t come back.
Paul Connett and I agreed that comments on these debate articles will be strongly moderated to prevent the usual abuse and nastiness that seems to accompany this issue. I personally find the extensive copy and pasting of trolls to be offensive. It shows a complete lack of respect for other commenters.
Hopefully we can now return to our original discussion.
I believe someone asked you about your activism in the anti-vaccination movement. Is that true? If so, I think it demonstrates a particular problem the anti-fluoridation people have when it comes to referenda. People will mostly trust the health experts and scientists – after a all they recognise the benefits these experts give to society. But anti-fluoridation activists won’t win that trust because people realise that next week these people will be protesting about chemtrails or vaccinations. They don’t have the credibility that the health and scientific experts have and that is what counts in referenda – not details of a complex science.
LikeLike
. . . especially since Cedric keeps posting videos . . . not his own I presume . . . or are they allowed because he agrees with you?
LikeLike
So true about the details of a complex science . . . I note that the DHB’s never let the facts get in the way of a good campaign . . . but ‘health and scientific experts’ are no longer fooling all of the people all of the time . . . now that they only fool a shrinking % all of the time and a growing % none of the time . . . see where that graph’s going? . . . :}
LikeLike
You are diverting away from the questions put to you Tricia – quickly losing any credibility you might have had.
Come on, I am trying to get a better standard of discussion on these debate articles.
LikeLike
Forgive the off-topic diversion but this lecture on Smallpox and Jenner is excellent. Gives a very balanced look at the man himself as well, warts and all. approx 60min
From Jenner to Wakefield: The long shadow of the anti-vaccination movement
LikeLike
The horse story and video has appeared prominently on several of the anti-fluoridation sites in NZ. It is rather over the top and I don’t think many people would be convinced by it.
LikeLike
Hi Tricia,
In what way is Ken’s interpretation of the Finnish study faulty?
LikeLike
Trevor, the “rules here” of which you state you were not aware, are standards of accepted science. This is one of the major problems with fluoride opponents. They do not understand accepted scientific standards yet still attempt to interpret and apply science to their position. Unsubstantiated claims and opinions are meaningless in regard to science and healthcare issues, in the absence of valid evidence to support them.
In regard to the Iowa Study, this was a study to determine if the current optimal level of fluoride, i.e. that concentration at which maximum dental decay prevention occurs with no adverse effects, could be further refined to a level which provided even more decay prevention, with less dental fluorosis. The range of study was 0.5 ppm to 0.8 ppm, the current optimal level being 0.7 ppm. The conclusion was that the optimal level could not be narrowed down any further due to the existence of far too many variables. There was found to be too much intermingling between fluoridated and non-fluoridated areas for there to be any definitive segregation between the two groups for the purpose of study. The dental fluorosis they found was overwhelmingly of the barely detectable nature, and posed no effect on cosmetics, form, or function of teeth.
Given the inability to accurately determine the degree of exposure to the current optimal level of fluoride for the subjects of the study, there could be no reliable results obtained on decay rates of fluoridated versus non-fluoridated subjects. This is the fallacy of fluoride opponents taking quotes from this study and others, and posting them out of context on their websites. These studies must be read and considered in their complete and proper contexts before attempting to draw any conclusions from them.
Steven D. Slott, DDS
LikeLike
So let’s recap…
Appeals to faulty Authority.
Anecdotes.
More Anecdotes.
Conspiracy theories.
Not being able to stop at just one position on science denialism.
Cutting and pasting.
More cutting and pasting.
Serious confusion about this whole fussy citiations business.
And handwaving about videos that support critical thinking skills.
Hmm.
I’m shocked (SHOCKED!!) to find out that there is gambling going on in this establishment.
All we need now is a rant typed out in allcaps.
LikeLike
Steve you did not cite any valid evidence for the claims you made about Cathy Justus’ horses, you brought this up not me. Your argument is meaningless. You did not state where you read this story. You didn’t even know where they lived. I think you are the biased. I already told you that she had to take the horses to the different vets because they didn’t know what was wrong with them not as you say that they told her fluoride poisoning was not the cause of death. If fluoride didn’t harm her horses and kill some of them then what did? Can you provide your citations and proof of what you are saying? As I mentioned there are 2 peer reviewed studies from Dr. Krook on her horses which is well documented.
LikeLike
1st peer reviewed scientific manuscript on horses by Dr. Lennart P. Krook and Cathy Justus “FLUORIDE POISONING OF HORSES FROM ARTIFICIALLY FLUORIDATED DRINKING WATER” http://www.fluorideresearch.org/391/files/3913-10.pdf
2nd peer reviewed scientific manuscript on horses by Cathy Justus and Lennart P. Krook “ALLERGY IN HORSES FROM ARTIFICIALLY FLUORIDATED WATER” http://www.fluorideresearch.org/392/files/39289-94.pdf
3rd peer reviewed scientific manuscript on horses by Pixi Macicek and Dr. Lennart Krook “FLUOROSIS IN HORSES DRINKING ARTIFICIALLY FLUORIDATED WATER” http://www.fluorideresearch.org/413/files/FJ2008_v41_n3_p177-183.pdf
Editorial on equines by Dr. Bruce Spittle: “FLUORIDE TOXICITY AND DONKEYS” http://www.fluorideresearch.org/431a/files/FJ2010_v43_n1_p004.pdf
4th peer reviewed scientific manuscript on equines by S.L Choubisa, Vdaipur, India “OSTEO-DENTAL FLUOROSIS IN DOMESTIC HORSES AND DONKEYS IN RAJASTHAN, INDIA” http://www.fluorideresearch.org/431a/files/FJ2010_v43_n1_p005-012.pdf
LikeLike
I read through those studies, Steve, and I continue to be surprised at the poor quality. Yes, with hundreds of studies being conducted over half a century, there should be much better literature reviews and studies available. Are these the most compelling? In Australia SES was controlled for based on general area of the postal address or the postal address of the dental clinic visited, which is a loose way of defining that variable. In the Brazil study, even the authors noted significant issues with the data, and, importantly, the single largest factor is was time. A 25% reduction in decay was seen country-wide every 5 years. I have worked in Brazil with low income populations and collaborate with a number of colleagues there frequently, and it is clear that socio-economic status plays an even more important role there than in the United States. The authors of this study did not control for socio-economic status (or rather, the Human Development Index data they tried to use had to be thrown out of the model because it wasn’t proving significant in regression analysis). This isn’t surprising considering that it would have been very hard to gather all this data. Have you read through the whole study from Brazil, or just the abstract?
Is there a government review or a guide for policy makers you’re aware of that discusses the full weight of the evidence with references to the literature?
LikeLike
In the Iowa study it looked at all sources of fluoride intake from water, dentrifice, supplements, as well as other foods and beverages made with, or containing water. In the study it states that fluoride’s benefits are mostly topical. The concept of an “optimal” or target intake is relatively moot. Children who were free of both caries and fluorosis had mean fluoride intakes of less than 0.05mg F/Kg bw. The group with fluorosis but free of caries had mean intakes mostly higher than the other groups. These findings suggest that achieving a caries-free status may have relatively little to do with fluoride intake, while fluorosis is clearly more dependent on fluoride intake. Also it says the range of 0.05 to 0.07 mg F/kg bw may still be associated with caries prevention, it may not be optimal in preventing fluorosis. Limiting fluoride intake to less than 0.05mg F/kg bw may be appropriate to prevent fluorosis. As stated by Burt and Eklund perhaps it is time that “the term optimal fluoride intake be dropped from common usage”.
AS you state the Iowa study does have it’s challenges to determine the exact amounts of fluoride ingested each day by each child but this is the same challenge of other tooth decay surveys that are done. This is why I think that Weston Price’s studies are alot better as he looked at diets of people with and without cavities and these people did not have any cavities whatsoever who eat unprocessed natural foods. Those that ate processed food developed cavities, cavities have nothing to do with fluoride intake as the Iowa fluoride findings suggest that achieving a caries-free status may have relatively little to do with fluoride intake, you can have perfect teeth without fluoride. Cavities are not caused by lack of fluoride.
LikeLike
I came across the issue of fluoridation trying to answer the question “how much fluoride should my one year old and 3 year old have, and quickly found that there is widespread disagreement. Here is a 2009 study that deals with the problematic nature of ingested fluoride and recommended intake, using the Iowa Fluoride Study data.
http://onlinelibrary.wiley.com/doi/10.1111/j.1752-7325.2008.00108.x/full
Considerations on Optimal Fluoride Intake Using Dental Fluorosis and Dental Caries Outcomes – A Longitudinal Study
John J. Warren DDS, MS1,*, Steven M. Levy DDS, MPH2, Barbara Broffitt MS1, Joseph E. Cavanaugh PhD3, Michael J. Kanellis DDS, MS4, Karin Weber-Gasparoni DDS, MS, PhD4
ABSTRACT:
Objectives: The “optimal” intake of fluoride has been widely accepted for decades as between 0.05 and 0.07 mg fluoride per kilogram of body weight (mg F/kg bw) but is based on limited scientific evidence. The purpose of this paper is to present longitudinal fluoride intake data for children free of dental fluorosis in the early-erupting permanent dentition and free of dental caries in both the primary and early-erupting permanent teeth as an estimate of optimal fluoride intake. Methods: Data on fluoride ingestion were obtained from parents of 602 Iowa Fluoride Study children through periodic questionnaires at the ages of 6 weeks; 3, 6, 9, 12, 16, 20, 24, 28, 32, and 36 months; and then at 6-month intervals thereafter. Estimates of total fluoride intake at each time point were made by summing amounts from water, dentifrice, and supplements, as well as other foods and beverages made with, or containing, water. Caries data were obtained from examinations of children at ages 5 and 9 years, whereas fluorosis data were obtained from examinations of children only at age 9 years. Results: The estimated mean daily fluoride intake for those children with no caries history and no fluorosis at age 9 years was at, or below, 0.05 mg F/kg bw for nearly all time points through the first 48 months of life, and this level declined thereafter. Children with caries had generally slightly less intakes, whereas those with fluorosis generally had slightly higher intakes. Conclusions: Given the overlap among caries/fluorosis groups in mean fluoride intake and extreme variability in individual fluoride intakes, firmly recommending an “optimal” fluoride intake is problematic.
LikeLike
Alison, see my above comment in regard to the Iowa Study. This study was not to determine a safety level of fluoride, or how much your child “should have”. It was to determine if, within the narrow range of 0.5 ppm to 0.8 ppm, there is a concentration which would provide more dental decay resistance and/or less risk of dental fluorosis. They determined that, due to the overlap of groups, it is not possible to accurately determine a more desirable concentration than the current optimal level of 0.7 ppm. The dental fluorosis about which they speak in the study is verwhelmingly mild to very mild, barely detectable, which has no adverse effect on cosmetics, form, or function of teeth.
Steven D. Slott, DDS
LikeLike
Alison, the studies I cited have all been peer-reviewed. Peer-review evaluates, among other things, validity, adequacy of controls, accurate use of references, methodology, and conclusions. If you want to argue your position based on your opinion that these studies are of inadequate quality, that’s certainly your prerogative. Just understand that your opinion contradicts that of experts in the field who have extensively reviewed these studies.
Steven D. Slott, DDS
LikeLike
Steve, perhaps I chose the wrong words when I said “poor quality”. It’s not that these studies are of poor quality, I just mean that they do not allow us to conclude anything more than what is shown in the data. When taken as a group of five, they do a poor job of providing overwhelming evidence for the universal safety and efficacy of fluoridation. That is all. For example, the Brazil study says that they see it as a good start for outlining future research. The study does that well, and made it through peer review, but it should not be used to make decisions beyond that.
LikeLike
Steve, you have confused the purpose of study. Read it again. They were looking at optimal INTAKE of total fluoride from all sources. It has nothing to do with fluoride concentration in the water, as fluoride can be ingested through a variety of pathways.
LikeLike
Have a look at the USDA fluoride database. White grape juice has a mean concentration of 2.33 ppm fluoride (about 3X the concentration of tap water). Some kids drink a lot of grape juice and in many cases they get a lot more fluoride from the grape juice than water. We cannot simply talk about fluoride in water. There must be a larger context for it that factors in fluoride from ALL sources!
Click to access F02.pdf
LikeLike
…and quickly found that there is widespread disagreement.
Can you name a single scientific community that rejects the consensus on fluoride?
LikeLike
The EPA union of scientists do http://www.nteu280.org/Issues/Fluoride/NTEU280-Fluoride.htm
LikeLike
Hi Alison you can view the list of adequate intake here http://www.nap.edu/openbook.php?record_id=5776&page=303
AI for Infants
0 through 6 months
0.01 mg/day
AI for Children
7 through 12 months
0.5 mg/day
AI for Children
1 through 3 years
0.7 mg/day
AI for Children
4 through 8 years
1 mg/day
AI for Boys
9 through 13 years
2 mg/day
AI for Girls
9 through 13 years
2 mg/day
AI for Boys
14 through 18 years
3 mg/day
AI for Girls
14 through 18 years
3 mg/day
AI for Males
19 years and over
4 mg/day
AI for Females
19 years and over
3 mg/day
LikeLike
Can you name a single scientific community that rejects the consensus on fluoride?
The one mentioned above. Disagreement on how much fluoride is optimal.
LikeLike
Do you have a copy of the full brazilian study Alison? I would like to see it.
LikeLike
Where does the USDA actually say that they reject the scientific consensus on fluoride? That would be pretty big news….if it was true.
LikeLike
Not the USDA. You’re really missing the point. There is disagreement on whether or not there is an optimal level of total ingestion as measured in mg of fluoride per kilogram of body weight per day. See this study: http://onlinelibrary.wiley.com/doi/10.1111/j.1752-7325.2008.00108.x/full
LikeLike
There is disagreement on whether or not there is an optimal level..
I need you to focus.
This is what I asked you…
“Can you name a single scientific community that rejects the consensus on fluoride?”
Well?
LikeLike
Cedric, there also is not a “scientific consensus” on fluoride in the same way that there is about climate change. Experts differ in opinion on the way that fluoride works and how it works most effectively. Water fluoridation is meant to deliver fluoride to populations that might not be getting enough. There is mainstream scientific consensus on the benefit of fluoride for the remineralization of teeth. However, experts differ on a number of the details.
LikeLike
One scientific consensus that was questioned in the article was this: “The “optimal” intake of fluoride has been widely accepted for decades as between 0.05 and 0.07 mg fluoride per kilogram of body weight (mg F/kg bw) but is based on limited scientific evidence….” The study goes on to point out the problems with the widespread “consensus” based on newer data.
Honestly, Cedric. I am not a conspiracy theorist and I, like you, reject poor quality arguments. I also recognize that the majority of anti-fluoride comments posted in forums like this have a strong tendency to be extreme, anecdotal, and illogical. However, pointing out inconsistencies in an argument and asking experts like Steve and Ken to engage in dialogue is no threat to science. I don’t have a hard, extreme position, so I’d rather not get into a back and forth squabble with you.
LikeLike
Cedric, there also is not a “scientific consensus” on fluoride…
Then name a scientific community that rejects the consensus.
There’s loads of scientific communities out there.
Name one.
I don’t have a hard, extreme position…
Never said you did.
So….can you name a single scientific community that rejects the consensus on fluoride?
LikeLike
Further. It is perfectly reasonable that many of us would prefer not to have “very mild” dental fluorosis, as pictured here courtesy of the US CDC.
LikeLike
Alison, the optimal fluoride level in water is set taking into account intake from all sources. The CDC has estimated that 75% of daily fluoride intake from all sources, including dental products, is from the water. Thus, the optimal level of fluoride in water is not only relevant, it is the deciding factor. The Iowa Study concluded that there was too much overlap between groups for it to be possible to segregate fluoridated from non fluoridated sufficiently for the purpose of study.
The Institute of medicine has established that the upper limit of daily fluoride intake from all sources, for all individuals above the age of 8 years, to be 10 mg before adverse effects will occur. For kids below the age of 8, the upper limit is less, for the sole reason that ages 0-8 years are the tooth developing years, and as such during these years, there is a risk of development of mild dental fluorosis if the daily upper limit is exceeded. The upper limit for infants aged 0-6 mos is 0.7 mg/day, that for 6 -12 mos is 0.9 mg per day, for 1-3 years is 1.3 mg, and 4-8 years is 2.2 mg. As there is a risk of exceeding the upper limit for infants if fluoridated water is used to reconstitute powdered formula, for those parents who may be concerned with the development of mild dental fluorosis, the ADA and the CDC have suggested that they either use non-fluoridated bottled water to reconstitute, or simply use premixed formula, most, or all of which are produced with low fluoride content water.
The risk of mild dental fluorosis is the only concern with the establishment of the optimal level of fluoride intake. The Iowa Study attempted to determine if this level could be more precisely determined, if indeed it even heeded to be given the broad range of safety. It determined that it could not.
Click to access ULs%20for%20Vitamins%20and%20Elements.pdf
Steven D. Slott, DDS
LikeLike
Further. It is perfectly reasonable that many of us would prefer…
Is English you second language?
Focus.
Try.
Can you name a single scientific community that rejects the consensus on fluoride?
LikeLike
Don’t know why my img tags don’t seem to be working. Let’s try again.
LikeLike
Wow. This is unpleasant. Cedric, you don’t seem to understand the issue and it is distracting me from having a conversation with Steve. You are interjecting with your own questions that I don’t see as relevant. Maybe if you want to detail what you view as the scientific consensus on fluoride, then I could produce a paper, but for now, I will wait for Ken to moderate. For now, it feels like Cedric is being a bit abusive. Thanks, Steve and Ken for taking the time to respond thoughtfully.
LikeLike
Tricia
The ash from Tongariro has significant levels of fluorine, the soluble form of fluoride. Water from Tongariro has significant fluoride levels because of it.
Much of the “natural” levels of fluoride in Hamilton’s water are derived from Tongariro’s ash via the Waikato River.
How much fluoride is in that Tongariro water you are drinking in the belief that it is free of F?
LikeLike
….here courtesy of the US CDC.
The CDC.
Ah, glad you brought it up. They’re a scientific community.
They accept the scientific consensus on flouoride.
They’re very clear on it.
It’s all there in plain English on their website.
What is fluoride?
Fluoride is a naturally occurring mineral that is proven to protect against tooth decay.
Why is fluoride added to water and toothpaste?
Fluoride’s action in preventing tooth decay benefits both children and adults throughout their lives. The health benefits of fluoridation are—
• Fewer cavities and less severe cavities.
• Less need for fillings and tooth extractions.
• Less pain and suffering associated with tooth decay.
(..)
What is community water fluoridation?
Almost all water contains some naturally occurring fluoride, but usually at levels too low to prevent tooth decay. Many communities choose to adjust the fluoride concentration in the water supply to a level beneficial to reduce tooth decay and promote good oral health. This practice is known as community water fluoridation. Given the dramatic decline in tooth decay during the past 60 years, the Centers for Disease Control and Prevention (CDC) named water fluoridation one of Ten Great Public Health Interventions of the 20th Century.
Can you name a single scientific community that rejects the consensus on fluoride?
Still waiting here.
LikeLike
Alison, it always amazes me that fluoridation opponents speak of total daily fluoride intake as if the CDC, the EPA, the ADA , and all of the other highly respected regulatory bodies and healthcare organizations, have not taken this into account in setting the MCL and optimal levels of fluoride. It’s as if you believe you are privy to some “new” information which all of respected science and healthcare has somehow missed.
Stop relying on half-truths and misinformation found on antifluoridationist websites, and read the literature from reliable, respected, and original sources. You will be amazed to find that these entities are not nearly as incompetent as would antifluoridationists have everyone believe. They actually are way ahead of you.
Steven D. Slott, DDS
LikeLike
I spent 4 1/2 years debating, presenting and educating my town about ‘Hydrofluoslicic acid’
Churchill no fluoride became SafeWater Churchill last November 2012.
Regardless of science, regardless of opinion I did not consent to be medicated! This is a violation of human rights period!
And please, when did a toxic soup waste product become a nutrient?
This is not calcium fluoride which still isn’t a nutrient!
And with less than 1% being consumed how is this cost effective?
Churchill, have now set up a program within the school for parents who wish to receive treatments!
Get your heads out of 50s science that was so obviously doctored!
And lastly to think humans have to drink, bath and cook with a product that is not even NSF 60 approved.
Mark
SafeWater Churchill,Mb Canada
LikeLike
Alison, there are no respected, credible organizations which oppose the public health initiative of water fluoridation.
Steven D. Slott, DDS
LikeLike
This is unpleasant.
I’m asking you to name a single scientific community that rejects the scientific consensus on fluoridation.
Nothing unpleasant about it.
Cedric, you don’t seem to understand the issue…
It’s a question that you don’t seem to be able to answer.
I understand that issue very well.
… and it is distracting me from having a conversation with Steve.
Ah. It’s a “distraction”. How terrible for you.
You are interjecting with your own questions…
No. It’s just one question. Repeated several times.
… that I don’t see as relevant.
Your hand waving is impressive.
Maybe if you want to detail what you view as the scientific consensus on fluoride, then I could produce a paper,…
How extraordinary. I don’t remember asking you to produce a paper.
Focus.
Go on.
Can you name a single scientific community that rejects the consensus on fluoride?
(…awkward silence…)
LikeLike
What is the scientific consensus on Flouride?
Is there one?
LikeLike
They have told me it is between 0.1 and 0.2 ppm and I believe it is not from a source exposed to the ash but would come from calcium fluoride.
I don’t agree with the argument that fluoride from any source is the same.
It is obvious for instance with the salts of arsenic that you can get a lethal dose from one but in another form, with exactly the same amount of arsenic per say, will not kill you.
I am surprised that Ken with his background in soil chemistry isn’t quick to acknowledge this.
I am sure most people will appreciate that there is a difference between sodium chloride and hydrochloric acid;
and yet when it comes to fluoride that goes out the window for some (un?) reason.
The pH matters greatly in the uptake of minerals from the soil and silmilarly in the body the effects on an individual are very individual depending on a great many factors including their genetic makeup, diet, lifestlye etc.
Coupled with Ken’s observation that the body can’t regulate blood and plasma fluoride levels (which again suggesst that we are not designed to be exposed to it ) it truly is a game of Russian roulette that the dental fraternity are asking us all to play . . . I’ve opted out of the game thank you.
LikeLike
Sorry . . . the levels should be 0.01 to 0.02 . . . Oops!
LikeLike
Alison, the degree of desired benefit of any public health initiative can be argued. However, the overwhelming consensus of peer-reviewed science is that water fluoridation significantly prevents dental decay. The problem of rampant, untreated dental disease is overwhelming in nearly all parts of the world. Given that one untreated cavity in one tooth can and does cause an untold amount of pain, debilitation, life-threatening infection, and even death….. given that there have been no proven adverse effects of water fluoridation in the entire 68 year history of the initiative…….and given the fact that fluoridation is nothing more than raising the already existing level of fluoride ions in water by a miniscule few parts per million……there is no scientifically valid reason to oppose this initiative.
The 2006 National Research Council Committee on Fluoride spent 3 years reviewing, in exhaustive detail, all of the relevant, scientific literature on fluoride. Dr. John Doull, the Chair of this 2006 NRC Committee, stated in March of this year:
“I do not believe there is any valid, scientific reason for fearing adverse health conditions from the consumption of water fluoridated at the optimal level”
—John Doull, MD, PhD, Chair of the National Academy of Sciences, National Research Council 2006 Committee Report on Fluoride in Drinking Water
—–http://www.ilikemyteeth.org/wp-content/uploads/2013/03/doull-email-on-cwf-march-2013.pdf
Steven D. Slott, DDS
LikeLike
Hi Tricia,
You claimed Ken was wrong about the Finnish study.
In what way is Ken’s interpretation of the Finnish study faulty?
(Polite, repeated question).
LikeLike
It’s hard to find adverse effects if you firmly believe there are none and don’t look for any, Steve.
A few miniscule parts per million are all it takes of some substances to alter the nesting habits of some birds,to change the gender in others, and innumerable other effects on the hormonal system see ‘Our stolen Future’ . . . I would put fluoride in that category.
Ken starts with comparisons of Selenium and how it can be toxic over a certain level and assumes that Fluoride is in the same category.
No study has been able to show that F is an essential nutrient and therefore is more aptly put with Cadmium, Arsenic, Mercury and Lead . . . none of them desirable to ingest in any quantity, certainly not on purpose;
and especially since the synergistic effects of one with the other have not been elucidated;
and it has been shown that F increases the uptake of lead . . . even more so in Latino than European, and even more so in Afro-American than either of the other two groups.
The last doctor I had a conversation with was very blase, spouting forth the benefits of fluoride to dental health and convinced that it was totally harmless . . . but then he didn’t even know what was being put into the water.
Such is the blind acceptance of dogma in dental and medical circles.
LikeLike
Tricia, you again exemplify one of the major problem with fluoride opponents. You simply do not not understand the science and discount the opinions of those who do. An elementary chemistry text will tell you that a fluoride ion is a fluoride ion, regardless the source. Whether that ion is released from the compound Calcium Fluoride, the compound Sodium Fluoride, or the compound Hydrofluorosilic Acid, it is identical. This fluoride ion and nearly undetectable amounts of trace contaminants are the only substances ingested as a result of fluoridation. The trace contaminants are in such miniscule amounts that they are harmless, and the fluoride ion is identical to that released by CaF, or any other source.
You certainly may substitute your opinion for that of proven scientific fact, if that is what you wish to believe. However, your credibility in so doing is at zero.
Steven D. Slott, DDS
LikeLike
Tricia, again, there must be valid evidence that there is a problem before it is reasonable to demand proof that there is not. Demanding proof of a negative is not valid science, it is simply a fishing expedition for the purpose of endless stalling. There will always be unsubstantiated claims made by fluoridation opponents regardless of how many times they are refuted.
Provide valid support for your claims, or they are meaningless.
Steven D. Slott, DDS
LikeLike
>i>Demanding proof of a negative is not valid science,
It is if you are Tricia and apply the brand new branch of statistics that she has invented and also used in her opening comment.
LikeLike
Alison, I am neither an expert, nor any sort of authority on water fluoridation. I’m simply a healthcare professional who has done due diligence in researching this issue from reliable, respected, and original sources.
Steven D. Slott, DDS
LikeLike
Mark, fluoridated water does indeed meet EPA mandated NSF Standard 60 certification requirements. If it did not, it would not be allowed. Standard 60 begins with water at the tap. Hydrofluorosilic Acid does not exist at the tap, it is not ingested, and is therefore of no concern whatsoever. For accurate information on NSF certification in regard to the contents of fluoridated water:
http://www.nsf.org/newsroom/nsf-fact-sheet-on-fluoridation-chemicals
Steven D. Slott, DDS
LikeLike
My main contention is with the assertion that 75% of fluoride intake comes from water. This is simply not supported by the literature. For any child that drinks grape juice on a daily basis, this is not true. In fact, most kids that are at an elevated risk of decay are not drinking much water anyway! I’m not sure about NZ. The levels of fluoride in white grape juices may not be as high… They may not allow such a heavy use of cryolite, which is a fluoride based pesticide.
I’m also wondering if studies from the US have looked at the IQ correlation… I know the Chinese don’t prove that there is an issue, but it is probably worth researching. It is widely accepted that bottle-fed babies tend to have slightly lower IQ’s than breasted children, and no one knows exactly why.
LikeLike
Trevor, fluoride is not a drug, and it is not “forced” upon anyone. Fluoride is a mineral which the FDA must classify as a drug for the sole reason of its stated use in water as a therapeutic rather than as a disinfectant. No other reason. As the EPA regulates all mineral additives to water, it is the EPA, not the FDA, which controls and regulates fluoride in water. Fluoridated water meets all NSF Standard 60 certification requirements as mandated by the EPA. There are no dosage requirements for fluoride, nor is there any need for such, any more than is there any need of dosage requirements of chlorine in water.
Steven D. Slott, DDS
LikeLike
Trevor, take my comments on the horse tale any way you wish. I simply used it as an example of confirmation bias.
Steven D. Slott, DDS
LikeLike
Trevor, the fluoride ion released by Calcium Fluoride into water is identical to the fluoride ion released into water by HFA. This is simply elementary chemistry. Continue to deny this if you wish, but facts are facts.
Steven D. Slott, DDS
LikeLike
Alison
Grape juice in New Zealand is almost the price of wine.
Children may drink it a few times a year, if at all.
They will certainly drink water much more often.
LikeLike
Proponents claim that once the silicon fluorides have been diluted at the public water works they are completely dissociated to free fluoride ions and hydrated silica and thus there is no need to examine the toxicology of these compounds. However, while a study from the University of Michigan (Finney et al., 2006) showed complete dissociation at neutral pH, in acidic conditions (pH 3) there was a stable complex containing five fluoride ions. Thus the possibility arises that such a complex may be regenerated in the stomach where the pH lies between 1 and 2. There should be more testing on these silicon fluorides to make sure they are safe.
LikeLike
Tricia.
Most of the central North Island is covered with ash from Tongariro. Almost all of the rest of New Zealand, including the Chatham Islands, is covered with ash from the Taupo volcano.
If you take water from anywhere in the Tongariro district, it has definitely been exposed to fluorine in the ash from Tongariro. If I were you, I would question those figures that you have been given for fluoride concentrations in water from Tongariro.
“I don’t agree with the argument that fluoride from any source is the same.”
It’s not an argument. It’s as close to fact as science can get.
Basic chemistry: a fluorine atom is a fluorine atom is a fluorine atom.
A fluorine atom is not (for example) a chlorine atom, an iron atom, or a mercury atom. It is a fluorine atom. That’s why it is called a fluorine atom. If it were something else it would not be fluorine. Fluoride is merely the name given to a fluorine atom found within a chemical compound; it is still a fluorine atom.
A sodium atom in sodium chloride is indistinguishable from a sodium atom in sodium fluoride. A chlorine atom in sodium chloride is indistinguishable from a chlorine atom in hydrogen chloride. A hydrogen atom in hydrogen chloride is indistinguishable from a hydrogen atom in water. A fluorine atom in sodium fluoride is indistinguishable from a fluorine atom in polytetrafluoroethylene (Teflon).
The same can be said for every element in the periodic table. There are no exceptions, not even fluorine.
(For pedants, I’m talking chemistry, not the physics of isotopes)
LikeLike
Trevor, you are straw clutching to think that F reacts with SiO2 in the stomach to produce fluorosilic acid again. Because the molecule dissociates to H+ (or really H2O), F-, and hydrated silica, and the silica then polymerises by olimerisation, the reaction is actually a deocmposition reaction. It doesn’t reverse itself because SiO2 is removed – especially with the time taken from the original dilution to arriving at your tap.
If I were you I would avoid this argument (even though Connett apears to advocate it) – it is bad chemistry.
Because of the extremely low pH F exists mainly as the HF moelcule in the stomach, and this enhances its ability to tranfer though membranes to the blood stream where it will exist as the F- anion again.
LikeLike
Again, Trevor, you are not providing references, citations or links. I will hold such comments in moderation.
LikeLike
Looks like the discussion here is drying up and going around in circles with simple reasserting what has been said before.
Tomorrow I will post Paul Connett’s response to this article.
Hopefully discussion can then transfer to the comments in that post and be relevant to his response.
LikeLike
Trevor, fluoride at 0.7 ppm does require any “approval”. As a mineral additive to water it is under the regulatory authority of the EPA, not the FDA.
The FDA is just one of several regulatory agencies that ensure public safety. The FDA’s authority is limited to products sold to the public and fluoride has been approved for use in toothpastes, mouth rinses and even bottled water. The FDA has no role in approving drinking water additives pursuant to their agreement with the EPA in the early 1980’s. Additives are covered by state regulation’s. It should be noted that the FDA does not have the authority to approve many of the products we use every day.
The Safe Drinking Water Act (SDWA) of 1974 confers the authority for ensuring the safety of public drinking water to the Environmental Protection Agency (EPA). The EPA is responsible for setting drinking water standards and has the authority to regulate the addition of fluoride to the public drinking water.
—–http://www.cdph.ca.gov/programs/Pages/FluorideandApproval.aspx
——http://www.epa.gov/safewater/standard/setting.html
Steven D. Slott, DDS
LikeLike
Trevor, in regard to the “convincing Canadian studies” to which you linked, not directly, but through an antifluoridationist website: two are actual studies, one is simply a report, and two are Masters’ Theses of public Health graduate students.
Let’s take a look at these studies when viewed in their original context, not filtered and edited through antifluoridationists websites:
1) Study
“In the larger scheme of things, it appears that the role of water fluoridation in supporting good oral health must be weighed against other measures that may achieve similar success but at a higher cost, such as the widespread utilization of sealants. Moreover, it is unwise to resort to restorative interventions to meet the challenge of dental decay when a primary prevention measure such as water fluoridation preserves the integrity of dental tissues overall, is less expensive, and is more effective.”
—–Patterns of dental caries following the cessation of water fluoridation
Maupome ́ G, Clark DC, Levy SM, Berkowitz J. Patterns of dental caries following the cessation of water fluoridation. Community Dent Oral Epidemiol 2001; 29: 37– 47. C Munksgaard, 2001
2) Study
“Results also suggest that the overall aesthetic ratings of parents concerning the colour of their children’s teeth did not change despite significant changes in the prevalence and severity of fluorosis scores. Most parents across all cycles rated the colour of their children’s teeth to be aesthetically acceptable or better. These results support the conclusion that fluorosis-related aesthetic problems are rare.”
“Following fluoridation cessation of the public water supply, the prevalence and severity of dental fluorosis decreased significantly. However, during this same time period the reported use of fluoride supplements and fluoride dentifrice decreased as well. Our analyses were unable to determine the influences of these different fluoride exposures and decreases and therefore suggest that different fluoride sources have played a role in declining TFI scores; their exact contribution to the relative effect is unclear. Furthermore, the decreases in TFI scores did not seem to affect the aesthetic ratings of parents during the study period.”
———-Changes in dental fluorosis following the cessation of water fluoridation
Clark DC, Shulman JD, Maupome ́ G, Levy SM. Changes in dental fluorosis following the cessation of water fluoridation. Community Dent Oral Epidemiol 2006; 34: 197–204. Ó Blackwell Munksgaard, 2006
3) Report
“Although current studies of the effectiveness of water fluoridation have design weaknesses and methodological flaws, the balance of evidence suggests that rates of dental decay are lower in fluoridated than non-fluoridated communities. The magnitude of the effect is not large in absolute terms, is often not statistically significant and may not be of clinical significance. The effect tends to be more pronounced in the deciduous dentition. The effect tends to be maximized among children from the lower socioeconomic groups so that this section of the population may be the prime beneficiary.”
“Fluoride is a poison in large doses but toxic levels cannot be achieved by drinking fluoridated water. Fluoride products such as toothpaste should be kept out of the reach of children since toxic amounts could be ingested via these sources.”
“Current studies support the view that dental fluorosis has increased in both fluoridated and non-fluoridated communities. North American studies suggest rates of 20 to 75% in the former and 12 to 45% in the latter. Although largely confined to the ‘very mild’ and ‘mild’ categories of the condition, they are of concern insofar as they are discernable to the lay population and may impact on those so affected.”
“Studies of bone mineral density have not detected changes consistent with the clinical picture of skeletal fluorosis from water containing levels of fluoride optimal for the reduction of dental decay.”
“Studies of the association between water fluoridation and bone fracture are largely ecological in design. Of 11 studies published prior to 1994, two showed a protective effect, five showed no association and four suggested an increase in hip fracture rates. In the latter, the strength of the association was weak, with relative risks ranging from 1.1 to 1.4.”
“The few studies published during the review period do not challenge earlier research showing that there is no reason to believe that exposure to fluoridated water increases the risk of cancer in bones or other body tissues”
“Recent studies emanating from China have claimed that children exposed to high levels of fluoride have lower IQ’s than children exposed to low levels. The two studies claiming such an effect are deeply flawed and provide no credible evidence that fluoride obtained from water or industrial pollution affects the intellectual development of children.”
——–BENEFITS AND RISKS OF WATER FLUORIDATION An Update of the 1996 Federal-Provincial Sub-committee Report
Prepared under contract for: Public Health Branch, Ontario Ministry of Health First Nations and Inuit Health Branch, Health Canada
4) Masters Thesis
We found n difference in caries prevalence or severity between 7 year old children from schools in non-fluoridated Caledon and schools matched on socio-economic factors, in fluoridated Brampton.”
“Residence in the two affluent communities did not accurately represent actual exposure to fluoridated drinking water due to the use of reverse osmosis filters, bottled water, and the mobility of families.”
“As shown by the numerous reviews, fluoridation remains an effective public health preventive intervention. It’s effectiveness is due to its basic efficacy, its population-wide coverage through reticulated water systems, and its effortless compliance by susceptible people of all ages.”
——-ITO, Caledon and Brampton Study, Peel Region (2757 Determinants of Caries in Adjacent Fluoridated and Non-fluoridated Cities) Mar 21, 2007
5) Masters Thesis
“Nevertheless, our findings which show little difference when fluoridation is stopped come from more stable, single cultural communities. Thus, in Toronto, 1) in the absence of universal access to preventive and restorative dental care; 2) high rates of immigration; and 3) high status of child poverty; the answer to the question of what would happen if water fluoridation were stopped is uncertain”
——-Azarpazhooh, Oral Health Consequences of the Cessation of Water Fluoridation in Toronto, MSc Thesis Report, Faculty of Dentistry – University of Toronto, City of Toronto Public Health, August 2006
Steven D. Slott, DDS
LikeLike
Trevor, FAN is a highly biased antifluoridationist group run by antifluoridationist/activist, Paul Connett. Neither it, nor its website “fluoridealert.org” can be considered as valid sites for accurate information on fluoridation. If you want credibility for your claims, it would be best to cite legitimate sources, not antifluoridationist websites.
Steven D. Slott, DDS
LikeLike
Trevor, every one of your “peer-reviewed articles on the horse tale are from “fluorideresearch.org”, an antifluoridationist website. Again, antifluoridationist websites are not valid sources of information. If you want credibility for your claims, it would be best to cite original sources, and refrain from citing filtered and edited information found on these highly biased, unreliable websites.
Steven D. Slott, DDS
LikeLike
Trevor, you are correct, cavities are not caused by a lack of fluoride. Fluoride does, however, provide protection against the cavities that are formed for a variety of reasons. Prevention is the key to effective addressing of any disease, including dental. Water fluoridation is a proven beneficial public health initiative that does just that, with no proven adverse effects in its 68 year history.
Steven D. Slott, DDS
LikeLike
I endorse the criticism of sites like Fluoride Alert and (in NZ) FANNZ – especially when it come to talking about research studies. I have found these cites very bad with citations. Often the links do not work. But also they have a habit of misrepresenting the cited paper – often claiming they say the exact opposite of what they do.
My attitude is always to check the original study – never trust sites like Fluoride Alert. I am always suspicious of people relying on Fluoride Alert as a reference. And I do know of at least one Facebook page which sends any comments including the words straight to spam.
Hey that is an idea – perhaps if I automatically send comments using Fluoride Alert straight to spam it will encourage commenters to look at the original work. 🙂
>
LikeLike
Trevor, in regard to the EPA Union, the National Federation of Federal Employees first referred to was a very small union of less than 1000 in an agency with 20,000 employees. A group of fewer than 20 passed the “resolution” supporting California antifluoridation efforts shortly before the union went out of business. There is no record of any official position on fluoridation of the National Treasury Employees Union, the Union that absorbed the NFFE membership when it went out of business, and the EPA does not support the statements of this union.
The driving force behind the union antifluoridationist activities was William Hirzy, then Vice-President of the union, and now the current paid lobbyist for Paul Connett’s antifluoridationist group, FAN. It is also useful to note that a recent petition by Hirzy to the EPA to ban use of HFA as a fluoridating agent, was totally refuted and rejected by the EPA. The reason for this rejection was due to Hirzy’s reliance on data from a study which he and fellow antifluoridationist, Robert Carton recently published in which they claimed increased rates of cancer from use of HFA. When the EPA reviewers examined the data from this study, they found an elemental error in math made by Hirzy, which produced a 70-fold error in the calculations of Hirzy and Carton. When this error was corrected by the EPA reviewers, they determined that Hirzy and Carton’s study proved exactly the opposite of what Hirzy and Carton had concluded. When notified of this grievous error and rejection of his petition, Hirzy stated that he was “embarrassed”, as he well should have been.
Steven D. Slott, DDS
LikeLike
Trevor, you cite “adequate intake” , not “upper limits”. The upper limit of daily fluoride ingstion is that maximum level which may be ingested without adverse effcts, long or short term. As I stated rarlier, the UL for all individuals over the age of 8 years, is 10 mg per day. Before this level could be reached, water toxicity would be the problem, not fluoride.
For infants and children in their tooth developing years of 0-8, the UL is lower, but only due to a risk of development of mild dental fluorosis, an effect which has no adverse effect on cosmetics, form, function, or health of teeth.
Steven D. Slott, DDS
LikeLike
Trevor, the peer-reviewed science is clear on the matter of immediate and complete hydrolyzation (dissociation) of HFA at the pH of water. Finney, et al put that issue to rest. Yes, at low pH, HF may reform. However, that it CAN reform, does not mean that it DOES, especially at the minute concentration ingested from fluoridated water. The theory that it does at this concentration is mere conjecture, with no valid, supporting evidence. As humans have been ingesting the fluoride ion in water since the beginning of time, were the reformation of HF to have been a problem, there would have been massive GI ulcerations and erosions of the epithelial lining, with all associated problems. This, obviously, has not been the case.
So, once again, demanding proof that there is not a problem requires there to be valid evidence that there is a problem in the first place. There is no valid evidence, whatsoever, of HF reformation in the gut.
Steven D. Slott, DDS
LikeLike
Trevor, again, there is no valid proof of adverse effects of fluoride at the concentration of 0.7 ppm. If you want to look at “dose” then realize that water is fluoridated at 0.7 mg/liter (ppm=mg/liter). Thus, for every liter of fluoridated water consumed, 0.7 mg of fluoride is ingested. The average daily water consumption of adults us 2-3 liters but, for the purpose of example, let’s use an excessive consumption of 6 liters of water per day. This would mean 4.2 mg of fluoride ingested. As the CDC has estimated 75% of fluoride intake from all sources to be from the water, this would mean the 75% of daily fluoride intake for an excessive consumption of 6 liters of water per day would be 4.2 mg. Thus, the daily fluoride intake from all sources for this excessive water drinker would be 5.6 mg., only slightly more than half the daily upper limit of 10 mg. As I stated in a previous comment, before even approaching the UL of 10 mg per day, water toxicity would be the problem, not fluoride.
Steven D. Slott, DDS
LikeLike
Hi All –
Loving the discussion/debate so far. Any theories on why the people who are opposed to fluoridation go to such lengths and effort to search for studies and then mis-report or misconstrue them and in some cases actually alter them – it must take a huge amount of time/resources.
Especially when it’s so easy to verify/check now….would love to hear what Trevor says about your reply to his sources, Steven
LikeLike
Alison, again, if you want to substitute your own opinion on how much fluoride is ingested on a daily basis, certainly that is your prerogative. Making your argument based on your own opinion versus that of the CDC, will be a difficult task, however.
“In the United States, water and processed beverages (e.g., soft drinks and fruit juices) can provide approximately 75% of a person’s fluoride intake. Many processed beverages are prepared in locations where the drinking water is fluoridated. Foods and ingredients used in food processing vary in their fluoride content. As consumption of processed beverages by children increases, fluoride intake in communities without fluoridated water will increase whenever the water source for the processed beverage is fluoridated (84). In fluoridated areas, dietary fluoride intake has been stable because processed beverages have been substituted for tap water and for beverages prepared in the home using tap water.”
—http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5014a1.htm
Steven D. Slott, DDS
LikeLike
I think confirmation bias is a human failing, Scrag – we all suffer from it and the ideologically driven more so. Remember the gorilla video?
LikeLike
Trevor, I won’t approve your last comment without the citation details. Simple names are just not good enough.
LikeLike
So are the dissociation constants for calcium fluoride and hydrofluosilicic acid the same?
LikeLike
Well said Trevor . . . cavities are not caused by lack of fluoride . . . end of story . . . :}
LikeLike
HI Tricia, good to see you are reading the comments.
You asserted than Ken had misinterpreted the Finnish study illustrating the placebo effect on fluoridation complaints.
Might you please explain to readers how he got it wrong?
LikeLike
I would still rather sprinkle sodium chloride on my food rather than hydrochloric acid and take calcium chloride in my tea rather than hydrofluorosilicic acid . . . is that OK with you?
Furthermore the substances added to water behave differently depending on what form they are added . . . they dissociate differently also depending on the make up of other substances in solution e.g. pH . . . as Ken has already alluded to on the take up of minerals from the soil.
And the interactions and synergistic effects haven’t even begun to be studied in any realistic way i.e. as it may be happening inside the body with the complexities of human physiology.
LikeLike
Exactly Trevor . . . in fact the effects already observed on gastric function already confirms that they are not safe.
LikeLike
5) What happens when water fluoridation is stopped has been established . . . teeth keep improving!
LikeLike
I would still rather sprinkle sodium chloride on my food rather than hydrochloric acid and take calcium chloride in my tea rather than hydrofluorosilicic acid
And who wouldn’t?
LikeLike
Since most of the other sources are pro-fluoridationist I would be wary of them also . . . :}
LikeLike
What you and your fellow contributors have established beyond a shadow of a doubt that this is just another highly biased website, steeped in pro-fluoridation ideology making it extremely unreliable.
LikeLike
See what I mean . . . just trotting out the dogma.
LikeLike
OK Tricia, your refusal to answer the repeated question must mean that …
…you don’t know the answer…
(no gasp inserted here)
…and you were just making stuff up.
(nor here)
LikeLike
Tricia “dissociation constants” is really not an appropriate term. CaF2 is an ionic solid and has a defined solubility constant. It is relatively insoluble which explains it’s lower toxicity than, say NaF which is far more soluble.
Fluorisilicic acid has a fluorosilicate anion which is covalent. While we can define dissociation constants for each stage of removal of fluoride, in practice because of the olimerisation and precipitation of SiO2, and it’s removal from equilibrium, the reaction is a decomposition rather than dissociation. When diluted at neutral pH values the final form of F is the hydrated F anion, the same as resulting from dissolution of caF2 or NaF.
There is absolutely no difference between the hydrated F anions from the different sources. Anyone who tells you that is being silly and just doesn’t understand basic chemistry.
LikeLike
Trica, why would you put HCl on your food? Acetic acid perhaps, but HCl? How silly.
Why would you put either CaCl2 or fluorosilicic acid in your tea? Again, how silly.
The hydrated F anion behaves as the hydrated F anion in dilute water – it’s reactions have nothing to do with the original chemical added at all. Whatever gave you the idea it would differ – that is completely silly.
Yes, the other ions on solution will participate possibly in reactions if present at high enough concentrations. That depends on what other chemicals are present, not on original fluoridating agent. Addition of lime, for example, could lead to precipitation of CaF2.
pH is a given because of the requirement to neutralise water so that corrosion of pipes is prevented. Certainly finished water is never at the low pH values which would interfere with decomposition of the fluorosilicate anion.
It is rubbish to claim that these reactions “haven’t even begun to be studied” – absolute rubbish. Why do anti-fluoridationists continually tell such lies?
Sure reactions in the body are complex – but we do know quite a bit and their complexity certainly does not excuse people who make up their own stories about it.
As they say, you are entitled to your own opinion, but not your own facts.
Now, please explain where I was wrong about the Finnish study.
LikeLike
That Number 5) makes you comment look like a thoughtless copy and paste, Tricia.
What happens when fluoridation stops – well there are studies as well as anecdotal evidence. But what about you providing evidence for your claim? And be careful, what happens will depend on what replaces fluoridation.
The Cuban study that the anti-fluoridationists continually quote is an example. The anti-fluoridationists never tell you this but when the fluoridation of the public water supply stopped it was replaced by a regular fluoride mouthwash programme in the schools. Unsurprisingly tooth decay in the children did not increase.
LikeLike
Of course you would endorse the criticism of sites like Fluoride Alert and FANNZ . . . because they disagree with you . . . and you would allow the most rude and outrageous comments about them but not about any of your sources because they all agree with you . . . . wow that’s really unbiased Ken.
LikeLike
Dental fluorosis is the first obvious sign of fluoride toxicity and if you had it may be you wouldn’t be so blase about it.
LikeLike
But there is evidence of gastric distress.
LikeLike
That’s nonsense – there is a lot of documented cases of adverse effects of fluoride at .7ppm or thereabouts.
LikeLike
Remind me not to buy anything from fluoridated regions . . . I’ve already told Hamilton that so I must tell all the other regions in NZ as well . . . thank you for the reminder . . . :}
LikeLike
If that were true maybe they caught it off the original Napier/Hastings experimenters?
LikeLike
Tricia, I think I have explained how my own experience using references to FA and FANNZ sources has shown the sources to be very unreliable – to the extent that they will often claim a paper says the exact opposite of what it really does. If you are not prepared to check out the originals please don’t be surprised if a scientifically aware person does not accept your claims.
Honest scientists do go to primary sources. I don’t accept anything from people who refuse to.
LikeLike
You’ve certainly been exhibiting it here Ken by allowing disgusting comments from your fellow idelogically driven pro-fluoridationists while binning even a hint from those who disagree with you.
LikeLike
Well said once againTrevor.
LikeLike
Unless they’re simple names you agree with Ken.
LikeLike
Trica, this is getting childish. I suggest you take a break. Perhaps have a look tomorrow at Paul’s new article – you might feel happier with that.
Nothing new is coming up here.
LikeLike
Trish, a word in your ear: Entering a simple punctuation mark between sentences works better than using the *post comment* button.
LikeLike
Hey,
Perhaps I don’t know how things work on this page…I seem to see comments from Tricia replying to those of Trevor yet can’t see any posts from Trevor in ages…?
Would like to see Tricias reply why Ken was wrong re: to the Finnish study?
LikeLike
Only the labels change. It’s uncanny.
“Since most of the other sources are pro-moon landings I would be wary of them also . . . :}
What you and your fellow contributors have established beyond a shadow of a doubt that this is just another highly biased website, steeped in pro-moon landing ideology making it extremely unreliable.
See what I mean . . . just trotting out the dogma.”
“Of course you would endorse the criticism of sites like AnswersinGenesis and ICR . . . because they disagree with you . . . and you would allow the most rude and outrageous comments about them but not about any of your sources because they all agree with you . . . . wow that’s really unbiased Ken.”
“You’ve certainly been exhibiting it here Ken by allowing disgusting comments from your fellow idelogically driven pro-warmists while binning even a hint from those who disagree with you.”
No need to change a thing.
LikeLike
Oh, another thing Trish, you made assertions regarding fluoridation and inhibition of enzyme action https://openparachute.wordpress.com/2013/10/30/fluoride-debate-part-1-perrott/#comment-46327
Both Chris and Ken requested clarification as to concentration of fluoride required for this inhibition. e.g. https://openparachute.wordpress.com/2013/10/30/fluoride-debate-part-1-perrott/#comment-46329
Still waiting.
Surely you can stand behind your claims.
LikeLike
It’s very rude and outrageous of you to ask Tricia to stand behind her claims, Richard.
Disgusting comment, really.
It’s (what’s the word?) unpleasant.
Yes, that’s what it is. Unpleasant.
Can’t you see that she doesn’t have a hard, extreme position?
You don’t seem to understand the real issue.
And interjecting. Oh mercy! The interjecting.
It is distracting Tricia from having a conversation with Ken.
Shame on you, Richard.
Besides, I’m sure Tricia doesn’t see it as relevent.
So there!
LikeLike
I don’t know how the denier mind works.
I read their claims repeatedly shot down in total flames – often they exposed as blatant lies – yet instead of honestly asking themselves if their position is still tenable they go extraordinary effort to invent some other new line of attack. Trevor’s implausible scenario of compounds regenerating in the stomach is a perfect example.
LikeLike
ChristopherAtkinson | November 3, 2013 at 7:51 pm |
Hey,
Perhaps I don’t know how things work on this page…I seem to see comments from Tricia replying to those of Trevor yet can’t see any posts from Trevor in ages…?
My guess is that Trish just reads her way through the comments and posts a reply after each, not understanding that the replies are not nested.
Maybe she reads from a feed that uses a different display/layout to that of the website.
Anyway, it makes for a pretty incoherent reading.
LikeLike
Tricia, the sources upon which I rely are those such as the EPA, the CDC, the ADA, the NSF and the WHO, among many others. I also depend on peer-reviewed scientific studies which I seek out and obtain in their entire and original form. Yes, these sources are generally “pro fluoride”, but that’s because they present facts supported by valid evidence, and the valid scientific evidence overwhelmingly supports the safety and effectiveness of water fluoridation. They are the original sources.
Now, contrast this with the sources you use. Antifluoridationist websites such as “fluoridealert.org” are third party sites which obtain information, filter and edit it to fit their position and then post it for those who lack the initiative to seek out accurate information themselves. Third party websites such as these are managed and maintained by unqualified people who haven’t the education, training, or experience to understand what constitutes valid science and what does not. When you use these sites you are not getting accurate, original information, you are getting unqualified, highly biased opinions on what these fluoride opponents want you to believe that the original information means. You are being spoon fed what someone else wants you to believe, instead of being presented with complete, accurate information which you can read yourself and upon which you can base your own, informed opinion.
So, if you consider such sites as the EPA, the the CDC, the ADA, the NSF, and the World Health Organization, to be “pro fluoride” that should tell you something about water fluoridation. They have the knowledge, understanding, and resources to present accurate information in its complete and appropriate context.
Steven D. Slott, DDS
LikeLike
Tricia, dissociation constants are irrelevant. Yes, Sauerhaber presents this argument in an effort to divert attention from the facts of fluoridation, but the point is that both Calcium and HFA release identical fluoride ions into water, regardless of the amount. The concentration of fluoride ions in water is measured prior to addition of any others through fluoridation with HFA. If the concentration of these ions, released by Calcium Fluoride, is equal to or greater than 0.7 ppm, then no more are added. If the existing concentration is less than 0.7 ppm, only enough HFA is added which will raise that concentration to 0.7 ppm. That CaF dissociates at a slower rate than HFA is irrelevant.
Too, it must be borne in mind that Sauerhaber works for “Attorney Deal” as Deal’s “Scientific Consultant”. Deal is the Connett affiliate who is highly involved in futile attempts to initiate lawsuits against fluoridation.
Steven D. Slott, DDS
LikeLike
Tricia, there are countless reasons for gastric distress. There is no valid evidence of gastric distress being caused by fluoridated water. There is no evidence of the massive erosion of the epithelial lining of the gut which would have been rampant throughout the entire history of humans, had the formation of hydrofluoric acid been occurring to any significant degree.
Steven D. Slott, DDS
LikeLike
“That’s nonsense – there is a lot of documented cases of adverse effects of fluoride at .7ppm or thereabouts.”
Ok, Tricia, then produce these “documented cases”. Please stick to that peer-reviewed evidence which is relevant to fluoride at 0.7 ppm.
Steven D. Slott, DDS
LikeLike
Trevor, if you want to rely upon a study from 1958 to support your argument, feel free. As far as your opinion on how best to deliver fluoride prevention, you are not qualified to make that assessment.
From the CDC:
“Both drinking water and toothpaste provide important and complementary benefits. The drinking water provides long low-level protection, but the fluoride in toothpaste is at a high enough concentration that it has additional properties. Whether in water or toothpaste, fluoride works in two main ways: by slowing the activity of bacteria that cause decay, and by combining with the enamel on the surface of the teeth to make it stronger and more resistant to decay. Fluoride in the water, although at a lower concentration than in toothpaste, maintains a constant low level of fluoride in the dental plaque and saliva all day. Toothpaste provides a high level of fluoride, but only for 1-2 hours after brushing, so the water exposure during the remainder of the day takes over after that.”
——http://www.cdc.gov/fluoridation/fact_sheets/cwf_qa.htm#3
Steven D. Slott, DDS
LikeLike
“And the interactions and synergistic effects haven’t even begun to be studied in any realistic way i.e. as it may be happening inside the body with the complexities of human physiology.”
Tricia, as fluoride ions identical to those which already exist in water, and trace contaminants in harmless concentrations, are the only products of fluoridation that are ingested, exactly what “interactions and synergistic effects” do you feel have not been studied sufficiently?
Steven D. Slott, DDS
LikeLike
You guys can’t see my posts because I am always under moderation!!! Everyone else is saying stuff without citations references etc and Ken says nothing about it.
I ask you guys to produce one randomized, prospective ,double blinded, placebo-controlled clinical trial measuring caries increment with calibrated examiners (high kappa scores) who use better a technique than counting DMFTs as a substitute for actual caries measurements (e,g, measuring caries progression with reproducible radiographic techniques).
Until such time those studies are weak evidence at best. Nothing has been proven since there are too many variables e.g. differences in tooth eruption…fluoride delays tooth eruption, Vitamin D differences, poor nutrition, sugar exposure, sealant placement, sugarless chewing gum use, oral hygiene, various topical fluoride home regimens and variable supervision of professional dental care…..all of these have been shown to affect caries rates.
LikeLike
You are not qualified or legally allowed Steve to mass medicate the entire population without their consent. You cannot give fluoride treatments at your office without consent and you cannot do it outside your office either. I do not believe fluoride works to prevent tooth decay in the first place especially when added to the water. Fluoride is an enzyme killer and thus kills the bacteria in the mouth that causes tooth decay. If you want a poison to kill the bacteria, why place it in the water, just use it in toothpaste or swish with it.
It is also acknowledged by dental researchers that fluoride has little effect on preventing cavities in the pits and fissures (chewing surfaces) of teeth – where the majority of tooth decay occurs. Also fluoride does not help prevent baby bottle tooth decay.
LikeLike
Trevor
“I do not believe fluoride works…”
That may be the problem.
I, personally, follow the science and let the experts give me state of the art advice. I don’t have to have any beliefs on whether fluoride works or not.
LikeLike
Hit post too early…
Knowledge suffices for me.
LikeLike
Stuart . . . Baaaaaaa.
LikeLike
Stuart try to find randomized double blind clinical triials showing fluoride is safe or effective you will find there is none. Double blind clinical trials are the gold standard in science to prove something is safe or effective. Also Stuart find one randomized, prospective ,double blinded, placebo-controlled clinical trial measuring caries increment with calibrated examiners (high kappa scores) who use better a technique than counting DMFTs as a substitute for actual caries measurements (e,g, measuring caries progression with reproducible radiographic techniques).
Until such time those studies are weak evidence at best. Nothing has been proven since there are too many variables e.g. differences in tooth eruption…fluoride delays tooth eruption, Vitamin D differences, poor nutrition, sugar exposure, sealant placement, sugarless chewing gum use, oral hygiene, various topical fluoride home regimens and variable supervision of professional dental care…..all of these have been shown to affect caries rates.
LikeLike
Tricia, did it ever occur to you that maybe…you’re wrong?
That maybe the the medical communities actually know more than you because they do the work?
Your ignorance does not magically trump their knowledge.
Making sheep noises doesn’t change that.
LikeLike
Trevor, I’m afraid I don’t understand the relevance of your comment that I am not “allowed to mass medicate the entire population without their consent”. No argument from me there, I know of no one who does have such allowance. I certainly have never claimed to have any such authority. But that is irrelevant to water fluoridated at 0.7 ppm. The decision to fluoridate water supplies is made by state and local governments in the US and similarly in other countries. Fluoride at 0.7 ppm is not a “medication” anyway, thus, any discussions in regard to it being such are irrelevant and moot.
The rest of your claims in this particular comment are simply your unsubstantiated opinion with no valid support provided. Thus, they are also moot.
Steven D. Slott, DDS
LikeLike
Trevor, in regard to your demands for double blind studies, water fluoridation is a public health initiative. As such, any assessments of its effectiveness are made on the basis of effects on the population as a whole, not on individual bases. Due to the halo and other intermingling effects, it is not even possible to segregate a population sufficiently to perform random, double blind studies, such as you and other antifluoridationists demand. However, in assessing the effectiveness of any public health initiative, observational studies are the method of choice. There are countless, peer-reviewed observational studies which demonstrate the effectiveness of the public health initiative of water fluoridation on the prevention of dental decay.
Steven D. Slott, DDS
LikeLike
Cedric, I now see that your original question asked me about “scientific communities” and not “peer-reviewed articles”. For some reason, as I was going back and forth with Steve, reading peer-reviewed journals, I must have gotten extremely lazy reading your comment jumbled it with what Steve and I were talking about. I do apologize. I can see how that would have been a bit maddening.
No. No scientific communities that I know of that explicitly opposes fluoridation, except the EPA Union of Scientists, and you’re probably aware of this example.
http://www.nteu280.org/Issues/Fluoride/NTEU280-Fluoride.htm
What is frustrating is that there is no agreement on how much fluoride is beneficial to be swallowed, or whether the benefit is entirely topical. There is no agreement on this issue, and even dental textbooks say that the precise way that fluoride works is actually still a mystery.
LikeLike
I do apologize. I can see how that would have been a bit maddening.
Ah, it was a case of genuine miscommunication? Ok then. Thanks for clearing that up.
No. No scientific communities that I know of that explicitly opposes fluoridation…
A straight answer? Thank you again. You are the first.
Seriously, you are the first. I’m impressed.
, except the EPA Union of Scientists, and you’re probably aware of this example.
That’s a…union. I was referring to scientific communities. I think we both know that the actual EPA does not reject the scientific consensus on fluoride, just like every single scientific community on the planet-unions not withstanding.
I came across the issue of fluoridation trying to answer the question “how much fluoride should my one year old and 3 year old have, and quickly found that there is widespread disagreement. Here is a 2009 study that deals…
If there’s “widespread disagreement”, then why are there no scientific communities on the planet that reject the scientific consensus?
Logically, there should be dozens at least.
Yet they don’t exist.
Here is a 2009 study that deals…
Sure. Yet the scientific communities also read those same studies.
None of them reject the scientific consensus.
You have to factor that in rather than ignore it.
You have hunted for and discovered an anomoly. Here’s a study and there’s a study and another one over there. You are convinced that that there’s “widespread disagreement”.
Fine.
But there’s all these scientific communities out there that make it their business to understand fluoride in the water and they seem to very secure in their position.
Now there are two choices; either they are all wrong or you are wrong.
Have you considered that you might simply be wrong?
Or…there is one more sinister possibility.
It’s a global scientific conspiracy.
(…insert de eeeebil music here…)
People do this with climate change.
Did you know that climate change deniers like to pretend that there is no scientific consensus on climate change?
They do.
They have some wonderfully creative excuses and rationalizations as to why it doesn’t count or doesn’t even exist.
They go anomoly hunting too.
In the same way that you go after some study and search for details that confirm your bias, so to the climate deniers nit those picks in the IPCC reports.
If your methodology is aping exactly what the climate deniers do then that’s bad. Very bad. Whatever it is that you do should be better quality that what they do, agreed?
(Happy to provide you with fresh living examples of what I mean, if you like.)
I don’t sweat the small stuff.
Life is too short and nutters of all shapes and sizes are in plentiful supply.
I find it much simpler to congratulate the science denier on the fruits of their investigation, give them the benefit of the doubt and then go from there.
Ok, you have found “something”? I see. Something is wrong or something is contradictory or something is suspicious or poor quality etc, etc etc.
Whatever.
Fine. Let’s work with that.
So…Given that you have found “X”, can you name a single scientific community that rejects the scientific consensus on climate change, evolution, germ theory, vaccines, the moon landings, the cancer risks of smoking etc?
(…awkward silence…)
It cuts to the chase very nicely.
Some nutter who rejects the scientific consensus on climate change?
Widespread disagreement? Really?
Hmm, you don’t say?
(…Cedric goes to check out the NASA website…)
Job done.
It’s all there in plain English.
http://climate.nasa.gov/scientific-consensus
LikeLike
For those John Colquhoun fans, I wouldn’t believe everything he says:
LikeLike
Ken… can we seriously seriously believe dental fluorosis (however minor) is the first effect or first sign of F toxicity …it may be the 1st outward sign…..to find if F is so safe need to test on humans preferably, which we have been doing for a long time without proper controls /assessment of the effects
That;s why the above arguments continue until a scientific method is devised where the only variable is the amount of F added to the diet, Then a method to decide what is the first signs of change or toxicity ( I think it is agreed that F is toxic) Until such testing is done F will continue to create controversy
Then someone has to determine what safety factor is required to prevent hypersensitive / people who are not average consumers eg drinking only 2-3 litre of water (Thanks for that Steve) Athletes, people in hot climates labours etc may consume more.
If “additive a” is 4 ppm shows toxic signs, can you as the qualified researcher please tell us what level it should be allowed in food/water
LikeLike
“people in hot climates”
Just to note that that cities lower the fluoride ppm down in hotter cities (closer to the 0.7ppm).
LikeLike
Ian, you seem to passionately want fluoride to be toxic.
So far the only credible effect of F at fluoridation levels of 0.7 a 1.0 ppm has been very mild or questionable fluorosis. It is debatable that one should call this a “toxic” effect as it presumably has been a common feature of teeth through the centuries and is harmless. Just because there might be other effects which have not yet been shown is not proof that there are other effects.
Your comments about a theoretical experiment apply to any other elements just as much as they do to fluoride.
As for hypersensitivity can you provide any evidence that any more people are hypersensitive to f than are to water or Cl2? And there does seem to be good evidence that many of the claims of hypersensitivity are psychosomatic.
>
LikeLike
Shane, I am moderating comments that do not provide details when they refer to publications. Could you please repeat with a reference, citation and/or link to the Waldbott paper?
I am doing this to discourage poor citing and in the interests of the useful discussion which arises when people have the right information.
LikeLike
Ian, in regard to your question as to what amount of fluoride should be allowed in water…… in the United States that maximum amount is currently 4.0 ppm as set by the EPA (MCL for fluoride). The 2006 NRC Committee on Fluoridation recommended that this maximum amount be lowered due to the increased risk of moderate/severe dental fluorosis and bone fracture with chronic, long-term ingestion of water with a fluoride content of 4.0 ppm or greater. The NRC Committee made no recommendation on the EPA secondary MCL of 2.0 ppm fluoride, thus deeming this level to adequately protective if the health of the public. Water is fluoridated at 0.7 ppm, one third the level that the NRC Committee deemed safe.
Steven D. Slott, DDS
LikeLike
Ian, you seem to passionately want fluoride to be toxic.
Well I think we both agree F is toxic, its just a matter of concentration (ppm in water) So the thing I’m passionate about is that it be tested appropriately and a true safe level can be determined…thus end 50+ years of controversy
Ken ….very mild or questionable fluorosis ….debatable that one should call this a “toxic” effect as it presumably has been a common feature of teeth through the centuries and is harmless.
So I guess the question to you would be regarding fluorosis what effect by F on human body function or symptom would illustrate toxicity to you
As to hypersensitivity if as you as say if people have this problem with Chlorine (Cl2) then you would expect similar reactions with F remember F is more reactive then the other halogens (Cl2, Bromine, Iodide) But delete the word “hypersensitive” from my previous comment
LikeLike
Ian, as you are the one alleging toxicity of fluoride at 0.7 ppm, it is up to you to provide substantiation for such a claim, it is not up to others to provide proof of a negative. Antifluoridationists constantly use the tactic of alleging disorders associated with fluoridation, with no substantiation, then demanding proof that these disorders do not occur. This is an endless process and is not valid science.
Steven D. Slott, DDS
LikeLike
Cedric, I actually read through (skimmed) the dialogue you had with the climate change denier a few days ago before the fluoride debate started. I was curious what a recent version of the argument against climate change might look like… I kept scrolling and scrolling, waiting to get the argument or explanation, and like you said… there was none. I really wasn’t able to ascertain the what exactly his argument was or why he felt it was important to argue against climate change… but I think you’re right. It basically comes down to fitting the climate change issue into some larger view of a sinister world order trying to fool everyone. Certainly there is plenty of room to criticize and refine the details of and strategy for what we should do about global warming…
But anyway, I don’t see a parallel between opposition to fluoridation and denial of global warming. I’m not afraid of the facts, so I’m not trying to pick studies to prove a point and I have no reason to try and hide the fact that fluoridation has a long list of endorsements. However, it takes a long time for science to effect public policy, and I think you’re over estimating the energy that goes into evaluating fluoridation. It is not on the top of most of these organization’s priority list and most doctors and dentists have no idea that fluoride based pesticides are being used so much. In fact, there is a big issue with sulfuryl fluoride right now because the EPA decided to phase it out as a pesticide due partially to its role as a greenhouse gas and partially to the fact that some Americans are already over exposed to fluoride (based on dental fluorosis data). Dow Chemical is now trying to override this decision by tacking on an amendment to the farm bill…
Anyway, I personally think that fluoride exposure is slowly increasing in the United States, due largely to pesticide use, and that we may be at a crossroads where water fluoridation doesn’t make sense. The situation may be different in NZ. I do not think it fits into any larger world view.
Here are a few more studies that deal with the issue of systemic and topical exposure to fluoride. I am not claiming that these studies reject fluoridation, just that they show some disagreement. For me, as a mother who doesn’t particularly like the the way fluorosis looks but who wants to protect my kids from cavities, this is relevant and important.
Here is one that discusses the evolving scientific consensus and debate about how fluoride works…
http://www.karger.com/Article/Pdf/77764
Systemic versus Topical Fluoride,
Abstract
The actual mechanism of fluoride action is still a subject of debate. A dogma has existed for many decades, that fluoride has to be ingested and acts mainly pre-eruptively. However, recent studies concerning the systemic effect of fluoride supplementation concluded that the caries-preventive effect of fluoride is almost exclusively posteruptive. Moreover, epidemiologists have cast doubt on the validity of the ‘old’ studies dealing with fluoride use….
This study talks about the wide range of fluoride intake and notes the fact that some children ingest more fluoride from toothpaste alone than is recommended for the entire day from all sources (this is the same author of the 2009 study. I should mention that he supports water fluoridation, but also encourages careful monitoring of fluoride from all sources. He is the head of the Iowa Fluoride Study and a widely recognized expert on the subject):
http://www.ncbi.nlm.nih.gov/pubmed/10553251
Here is a study that clarified that the primary role of fluoride is topical. Again, I’m not saying that the author is against fluoridation. I’m saying that the role of fluoridation is a considered to be topical benefit of fluoride by most experts who are on top of the research.
http://www.ncbi.nlm.nih.gov/pubmed/10086924
Here is a link that includes the CDC report saying the same thing about topical fluorides and the changing understanding of the science. It also includes the Featherstone on topical fluoride as the cover story for the Journal of the American Dental Association
LikeLike
Can fluoride cause fluorosis in existing teeth or does it cause lfuorosis only during pre-eruptive formation of enamel?
anybody?
LikeLike
Alison, I am briefly dealing with the topical vs systemic issue in my response to Paul. It should also be covered in his next article and my response to that.
I don’t think there is any controversy about the predominant surface mechaism of F in protecting existing teeth. The word “predominant” is important as anti-fluoride people tend to omit and purposely imply “only.” The “existing teeth” is also important as there is still understood to be an effect on pre-erupted teeth. Then there is the beneficial effect on bones. Both of these require F ingestion.
A final, and very important, point is that fluroidated water operates by this topical mechanism. Very effectively because regular drinking means that concentrations of F in saliva are maintained at useful levels. In contrast toothpaste raises the concentration less frequently. So toothpaste and fluoridated water tend to be complimentary rather than substitutes.
LikeLike
Yes, Ken. I have read all those studies, so I understand the full argument. That’s why I specifically mentioned that the authors were not opposed to fluoridation, but that our understanding has evolved. By this reasoning, the fluoride present in fruit juices, wines, teas, and other foods would also have the same effect on fluoride concentrations in saliva, correct?
LikeLike
I think it is only during the pre-eruptive stage. Mind you, high F levels may be different.
LikeLike
Yes, food and other beverages will contribute.
There are studies estimating the relative importance of different forms of intake and water/beverages seems to still be the major one. But it could be changing and also dependent on diet. I don’t eat red meat but do eat fish so hope I get my F that way.
LikeLike
That’s correct, Ken. Dental fluorosis only occurs during tooth development. That’s why the upper limit of daily fluoride takes such a big jump after age 8. O-8 are the tooth forming years when fluorosis can occur, so the upper limit is lower during that time, solely for that reason. After age 8, the teeth are formed and the upper limit therefore jumps to 10 mg per day.
Steven D. Slott, DDS
LikeLike
Alison, the issue of systemic versus topical is simply a diversion from the facts of water fluoridation. Exposure of the teeth to low concentrations of fluoride all during the day is a very effective means of dental decay prevention. Water fluoridation is by far the most cost-effective means to attain this. The effect of fluoridation is both systemic and topical, but what percentage is one or the other is moot in terms of effectiveness of this public health initiative. At less than $1 per person per day for fluoridation, there is no other means of delivering this type of protection that even comes close to the efficacy and cost effectiveness of water fluoridation.
Steven D. Slott, DDS
LikeLike
Sorry, that’s $1 per person per YEAR, for fluoridation, not per day as I mistakenly stated in my previous comment.
Steven D. Slott, DDS
LikeLike
Cedric, I actually read through (skimmed) the dialogue you had with the climate change denier a few days ago before the fluoride debate started. I was curious what a recent version of the argument against climate change might look like… I kept scrolling and scrolling, waiting to get the argument or explanation, and like you said… there was none. I really wasn’t able to ascertain the what exactly his argument was or why he felt it was important to argue against climate change… but I think you’re right. It basically comes down to fitting the climate change issue into some larger view of a sinister world order trying to fool everyone.
Thank you for looking at that. It serves as a wonderful example of how these people think.
But anyway, I don’t see a parallel between opposition to fluoridation and denial of global warming.
It’s about the methodology. Look at what the anti-fluoridationists do.
Now look at what the climate deniers do.
They’re the same.
Sure, one’s talking about fluoride and one’s talking about the climate but that only a difference in labels.
You can take what one says and then put it in the mouth of the other and nobody would spot the difference.
Climate deniers have the same problem as HIV deniers.
They are both denying the scientific consensus on their respective topics.
HIV deniers have the same problem as creationists.
They are both denying the scientific consensus.
The same goes for a host of other nutters out there.
Anti-vaxxers, moon landing deniers, tobacco deniers etc.
Because they have the same problem…they reach for the same solutions.
I’m not afraid of the facts, so I’m not trying to pick studies…
Anybody could say that. I’m not saying that you personally don’t believe it but it’s the kind of self-reassuring statement that any HIV denier, vaccine denier, climate denier might come up with.
Methodology.
However, it takes a long time for science to effect public policy, and I think you’re over estimating the energy that goes into evaluating fluoridation.
Methodology.
You are now rationalising away the scientific consensus on fluoride.
I can’t just meekly take your word on this. There’s no reason for me to do so. You are trying to “interpret” for me. I somehow don’t understand how “it really works”. All those scientific communities are doing something wrong and you’ve got one up on them. Thank goodness you’re here to give me the inside info and set me straight. Lucky me.
No.
I wouldn’t talk to you like that and you should do me the same courtesy.
A science denier talks like that all the time.
Look at your methodology. It’s indistinguishable from the nutters.
Look at how the anti-fluoridationists go about propogating their ideas.
It’s exactly the same.
Anyway, I personally think that etc, etc,…
Climate deniers say the same thing. Only their thinking tends not to (surprise, surprise) match up somehow with the consensus.
Here are a few more studies that deal…
Why are you doing this?
That’s not a rhetorical question.
I’m deadly serious.
Why are you doing this?
Look at your methodology.
Are you aware that climate deniers pick studies too and then offer them up as proof of something or other?
“I am not claiming that these studies reject climate change, just that they show some disagreement. For me, as a mother who doesn’t particularly like the the way the IPPC looks but who wants to protect my kids, this is relevant and important.
Here is one that discusses the evolving scientific consensus and debate about how climate change works…
The actual mechanism of climate is still a subject of debate. A dogma has existed for many decades, that mankind somehow affects the climate However, recent studies concerning concluded that the rise in temperatures of climate is almost exclusively natural. Moreover, respected scientists have cast doubt on the validity of the ‘old’ studies dealing with man-made climate change….
I’m going to say this again because it’s important.
Methodology.
Look closely at the methodology of the science deniers.
All of them.
They fit certain specific patterns.
Their methodology is the same.
You can strip the labels off and swap them around and nobody would notice the difference.
If you are doing what the climate deniers are doing then you are endorsing their arguments. That should disturb you greatly.
You should be better that they are.
Adopt a methodology that is genuinely incompatible with climate denialism or any other science denial out there.
Can you do it?
Michael Specter: The danger of science denial
LikeLike
Thank you Ken and Steve re when formation of fluorosis occurs.
Steven,
I have recently moved to a rainwater supply from 35Kl tank. Are you aware of DIY home-fluoridation set ups or kits?
All I see in a brief internet search are systems to filter it out.
LikeLike
Dear Steven D Stott DDS
Presumably that “climate change denier” that you refer to is me,
I do not deny Climate change, but never mind, I don’t mind the label. I have my own labels for guys like Cedric.
I actually have lots of arguments, but I don’t tend to air them on blogs like this because it confuses the locals.
I really like to probe the locals to see if they actually have any knowledge of the topic at all.
The simple answer is no.
Appeals to authority is all they have .
I hope that is helpful, Steven D Stott DDS
LikeLike
Steve you said “Ian, as you are the one alleging toxicity of fluoride at 0.7 ppm, ”
I’m not alleging .07ppm or any other concentration is toxic that’s the whole point ..what I am alleging is the proper test/s to determine what the MCLG has not been done but needs to be done
So if you like I would be happy to start a fund with a small contribution (say $100) to get crucial testing started so all information about F is basis on valid science
LikeLike
Ian, we already have the information you talk about. We are sufficiently confident of the safety of F at concentrations used in fluoridation got recommend it to local bodies. You are stubbornly choosing to interpret lack of evidence of negative effects from this research as lack of work – you won’t be satisfied until this research does turn up a negative effect.
The world just doesn’t work that way – and just as well as that attitude would have resulted in the extinction of our species long ago.
LikeLike
Still making wild bizarre claims I see Ken . . . :}
LikeLike
Yet another fail from the blog’s resident troll, Andy.
Andy, if you are going to have a go, make sure you identify your target correctly.
LikeLike
Andy’s quite famous.
Perhaps he’ll be good enough to recount his “Daily Currant” moment?
Comedy gold.
LikeLike
Well I look forward to your revelation
LikeLike
“It’s about the methodology. Look at what the anti-fluoridationists do.
Now look at what the climate deniers do.
They’re the same.
Sure, one’s talking about fluoride and one’s talking about the climate but that only a difference in labels.
You can take what one says and then put it in the mouth of the other and nobody would spot the difference.”
Let’s test that shall we?
We shall.
I do not deny fluoridation, but never mind, I don’t mind the label. I have my own labels for guys like Cedric.
I actually have lots of arguments, but I don’t tend to air them on blogs like this because it confuses the locals.
I really like to probe the locals to see if they actually have any knowledge of the topic at all. The simple answer is no.
Appeals to authority is all they have .
Yep, one size fits all.
Works for the moon landings too.
I do not deny the moon landings, but never mind, I don’t mind the label. I have my own labels for guys like Cedric.
I actually have lots of arguments, but I don’t tend to air them on blogs like this because it confuses the locals.
I really like to probe the locals to see if they actually have any knowledge of the topic at all. The simple answer is no.
Appeals to authority is all they have .
Insert your personal favourite label and rinse and repeat. Evolution, vaccines, etc.
Why even on this very thread, we have a live example:
StuartG | November 4, 2013 at 6:52 am |
I, personally, follow the science and let the experts give me state of the art advice. I don’t have to have any beliefs on whether fluoride works or not.(..)Knowledge suffices for me.
Tricia Cheel | November 4, 2013 at 7:05 am |
Stuart . . . Baaaaaaa.
Looks like Tricia and Andy have a lot in common. The mentality is identical.
LikeLike
Cedric, good points about science deniers and methodology. The bottom line with most deniers is that their objections are grounded in personal ideology, not science. They pick and choose the science to match their ideology, not the other way around. Thus, no matter how much science is presented to them, it will not make one iota of difference. Connett is no different. He makes the same invalid arguments that antifluoridationists have been making for decades. He just cloaks them in updated terms and cherry-picks newer “studies” which bolster his personal ideology against water fluoridation.
Steven D. Slott, DDS
LikeLike
Richard, I am not personally aware of any home fluoridation systems. Generally, pediatric dentists will prescribe fluoride supplements for those whose primary water supply is not fluoridated. This is not as effective as water fluoridation, but is better than nothing. The best idea would be to check with your local dentist and/or pediatrician to get their recommendations.
Steven D. Slott, DDS
LikeLike
Ian, you are simply presenting the argument for more testing of fluoridation which is one of the arguing points found on most antifluoridationist websites. As HFA immediately and completely dissociates upon addition to drinking water, this would amount to nothing more than testing of the fluoride ion, which humans have been ingesting since the beginning of time in the same concentration range as exists in fluoridated water. Yes, Antifluoridationists have attempted to push the EPA to a zero MCGL for fluoride, but saner heads have always prevailed in that argument and the primary and secondary MCGLs for fluoride have remained at 4.0 ppm and 2.0 ppm respectively.
The 2006 NRC Committee on Fluoridation did an exhaustive, 3 year review of all the relevant scientific literature on fluoride. After this review, they recommended lowering the primary MCL down from 4.0 ppm for the sole reason that chronic, long-term ingestion of water with a fluoride content of 4.0 ppm, or greater, increases the risk of moderate/severe dental fluorosis, and bone fractures. They made no recommendation on the secondary MCL of 2.0 ppm., thus deeming that maximum level to be adequately protective of the health of the public. Water is fluoridated at 0.7 ppm, one third the level deemed safe by the 2006 NRC Committee in Fluoride. This is your answer.
Given the broad margin of safety between fluoride MCL and upper limit of daily fluoride ingestion, and that water is fluoridated at the miniscule level of 0.7 ppm, there is no need to narrow down any further.
Steven D. Slott, DDS
LikeLike
Sorry, should’ve read “MCLG” not “MCGL”.
Steven D. Slott, DDS
LikeLike
Andy, no, I have not referred to you or anyone else as being a “climate change denier”. You must be mistaking me for someone else.
Your comment about the locals having only “appeals to authority” does, however, reinforce my point about antifluoridationist objections being grounded in personal ideology and not science. No matter how much valid science is presented to you, in regard to fluoridation, you will always deny it.
Steven D. Slott, DDS
LikeLike
Ok, Cedric. That is fine. You are not interested in discussing fluoride, because you actually came here to test your theory that all fluoridation opponents are just like climate change deniers.

It is really quite simple. The CDC says that some children are getting too much fluoride. They say it in that too much fluoride has caused very mild dental fluorosis in about 40% of adolescents.
Dental researchers say that some kids get too much fluoride from toothpaste alone. My 3 year old, like many of them, is terrible at spitting. I would like to use fluoride toothpaste, but worry that if I use fluoridated tap water for all our cooking and drinking in addition to the fluoride toothpaste, he is likely to get fluorosis.
Steve and Ken insist that fluorosis can only be identified by a professional. This is not true. It is easy to detect for anyone who knows what it is. The scientific community does not share Ken and Steve’s suggestion that we might want more people to have fluorosis, nor that it is a desirable thing. Further, society does not share the view that fluorosis looks good. When I see people with dental fluorosis I used to think they just had stains on their teeth from poor hygiene or smoking but I now know that this is often not the case. People do not want stains on their teeth. Maybe science will eventually convince us all that we do, but for now, the consensus is that we don’t like the way it looks. This is the picture that the US CDC cites as one example of the VERY MILD variety. So there you have it. A classic science denier’s argument as revealed by a mother who likes her white teeth and doesn’t want stains on kids’ teeth.
LikeLike
I also care a great deal about protecting the environment in Central Florida, where I lived for 5 years while I attended Stetson University. If fluoridation is to continue, we will have to find a more sustainable source of fluoride. The phosphate fertilizer industry, by most accounts, represents a major threat to the Florida eco-system. In order for Mosaic to continue to furnish us with inexpensive HFSA, their mines will have to continue to expand into the Peace River watershed in Central/Southern Florida. Perhaps Ken, with his background in soil research, will touch on the impacts of the overuse of phosphate fertilizers and the problem with strip mining.
Here is a quote from this article, which explains why phosphate mining is a problem. http://e360.yale.edu/feature/phosphate_a_critical_resource_misused_and_now_running_out/2423/:
“Phosphate strip mines are environment wreckers. They produce around 150 million tons of toxic spoil a year. Their massive draglines, huge slurry pipes, and mountainous spoil heaps dominate the landscape for tens of miles in key mining zones…. The world’s largest mine is at Four Corners in an area known as Bone Valley in central Florida. The Four Corners mine covers 58,000 acres, an area five times the size of Manhattan…. As the drag mines move south in Florida, anger has been growing about the environmental impacts. A million tons of mine waste, containing lows levels of radioactivity, are already piled up at dump sites around the state, and disputes are growing over promised mine cleanups. Rivers have dried up, and settling ponds have leaked.”
This is the specific plant that HFSA originates from before it comes to my water company (the water company has been entirely helpful and open and have shared all certificates of analysis, which state the source as the Riverview, Florida phosphate plant, owned by Mosaic). The company was recently cited by the EPA for exceeding the new standards set for sulfur dioxide emissions. I think it is unfortunate that one of our drinking water additives depends on a process that is a major source of Tampa smog. I would prefer to pay a higher rate for fluoride additives and source it locally.
http://www.tampabay.com/news/environment/airquality/riverview-phosphate-plant-flunks-new-air-pollution-standard/2134793
LikeLike
Ok, Cedric. That is fine. You are not interested in discussing fluoride, because you actually came here to test your theory that all fluoridation opponents are just like climate change deniers.
Do you need any extra straw to build that strawman?
Focus.
It all comes down to methodology.
What are you doing that is so very different from the climate deniers?
You want me to look at studies?
Well, this may come as a shock to you but climate deniers want me to look at studies too.
Happens all the time. It’s a standard shtick.
How did you come by these studies? Do you subscribe to scientific journals?
Most people don’t.
So…how did those particular studies pop up on your radar?
Probably you found these studies with a bit of help, yes?
Guess how the climate deniers come by their studies?
(…thoughtful pause…)
Yep. They do what the anti-fluoridationists do. And they justify it the same way.
It all comes down to methodology.
It is really quite simple. The CDC says…
No. Don’t do that.
Don’t “helpfully interpret” what the CDC does or does not say on the subject of fluoride.
I don’t get my science information second-hand.
If I want to find out what the CDC has to say on fluordie then I’ll go straight to their website and find out for myself.
I don’t need you to cherry-pick some particular section and ignore the rest.
It’s the same thing with climate deniers. They tell me all sorts of things about NASA. You wouldn’t believe some of the babble they come up with.
To cut through the fog, I just go to the NASA website and it’s all there in plain English.
I think we both know that I can do the same with the CDC and get the same positive results.
I would like to use fluoride toothpaste, but worry that if I use fluoridated tap water for all our cooking and drinking in addition to the fluoride toothpaste, he is likely to get fluorosis.
Does your child have some special weakness?
Does he suffer from Trica syndrome or something?
I should hope not.
The health authorities are not trying to poison your child.
The scientific communities are not your enemy.
They’re not hiding anything. There’s nothing wrong or bad or strange going on.
They are doing their job. Just like the community they serve expects them too.
It’s very easy to go to the CDC and see that water fluoridation is fine and has been for many decades now.
You’ve been listening to the wrong crowd. Your methodology is screwy and your concerns are unfounded.
The anti-fluoridationists are playing on your fears. You shouldn’t let them manipulate you with crude propoganda. It really shoddy stuff. It’s all McCarthyism era nonsense. Very retro.
Why would you be content to adopt the methodology of the climate denier nutters out there? Surely the dental health of your family and that of your community is worth more than that. This is not a game. If you can be sucked in by one disinformation campaign then that same path leads you to others.
Today the topic is fluoride. Tomorrow it could be vaccines. The day after that, who know?
If you use a methodology or an argument, then you endorse it.
Look at your methodology.
Tell me how it’s any different from the science deniers out there that we both know exist.
tobacco_papers
LikeLike
Alison, there are multiple factors that cause discoloration of teeth, fluorosis being but one. As you can see from the close-up CDC picture you cite, mild dental fluorosis is barely detectable, with even these faint markings disappearing over time. If you can spot these faint spots at a normal speaking distance under normal lighting then you have the eyes of a hawk and are looking specifically for them, neither of which normally occurs in everyday life.
I did not state that we might want more people to have fluorosis, nor did I state that fluorosis “looks good”. What I stated was that as Kumar, et al, have demonstrated mildly fluorosed teeth to be more resistant to decay, that some do not consider this effect to even be undesirable, much less adverse. If you want to trade the dental decay preventive benefit for your child’s teeth in order to reduce the risk for development of these faint markings, that’s certainly your purview. However, others believe the protection against decay far outweighs these nearly undetectable white areas. From a strictly esthetic perspective, dental decay is far more esthetically undesirable than are these markings. I can tell you that having practiced dentistry in a fluoridated community surrounded by fluoridated communities for 32 years, I have as yet to see one single case of dental fluorosis, attributable in any manner to fluoridated water, which would be detectable outside of close examination in my dental chair. Anecdotal, yes, but anecdotal from a dental professional who treats thousands of patients per year.
The 2006 NRC Committee on Fluoride did not classify mild to very mild dental fluorosis as an adverse effect. That fluoridation opponents desperately want it to be so is indicative of the total lack of any other adverse effects that they can attribute to water fluoridation.
Here is the Kumar study:
http://jada.ada.org/content/140/7/855.long
The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren
Hiroko Iida, DDS, MPH and Jayanth V. Kumar, DDS, MPH
Steven D. Slott, DDS
LikeLike
Alison, you do realize that the strip mining, smog, and whatever other concerns you cite in regard to phosphate mining will occur regardless of whether HFA is recovered or not, correct? Phosphoric acid is the other co-product of this process, with that substance being utilized in soft drinks and fertilizers predominantly. Recovery of HFA from this process, to be utilized in a productive manner, rather than allowing it to be unused and discarded, is just good conservation and utilization of our natural resources. It is not causing any detriment to the environment.
Steven D. Slott, DDS
LikeLike
Alison, maybe you are aware of the recent fluoridation battles in Tampa and its nearby neighbor, Brooksville. Tampa reinstated fluoridation after it was briefly interrupted by the local city council in 2011. Brooksville has a staunch antifluoridationist mayor who nearly single handedly ceased fluoridation of that community two years ago, with no prior notice to the community of an impending consideration by her council. This decision was recently overturned by the Brooksville City Council over the zealous objections of the mayor. She had the full support of FAN and nyscof during her tenure, and even went so far as to give Paul Connett a full hour and a half in front of her council, in late September of this year, allowing no one else to speak in rebuttal. In the end, after considering Connett’s arguments as opposed to those of the scientific and healthcare community, the Brooksville Council voted 4-1 to reinstitute fluoridation to that community, the sole dissent being the disgruntled mayor.
Steven D. Slott, DDS
LikeLike
She had the full support of FAN and nyscof during her tenure, and even went so far as to give Paul Connett a full hour and a half in front of her council, in late September of this year, allowing no one else to speak in rebuttal. In the end, after considering Connett’s arguments as opposed to those of the scientific and healthcare community, the Brooksville Council voted 4-1 to reinstitute fluoridation to that community, the sole dissent being the disgruntled mayor.
4-1?
After an hour and a half of Connett with no rebuttal?
Ouch.
That must have left a mark.
LikeLike
Connett and the mayor tried their utmost to badger a local pediatric dentist, who is more knowledgeable on fluoridation than Connett, to debate, “Presidential style”. The ped dentist said no no to that, but would be more than willing to present either before or after Connett. They refused anything other than a debate, and ended up refusing to let anyone else speak at that meeting other than Connett.
Yeah, I’m pretty sure that nyscof and Connett are stinging after that one.
Steven D. Slott, DDS
LikeLike
Cedric, you hit the hail squarely on the head. Why in the world would any intelligent person need a third party website to tell them what the CDC, the EPA, or the WHO says, when with just a click if the mouse they can access that information directly from the original source? There is but one reason that people attempt to steer readers to third party websites, instead of original sources…….to intentionally deceive.
Steven D. Slott, DDS
LikeLike
Connett and the mayor tried their utmost to badger a local pediatric dentist, who is more knowledgeable on fluoridation than Connett, to debate, “Presidential style”.
They crave the limelight and the respectability.
It’s a wonderful photo opportunity…for them.
Sharing the same stage with the real health authorities is an automatic win for the science denier.
The uninformed public looks at it, gets confused and feels that something serious is going on.
It will come as no surprise to some readers that the creationists and the science deniers and and the anti-vaxxers do exactly the same thing.
Which is why scientists routinely refuse.
Some of them refuse spectacularly well….
Dear Dr. Klinghoffer:
Thank you for this interesting and courteous invitation to set up a
debate about evolution and creationism (which includes its more
recent relabeling as “intelligent design”) with a speaker from the
Discovery Institute. Your invitation is quite surprising, given the
sneering coverage of my recent newspaper editorial that you
yourself posted on the Discovery Institute’s website:
However, this kind of two-faced dishonesty is what the scientific
community has come to expect from the creationists.
Academic debate on controversial topics is fine, but those topics
need to have a basis in reality. I would not invite a creationist
to a debate on campus for the same reason that I would not invite
an alchemist, a flat-earther, an astrologer, a psychic, or a
Holocaust revisionist. These ideas have no scientific support, and
that is why they have all been discarded by credible scholars.
Creationism is in the same category.
Instead of spending time on public debates, why aren’t members of
your institute publishing their ideas in prominent peer-reviewed
journals such as Science, Nature, or the Proceedings of the
National Academy of Sciences? If you want to be taken seriously by
scientists and scholars, this is where you need to publish.
Academic publishing is an intellectual free market, where ideas
that have credible empirical support are carefully and thoroughly
explored. Nothing could possibly be more exciting and electrifying
to biology than scientific disproof of evolutionary theory or
scientific proof of the existence of a god. That would be Nobel
Prize winning work, and it would be eagerly published by any of the
prominent mainstream journals.
“Conspiracy” is the predictable response by Ben Stein and the
frustrated creationists. But conspiracy theories are a joke,
because science places a high premium on intellectual honesty and
on new empirical studies that overturn previously established
principles. Creationism doesn’t live up to these standards, so its
proponents are relegated to the sidelines, publishing in books,
blogs, websites, and obscure journals that don’t maintain
scientific standards.
Finally, isn’t it sort of pathetic that your large, well-funded
institute must scrape around, panhandling for a seminar invitation
at a little university in northern New England? Practicing
scientists receive frequent invitations to speak in science
departments around the world, often on controversial and novel
topics. If creationists actually published some legitimate science,
they would receive such invitations as well.
So, I hope you understand why I am declining your offer. I will
wait patiently to read about the work of creationists in the pages
of Nature and Science. But until it appears there, it isn’t science
and doesn’t merit an invitation.
In closing, I do want to thank you sincerely for this invitation
and for your posting on the Discovery Institute Website. As an
evolutionary biologist, I can’t tell you what a badge of honor this
is. My colleagues will be envious.
Sincerely yours,
Nick Gotelli
P.S. I hope you will forgive me if I do not respond to any further
e-mails from you or from the Discovery Institute. This has been
entertaining, but it interferes with my research and teaching.
(Link)
LikeLike
Cedric, you’re correct, this parallels antifluoridationists such as Connett to a “T” !! Change a few words and this most certainly could have been a response to Connett.
One commenter stated a while back that asking healthcare providers to debate Connett is like asking NASA to debate an astrologer.
Steven D. Slott, DDS
LikeLike
You dental people are just so rude, abusive and arrogant that I wonder anybody even tries to debate anything with you . . . I certainly think for any ‘debate’ to work it needs an independent mediator who will cut this sort of constant ridicule you indulge in as Ken obviously is so one-eyed about it . . . :}
LikeLike
Alison: This is the picture that the US CDC cites as one example of the VERY MILD variety.
Those teeth look great. Why anybody with teeth like that would think their life is ruined (looking at you Core) escapes me.
I’m beginning to suspect all this dread and paranoia regarding fluorosis has some foundation in cultural values, in particular N America, land of Donny Osmond / TV presenter dental work.
LikeLike
You dental people are just so rude, abusive and arrogant that I wonder anybody even tries to debate anything with you
Trish, put away your brolly and calm down.
It is you who refuse to engage, you who refuse to acknowledge any questions etc regarding your unreferenced claims and assertions. You haven’t the high ground to be outraged because people call you out on faulty mathematics and misunderstanding of chemistry etc.
LikeLike
Tricia, debates are all about the debaters, not the issues. Candidates for public office are evaluated for how they act and react as much as they are for their stances on issues. Therefore, debates are appropriate in the political arena. Healthcare issues are evaluated on science and validity. The debaters themselves are irrelevant and little more than an unnecessary distraction which can easily lead to undesirable results for the affected populace. Paul Connett knows that his science is weak and thus depends on his debating abilities to overcome this weakness and to further his own personal views. Were he a true scientist in search of the truth, he would do legitimate research, submit his findings for proper peer-review, and follow wherever that took him. To constantly seek to turn the issue of water fluoridation into a circus sideshow exposes his penchant for showmanship over truth and accuracy. The people whom he hurts the most with such misguided efforts are those for whom I have provided low cost and free dental treatment for the majority of my dental career. They are the population for whose improved access to care I have advocated loudly and publicly for well over the past decade, to the chagrin and alienation of my dental leadership.
So, needless to say, I have very little patience with you, Paul, and all other antifluoridationists who seek to further their own personal ideologies, at the expense of those who need our help the most. Instead of seeking to create sideshows and sell his book, Paul needs to get out of the way and let those of us who are actually in the trenches fighting the battle against rampant, untreated dental disease, do what we know how to do far better than he purports to know.
If you truly want to know what I am all about:
http://www.ada.org/news/1284.aspx
Steven D. Slott, DDS
LikeLike
Tricia says:
<emYou dental people are just so rude, abusive and arrogant that I wonder anybody even tries to debate anything with you . . . I certainly think for any ‘debate’ to work it needs an independent mediator who will cut this sort of constant ridicule you indulge in as Ken obviously is so one-eyed about it . . . :}
Indeed. Just substitute “dental people” for “climate change activist/atheist/etc
Just the labels change, the methodology and the language is the same.
LikeLike
Tricia, as the moderator I expect flack from some people because I am trying to stop certain bad habits that are rife among commenters on the fluoridation issue. So I will understands your comment accordingly – not that I have had to stop any of your comments. Just that you feel hard done by because you have not been prepared to answer questions out to you. Well life, especially in the Internet, is hard.
This exchange is of course only a “debate” in name. We are not indulging in a gladiatorial sport but simply exchanging and critiquing views, as scientists, on the fluoridation issue. This exchange is between Paul and me – not directly with commenters – although I enjoy getting into comment discussions myself.
Frankly in these sort of discussions I have noticed that the rudeness tends to come mainly from one side. That has certainly been my experience.
However, what about putting aside the bitching and getting on with the discussion? There is plenty of material in the articles and in the comments from others.
LikeLike
Be honest, Andy. In our past exchanges who has been the most rude. Who has resorted to vulgar obscenities and hatred. It has not come from my climate science supporting side but from your climate change denial side, hasn’t it?
Should I post a few links so people can get an idea?
LikeLike
Should I post a few links so people can get an idea?/em>
That;’s a great idea Ken. Then your readers will know how much contempt and undiluted hatred I have for you.
Please link my profanities and vulgarities from my “climate denial side”
As you know, I put you in the same category as the Lysenkoists and the Eugenicists. I would be delighted for you to highlight my thoughts.
LikeLike
Yes, Steve. I do realize that. It’s the $10,000 check that my small community writes to Mosaic every year that bothers me. If the Florida Sierra Club is successful, the strip mining will hopefully not expand much further South. Here in Maine, a lot of people care about supporting local food and local businesses, and many object to supporting companies with poor environmental records. There is also a concern about dangerous chemicals and freight trains with poor safety records. The HFSA is bid out each year to the lowest bidder and there have been problems with availability in the past. Some Maine utilities purchase the product from China, and many of us are uncomfortable with that.
LikeLike
Alison, environmental concerns as related to strip mining are a whole different issue. Your concerns with that, valid though they may be, are not reason to deprive a population the benefits of a public health initiative such as water fluoridation. As far as obtaining HFA From China or anywhere else, the only thing with which you need be concerned is that which comes out of your tap. The EPA mandates that all water additives meet the stringent National Sanitary Foundation Standard 60 certification requirements. Standard 60 begins at the tap, and mandates that no contaminant exceed 10% of the EPA maximum level of safety (MCL) for that contaminant. Fluoridated water meets these requirements with plenty of room to spare. It makes no difference where the HFA or any other additive originates. The water from the tap must meet Standard 60 cert. requirements or it is not permitted by the EPA.
Steven D. Slott, DDS
LikeLike
Ferguson van Reesema, you comments are either too aggressive or far too lengthy and really not related directly to the current discussion. I won’t approve these ones but you are welcome to contribute comments more related to the current debate and not as aggressive.
By the way this is not a debate between a scientist and a doctor. both Paul and I are retired research chemists with similar qualifications (PhDs). You are welcome to your own beliefs about the relevance of our backgrounds.
LikeLike
Ferguson. You exhibit a prime example of a small bit of irrelevant information being erroneously attempted to be applied to a scientific issue. Pay attention to this debate. You might actually learn something.
Steven D. Slott, DDS
LikeLike
There is a lot to be said. Fluoride is a lethal poison. I have documented something that will change the face of MOSAIC and Florida. I messaged the PDF onto The Facebook pg: Making Sense of Fluoride Hope to hear back from someone who is interested to know more.
LikeLike
Gina – you are quite wrong. Demonstratably so. F is not toxic at the optimum concentrations used in community water fluoridation. It is not lethal as you claim. If it were many millions of people would have died.
LikeLike