
This is Ken Perrott’s response to Paul Connett’s article Fluoride debate Part 1a – response: Connett
I think Paul’s response illustrates some of the problems in discussions of the fluoridation issue. He shows a selective approach to data, indulges in unwarranted extrapolation from research and misinterprets scientific knowledge to fit his own agenda. In the interests of maintaining interest by avoiding repetition, I will just select a few of the more obvious examples in my response.
It is pointless to continue debating definitions of fluoride as a medicine – as I have said the argument is largely semantic. people who wish to pursue the argument should do so in a court of law.
Irish oral health data.
Paul dismisses the data I presented showing the difference between fluoridated and unfluoridated areas in Ireland because he “would not exclude the researcher’s bias influencing the result!” That is an incredible statement because the source of the Irish data in my plot was exactly the same as that used in the plot of Cheng et al (2007) which Paul and many other campaigners against fluoridation constantly use to argue that fluoride does not contribute to the observed improvement of dental health!
In the figure below I have added the data for Ireland from Cheng et al’s diagram to illustrate this. Cheng et al used the mean WHO values for Ireland (the dotted line), (and only two data points for each country) while I simply used the data for both people from fluoridated and unfluoridated areas.
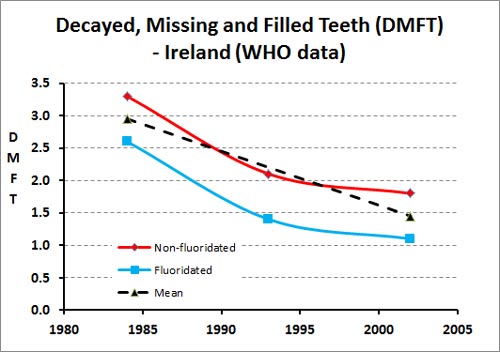
I am not impressed by Paul’s contradictory attitudes to the same data set. It displays a biased attitude driven by his wish to conclude that fluoridation has not had a beneficial effect on oral health.
I am also amazed that Paul should argue that with the Irish data it “would have been more impressive and more appropriate to have compared the health status of” the Republic of Ireland and Northern Ireland.
Surely comparison of the data from unfluoridated and fluoridated areas within a country introduces far fewer confounding factors than comparison of data for separate countries. History, culture, ethnic differences, differences in dental practice and assessments, and many other factors would contribute.
Paul shows some awareness of the problem of confounding factors when he refers to the noise in a large data set specifically in referring to Cheng et al’s original plots. Yet he seems to want to increase this noise, the influence of confounding factors, in the case of Ireland and rejects an example where confounding factors have been reduced. He then implies that it is the researchers who are “biased!”
The idea that somehow inter-country comparisons should have less noise than comparisons made within a country seems so obviously wrong to me I was pleased to find I am not the only person who sees this problem. Robyn Whyman in his report “Does delayed tooth eruption negate the effect of water fluoridation?“ puts it well:
“Studies that appropriately compare the effectiveness of water fluoridation do not compare poorly controlled inter-country population samples. They generally compare age, sex, and where possible ethnicity matched groups from similar areas. Inter-country comparisons of health status, including oral health status, are notoriously difficult to interpret for cause and effect, because there are so many environmental, social and contextual differences that need to be considered.”
Contamination of fluorosilicic acid
Here Paul handed over to William Hirzy who rejected the data I presented for Hamilton city, NZ, as atypical – because the arsenic (As) concentration was so low.
See my article Anti-fluoridation study flawed – petition rejected for some background to Hirzy, his paper and the petition he organised. One of our commentors, Steve Slott, has brought to my attention that Hirzy is a “long time avowed antifluoridationist and is employed by Connett as the paid lobbyist for Connett’s antifluoridationist group, FAN.”
In the table below I include data from 2 other certificates of analysis – in these cases Australian produced material. I also include my own data from a batch I analysed about 10 years ago when I was researching the chemical. This suggests the Hamilton sample is not that atypical, for our region anyway.
Concentrations (ppm) of contaminants in several different batches of fluorosilicic acid
| Toxic Element | Impurity limits* |
Hamilton City** | Incitec 08 | Incitec 09 | Own Anal |
| Sb | 40 | <0.09 | <2 | <2 | |
| As | 132 | 0.4 | 2.2 | <2 | 2 |
| Cd | 40 | 0.11 | <2 | <1 | <1 |
| Cr | 660 | 0.8 | <2 | <2 | 5 |
| Hg | 26 | <0.05 | <1 | <0.1 | |
| Ni | 264 | <1 | <2 | <1 | |
| Pb | 132 | 0.8 | <2 | <2 | 0.3 |
As you can see all the samples have a very low As concentration. Much lower than required by regulations for such materials used in water treatment. These samples do have a lot less As contamination than the ones Hirzy used in his study (typical value of 30 ppm). Maybe this represents the choice of samples in both cases, or maybe there are more sources of fluorosilicic acid in the US and some products have higher contamination of As. The fact that there are fewer plants producing fluorosilicic acid in New Zealand and Australia could be a reason for the apparently higher quality here.
I have no way of assessing the range of As contamination in US sourced samples so don’t know how representative Hirzy’s choices are. The NSF analyses water treatment chemicals and state in their last Fact Sheet on Fluoridation Products (2013) that only 43% of the fluoridation chemicals would have produced a detectable amount of As in the finished water (actually, because of the standard methods required – detectable in water at 10 times its maximum use level). The bar graph below shows the amounts of As measured in surveyed samples as a percentage of the USEPA regulated maximum contaminant level (MCL).
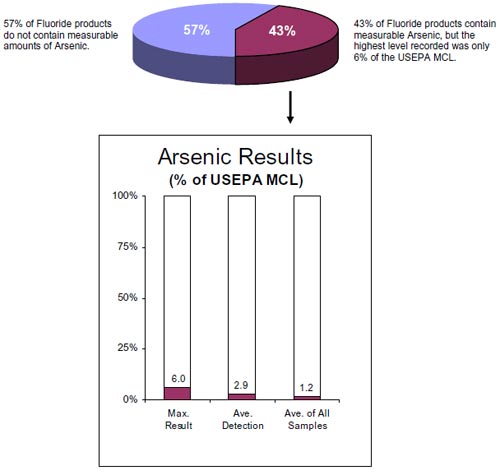
Similarly, Brown et al. (2004) (Trace contaminants in water treatment chemicals: sources and fate, American Water Works Association Journal. 96: 12, 111-125) identified the coagulation chemicals used in water treatment as far more likely to introduce contaminants than the fluoridation chemicals.
Hirzy may object because the NSF measured contaminants in terms of the finished water concentrations and not that in the concentrated chemicals. The finished water concentrations were then compared to the regulated MCL. But that will simply reflect his objection to the current MCL values.
This raises an interesting issue and identifies a problem with Hirzy’s approach in his campaign to substitute pharmaceutical grade NaF for fluorosilicic acid in water treatment. If the real issue for Hirzy was the As concentration he should instead have campaigned to lower the currently accepted regulations for level of contamination in fluoridation chemicals. Surely that would have satisfied his concern about the role of As in cancers – and possibly been more acceptable to authorities. If the current approved levels are too high let’s get them lowered – whatever chemical is used.
It is also interesting that the fluorosilicic acid used in Hamilton contained As contamination similar to those of the pharmaceutical grade NaF Hirzy used (typical value 0.76 ppm). He should be happy to advocate the use of material with our levels of purity in the US if his only concern is the As levels.
Perhaps we should be selling our fluorosilicic acid to the US if they cannot produce material to such standards.
Hirzy’s bandwagon is the possibility of cancers resulting from As in fluoridation chemicals. I appreciate where he is coming from and have no wish to debate that issue – it is outside my area of expertise. I can only comment that in our own situation (Hamilton City, NZ) the Waikato River source water has about 3 times the recommended maximum concentration of As for human consumption (see Hamilton – the water is the problem, not the fluoride!). This is reduced by about 80% during treatment but still remains a bigger source of As contamination than the fluoridation chemicals – by several orders of magnitude. it would be very silly to be concerned with contamination of the fluoridation chemicals and ignore the natural contamination of the source water.
Hirzy’s political activism
Finally Hirzy’s activist bias concerns me in that it could interfere with proper assessment of the risks. It certainly makes it difficult not to be suspicious about his claims. Out of hand he rejects the NSF conclusions as “a meaningless attempt at reassuring the public.” He also similarly rejects the conclusions of the NZ Water and Wastes Association as being “without merit.” This is derogatory to honest and active scientific and technical workers who have made the analyses, assessed the risks and drawn conclusions. Question the regulations if you must (and no regulations are permanent) but please do that using evidence, not by “poisoning the well” with such claims. Play the ball, not the man. Hirzy would object to his own work being flippantly rejected in such a way.
His use of the silly conspiracy theory that fluoridation is a way of disposing of industrial waste also raises questions of his credibility. And he is biased to claim that regulations have no “real value” because they were violated by one treatment plant!
Normal role of F in bioapatites
Paul seems to reject the concept that F is a normal constituent of apatites, including bioapatites. He argues that it is possible to have bones and teeth without fluoride. and says “that at the same level that fluorides interact with bioapatites it damages those bioapatites.”
But in the real, natural world, and not the extreme conditions of the laboratory, absolutely “pure” minerals don’t exist. Isomorphous substitution is normal and ubiquitous. Apatites only exist as end members like hydroxyapatite in unusual or laboratory situations. Fluoride and carbonate are very commonly incorporated into bioapatite by isomorphous substitution – as are some common cations.
In reality no bones or teeth are “fluoride free.” Which is just as well because they would have higher solubility and reduced strength and hardness. Sure, this might mean that it is normal for a proportion of people to have teeth with “questionable” or “very mild” forms of fluorosis. But that is a cosmetic issue (if at all noticeable) and does no harm. It has probably been a simple fact about our teeth through our whole evolution.
For the vast majority of people who have dental fluorosis (recognised by a professional) it is usually classified as “questionable” or “mild.” Real health concerns should only be raised for severe dental fluorosis. Yet anti-fluoride activists lump all those grades together and pretend that dental fluorosis is a much bigger problem than it really is.
“Topical” mechanism
We will deal with the mechanism of the beneficial role of fluoride on teeth in later articles so I will just respond briefly to Paul’s brief reference to the issue in his last article here. He claims the US Centers for Disease Control and Prevention (CDC) agrees “that the predominant benefit as far as protecting teeth is concerned is topical (rather than systemic).” (Actually, he says “concedes” and not “agrees” but this word is ideologically loaded). That is correct as far as it goes but we should remember that this is referring to existing teeth – ingested fluoride still has a beneficial role with bones and pre-erupted teeth. The word “predominant” is important. So I can’t help recognise the bait and switch tactic when, in his book, he drops the word “predominant” in his chapter summary and he says:
“For many years, fluoride was believed to act systemically to prevent caries— tooth decay—by being incorporated into the enamel of the developing teeth. However, it is now known to act topically—that is, at the surface of the tooth. Thus, the main reason for ingesting fluoride has disappeared . . .”
Again and again I find anti-fluoride people using this tactic to deny any mechanism but “topical.” They thereby purposely deny any of the known beneficial effects of ingested fluoride.
This bait and switch tactic is compounded by another bait and switch where the “topical” – referring to the reactions occurring at the tooth surface because of fluoride in saliva and biofilms – becomes a new “topical” – referring only to methods of application such as toothpaste and dentrifices. This tactic enables them to deny the beneficial roles of fluoride transferred from water to saliva during drinking, as well as that ingested.
Anti-fluoride activists pushed this misrepresentation hard during recent hearings on fluoridation at the Hamilton City Council in NZ. It had its effect when the Council took on itself to issue a leaflet giving oral health advice. This repeated the “topical” misinformation. Health and dental experts were publicly very critical of the leaflet and Hamiltonians felt embarrassed by the Council’s hubris.
Fluoridated toothpaste only complements, does not substitute for, this regular “top up” of saliva F during drinking and eating.
Perhaps we should be referring to “surface” mechanisms rather than “topical” ones as the latter is so easily seen as applying only to application methods.
Extrapolation from high concentration animal studies
I think Paul’s confidence in unsupported extrapolation from higher concentration animal studies is very cavalier. Paul claims:
“in the case of fluoride it is well know. That you have to give 5 to 10 times as much fluoride to rats to reach the same plasma level as you need in humans.”
He doesn’t support this with a citation – but I suspect that would only be to a similar assertion in Fluoride Alert or a sister web site, with no, or poor, literature reference.
The US National Research Council report “Fluoride in Drinking Water – A Scientific Review of EPA’s Standards“ discussed the contradictory data used for attempting to show a ratio between humans and rats for blood plasma levels and concluded:
“Dunipace et al. (1995) concluded that rats require about five times greater water concentrations than humans to reach the same plasma concentration. That factor appears uncertain, in part because the ratio can change with age or length of exposure. In addition, this approach compares water concentrations, not dose. Plasma levels can also vary considerably both between people and in the same person over time (Ekstrand 1978).”
I am suspicious of attempts to use comparison of blood plasma F levels for such justifications because of the huge range and variability of these levels. This sort of speculation seems to fuel the frequent use of the word “might” in Paul’s article (and attempts to convert such logical possibilities to realities) and in the end leads to the speculation being present as a fact (Paul’s “well-known” and the simple FANNZ declaration).
But Paul at least refers to one study on rats using drinking water with F concentrations closer to those of fluoridated water – Varner et al (1998). Unfortunately I could not get the full text of this paper and the link Paul provides to http://www.fluoride-journal.com does not allow access to mere mortals like me. In my search I was amazed how links promising full text of papers like this often just take one back to Fluoride Alert and their in-house interpretation.
The abstract mentions changes in cerebrovascular and neuronal integrity for AlF3, and to a smaller extent for NaF. As I can’t access the discussion to understand he possible significance of these small changes I won’t comment further on this.
Why do countries not fluoridate
Paul describes my consideration of the various reasons behind the decisions of countries not to fluoridate their community water supplies as “more like self-serving political spin than reality!” That is rather harsh – considering he then goes on to claim only 2 main reasons – freedom of choice and health concerns. Using his own article as a reference!
No, I won’t respond by selecting personal statement from citizens of the non-fluoridated countries as he asks. But here is an outline of the situation with fluoridation throughout the world taken from a recent issue of the newsletter of the New Zealand National Fluoride Information Service. It gives a pretty detailed picture:
Countries with widespread water fluoridation programmes include Australia, the United States of America, Canada, the United Kingdom, Ireland, Spain, Israel, Brazil, Brunei, Chile, Argentina, Colombia, Hong Kong, South Korea, Singapore and Malaysia. Countries with limited water fluoridation programmes include Vietnam, Fiji, Papua New Guinea, and South Korea.
Several countries are unable to introduce water fluoridation programmes due to technical, financial or sociocultural reasons. As an alternative, both salt and milk have been found to be reliable and convenient vehicles for increasing fluoride intake to an optimal level for hard to reach and low socio-economic communities. Studies have found them to be as effective as community water fluoridation schemes.
Some European, Latin American, and Caribbean countries, including France, Switzerland, Germany, Costa rica, Colombia and Jamaica currently use fluoridated salt schemes. Mexico and most Latin American and Caribbean countries (apart from Argentina, Brazil, Chile and French Guyana) have or have had salt fluoridation programmes.
A smaller number of countries currently have fluoridated milk programmes, including Bulgaria, Chile, China, Peru, Russia, Thailand and the United Kingdom
Some country regions have optimal amounts of naturally occurring fluoride which provides good protection for oral health. examples of countries supplied with naturally fluoridated water at or around the optimum level needed to prevent dental decay include the United Kingdom (estimated 329,000 people), United States of America (estimated 10,078,000 people) Canada (estimated 300,000 people) and Australia (estimated 144,000 people).
It is estimated that 39.5 million people around the world have access to naturally fluoridated water at the optimal level although variations from one community to another over time make it difficult to calculate an accurate total.
Reasons for not fluoridating water supplies and/or using alternative ways of overcoming fluoride deficiencies are simply not restricted to attitudes towards freedom of choice and health concerns, although they may have been deciding factors for a few countries. This is another instance where opponents of fluoridation are making widespread simplistic claims (like Europe bans use of fluorosilicic acid) based on only a few facts, and ignoring (or hiding) the details.
We should also remember that despite different decisions by governments and local authorities about implementation of fluoridation all the reputable national and international health bodies do accept the scientific consensus of the beneficial role of fluoride in oral health. It is this endorsement which is more relevant to us than the specific technical, political or social decisions made in other countries.
Political activism
I am glad Paul rejects extremism among anti-fluoride activists. However this does not seem to stop him cooperating with extreme conspiracy theorists like Alex Jones and Vinny Eastwood to produce videos. (Have a look at Cyber bullying of science, which includes a recent video of Eastwood’s attacking scientists and science, to get an idea of how silly these people can be). People do notice such associations and draw their own conclusions. Paul appears to give some justification of “the more nutty conspiracy theories espoused by some opponents of fluoridation.” He says “promoters of fluoridation should not be surprised that some people are trying to come up with a rational explanation for why certain governments are behaving so irrationally promoting this practice.” Well that is his perspective and it is a minority one. I certainly don’t accept such justifications because I, and many others, have no trouble understanding the decisions to fluoridate.
Misrepresentation of the facts is a real problem among activists of all persuasions. That is understandable because ideological and political convictions and motivations can distract even the most honest people. Paul presents an example of an image that illustrates this for some supporters of fluoridation.
This image seemed to create a lot of controversy among local Facebook pages and I got the blame because it was posted on this blog. I have been assuring complainants that it is not my image and I do not support its implied message. It seems to have been taken from a document prepared under the Queensland Health logo. I cannot find a source and no-one seems to be able to give a citation. It is not on the Queensland Health web site. All Internet references seem to be in documents and sites of fluoridation opponents – indicating that it has backfired as a propaganda exercise for fluoridation. I gather it may have been prepared to send to selected Australian members of parliament at some stage.
Paul has sent me a copy of the document which interested readers can download.
But here is the trouble for those living in glasshouses who wish to throw stones. This sort of misrepresentation is probably more common among opponents of fluoridation. The figure below, for example, is from a document of the “Queenslanders for Safe Water” website which ironically included and criticised the Queensland Health photos! (Thanks to commenter Steve Slott for the link). It uses photos of extreme skeletal and dental fluorosis to argue against fluoridation.
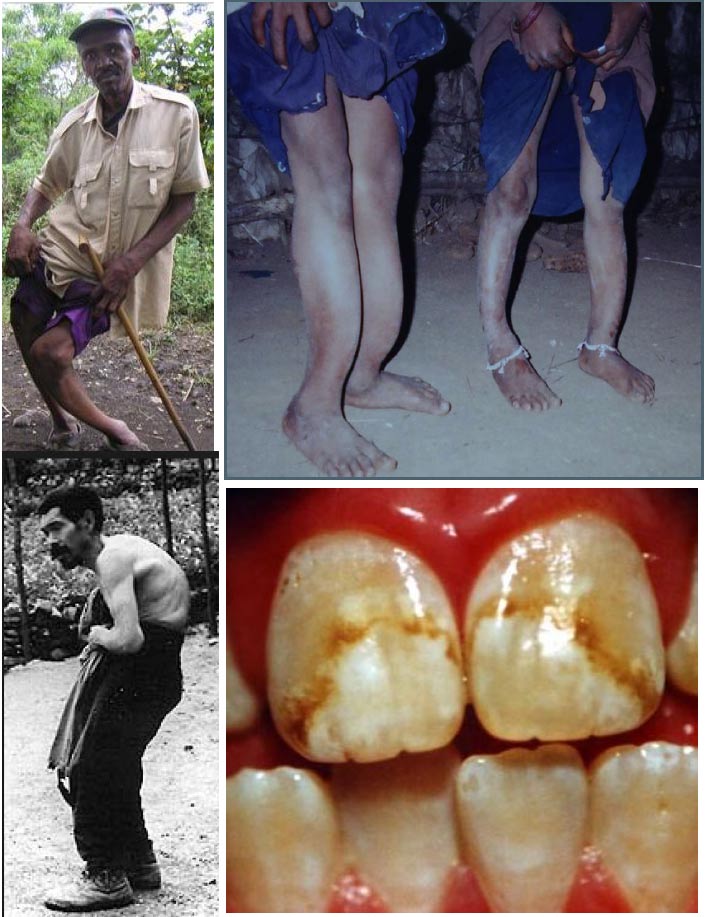
This, and the Queensland Health photos, are extreme exaggerations used to promote a message. Reasonable people should condemn that tactic. But isn’t this, in essence, the same tactic used by Paul and other opponents of fluoridation when they extrapolate from animal studies at high concentrations, characterise the relatively common very mild and “questionable” cosmetic fluorosis as if it were severe, use the “topical” mechanism to argue that fluoridated water has no influence, wildly exaggerate the concentration of toxic contaminants in fluoridation chemicals, persistently and inappropriately describes fluoride a poison and a neurotoxin, misrepresent the reasons why some countries do not fluoridate their water supplies and deny data illustrating a beneficial effect of fluoride on oral health as “biased?”
Anyone wanting to follow the debate and/or check back over previous articles in the debate can find the list of articles at Fluoride Debate.
See also:
Similar articles on fluoridation
Making sense of fluoride Facebook page








I’m glad you didn’t dignify with a reply the nonsensical evolutionary case for non fluoridation as put forward by Connett.
LikeLike
With fluoridation you can’t control the dose,don’t know intake from other sources and it’s difficult to monitor for individual sensitivities. I find Mr Perrott’s arguments on the weak side,defensive and pedantic while Mr Connett’s arguments are well reasoned and sensible. I think the major hurdle for the supporters of fluoridation is that they can never explain why it has to go into the public water supply so that everybody who partakes of it is subject to it, many against their will.
LikeLike
If delayed eruption was causing an apparent decrease in caries that effect would decrease with time as the delay time becomes a progressively smaller portion of the tooth’s life.
The Brunelle and Carlos data shows the opposite. A graph made from those data by Dr. Howard Pollick was published as part of a prior “debate” between Paul Connett and Pollick.
Dr. Pollick’s graph may be seen here:
http://photos.oregonlive.com/photogallery/2013/05/fluoridation_prevents_more_cav.html
Further a very large study was done in the 60’s which found no difference in eruption associated with drinking fluoridated water:
http://jdr.sagepub.com/cgi/reprint/44/3/509
James P. Carlos and Alan M. Gittelsohn
Longitudinal Studies of the Natural History of Caries. I. Eruption Patterns of
the Permanent Teeth
Journal of Dental Research 1965 44: 509-516
At the time data collection ended in 1960, fluoridation of the water supply in Newburgh had been in progress for 15 years.
Summary
The average age and sequence of eruption of each of the permanent teeth was determined by analysis of serial observations of 16,000 children in Newburgh and Kingston, New York, preliminary to further longitudinal studies of dental-caries incidence. From the volume and type of data on which these estimates are based, it is felt that they represent the most reliable description of eruption chronology yet available.
In addition to the expected tendency for eruption to occur earlier in females, an interesting and consistent finding was a sex difference in eruption sequence. Comparisons of mean eruption times within several sub-groups confirmed that appearance of the lower cuspid preceded that of upper and lower first bicuspids in females, while the reverse was true in males.
Consumption of fluoridated water (1.2 ppm) for varying periods of time had no discernible influence on eruption times or sequence.
Dr. Connett’s political use of a hypothesized year’s difference in eruption is egregious. Dr. Hardy Limeback did the same when he spoke both publicly and to my hospital’s medical in 2005 while campaigning for an initiative to “ban” industrial waste byproducts from drinking water. I am unaware of any study ever done showing a full year’s difference in eruption due to fluoridation. This claim is a fabrication.
Charles C. Haynie, M.D.; FACS
Hood River, OR
LikeLike
There’s another logical fallacy or assumption that is promoted and that people fall for, because it is repeated so often. The fallacy is that fluoride is required for good teeth.That is incorrect. You can have perfectly good teeth without consuming fluoride. This is evidenced by many places in the world that have better teeth than NZ without fluoride. Insisting on fluoride is a bit like saying you have to smoke Camels to look cool. Dentists featured in cigarette ads. They also said mercury was safe. Fluoride is very toxic and will go the same way as tobacco and mercury.
LikeLike
Shane, did you not read the article? I replied specifically to that argument and you have ignored my comments completely.
That is rude of you. 🙂
>
LikeLike
Shane
With fluoridation you can’t control the dose,don’t know intake from other sources and it’s difficult to monitor for individual sensitivities.
1 Unarguably fluoride is not delivered or intended to be delivered as a dose or series of measured doses, ergo…
2 …it need not be controlled as a strict discrete dosages
3 The fluoride ion is being made available in the environment (water supply) to enable a surface chemical reaction with teeth enamel.
4 The parameter that needs to be ensured is that the concentration in the environment is at a safe level to avoid harmful consequences when the body uptakes the ion. Overwhelmingly, the scientific literature is clear that levels set by public health authorities is safe.
LikeLike
Richard you don’t understand the difference between concentration and dose. You can’t go on concentration alone, as people drink different amounts. This means there is no control of fluoride intake. The best surface chemical reaction with the teeth enamel is from fluoridated toothpaste. That is unequivocal. What’s also unequivocal is that fluoridation subjects all your internal organs, brain and cells to fluoride which is totally unnecessary. So if you want fluoride then use toothpaste – its the most effective.
LikeLike
You don’t need to control single or even multiple dosages when delivered in this manner. Dosage is irrelevant.
It is environmental exposure that is important, and uptake, both within safe limits.
(here let me type it again…)
exposure…uptake….
both within safe limits.
Hello…?
Health authorities are not intellectually challenged.
They know water supply may not be the only source of exposure to fluoride.
Science has done the work, public health authorities have analysed the results and determined safe limits.
So where are the countless law suits against the evil health authorities for poisoning people?
Are you campaigning against iodised table salt on the same spurious grounds? If not why not?
LikeLike
“This is evidenced by many places in the world that have better teeth than NZ without fluoride.” Citations, please. And these ‘many places’ should be places that are not receiving it via milk, salt, or naturally fluoridated water.
LikeLike
Shane – “unequivocal” defines a high level of certainty. Are you using that word wisely? Have you any evidence to support your claims. Remember if you can’t supply any support you are exposed as being dishonest.
Now could you provide the support for your statement that “the best surface chemical reaction with teeth enamel is from fluoridated toothpaste” – consider the frequency of application in your answer.
And please provide support for the significance of your claim that “fluridation subject also all your internal organis, brain and cells to fluoride” – why is this any more significant that subjecting these organs, etc., to water?
>
LikeLike
Shane
In regard to your question about “dose” versus “concentration” that is a frequently used tactic of fluoridation opponents to induce undue fear where none is warranted. Simply put, water is fluoridated at 0.7 mg/liter (ppm=mg/liter). Thus, for every liter of fluoridated water consumed, the “dose” of fluoride intake is 0.7 mg. The average daily water consumption by an adult is 2-3 liters per day. So, let’s go to an extreme and double that to an excessive 6 liters of fluoridated water consumption per day. This translates to 4.2 mg “dose” of fluoride intake per day from the water. The CDC estimates that of the total daily intake, or “dose”, of fluoride from all sources including dental products, 75% is from the water. Thus as 4.2 mg is 75% if the total daily intake from all sources, the total daily intake, or “dose” from all sources would be 5.6 mg for an individual who consumed an excessive 6 liters of fluoridated water per day.
The Institute of Medicine has established that the daily upper limit for fluoride intake from all sources, for adults, before adverse effects will occur, short or long term, is 10 mg. Thus, even the excessive 6 liter per day consumer of water will still only take in a daily “dose” of fluoride that is slightly more than half the upper limit before adverse effects.
The range of safety between the miniscule few parts per million fluoride that are added to existing fluoride levels in your water, is so wide that “dose” is not an issue. Before the UL of 10 mg could be reached, water toxicity would be the concern, not fluoride.
Click to access ULs%20for%20Vitamins%20and%20Elements.pdf
Steven D. Slott, DDS
LikeLike
When all the debate over science and safety is through, it will boil down to one thing.
You can believe that public health authorities worldwide are right or they are wrong.
If wrong, then you have to establish a case that they are
1 incompetent. – All of them. No exceptions.
2 mendacious – all of them – which implies conspiracy.
LikeLike
Agreed, Richard. It constantly amazes me that antifluoridationists assume that the worldwide community of respected science and healthcare experts have totally overlooked issues such as “dose”, total intake, safety maximums, and other such elementary concerns that only they, the “informed” antifluoridationists, understand.
Steven D. Slott, DDS
LikeLike
Shane
With due deference to your expert” opinion on the “most effective” means of providing fluoride protection, the mode of action of water fluoridation is both systemic and topical. The percentage of each is irrelevant as the preventive benefit is derived from the consistent bathing of the teeth with a low concentration of fluoride all during the day. This comes directly from the consumption of fluoridated water, drinks made with fluoridated water, and foods prepared with fluoridated water…..and systemically from incorporation of fluoride into the saliva.
From the CDC:
“Both drinking water and toothpaste provide important and complementary benefits. The drinking water provides long low-level protection, but the fluoride in toothpaste is at a high enough concentration that it has additional properties. Whether in water or toothpaste, fluoride works in two main ways: by slowing the activity of bacteria that cause decay, and by combining with the enamel on the surface of the teeth to make it stronger and more resistant to decay. Fluoride in the water, although at a lower concentration than in toothpaste, maintains a constant low level of fluoride in the dental plaque and saliva all day. Toothpaste provides a high level of fluoride, but only for 1-2 hours after brushing, so the water exposure during the remainder of the day takes over after that.”
——http://www.cdc.gov/fluoridation/fact_sheets/cwf_qa.htm#3
Steven D. Slott, DDS
LikeLike
Ken
I do have the full text of Varner’s study, although I’m not sure how to get it to you if you really want it. I’ll look at it again, but as I remember, it has little pertinence to water fluoridated at 0.7 ppm.
Steven D. Slott, DDS
LikeLike
My toothpaste says “12 hour protection”.
LikeLike
Outstanding response, Ken. Once again, thank you for doing this.
Steven D. Slott, DDS
LikeLike
Shane
The relevance of marketing claims made by toothpaste manufacturers? Is this your idea of the “science” that supports fluoridation opposition? If so, you’re right in line with the thinking of most other antifluoridationists.
Steven D. Slott, DDS
LikeLike
(Just reminding Steve that Alison’s polite question remains unaddressed https://openparachute.wordpress.com/2013/11/07/fluoride-debate-part-1a-response-to-connets-response-perrott/#comment-46850 ).
LikeLike
Oops, previous comment was for Shane, not Steve, sorry about that.
LikeLike
Ken, You can argue that fluoridation is a not a medication but you cannot truthfully deny that fluoridation is implemented to treat people for the condition of tooth decay; thus fluoridation is a medical treatment.
Except in extreme cases, people with ‘capacity’ have the right to determine for themselves whether or not they accept or reject a treatment. Any medical practitioner worth his/her salt knows that ‘informed consent’ means ‘informed consent to medical treatment’.
Partly due to court cases and the evolution of medicine, people with ‘capacity’ are now legally entitled to determine the very serious matter of whether or not their own life support should be switched off in certain circumstances; such as in the recent case of the mentally-able quadriplegic, Timothy Bowers, who was woken from his coma following a hunting accident in Indiana, so he could determine for himself whether or not he wished to have his life-support system switched off.
Timothy legally chose death over life so his life-support was withdrawn and he died about five hours later.
Please explain your rationale for thinking that you and your ilk have a God-given right to override individuals with the ‘capacity’ to make informed rational decisions to determine their own medical treatments – in this instance, relating to being treated with industrial-waste, called fluoride, via public water supplies.
LikeLike
Steve, In India, 0.7 to 1.7 ppm/fluoride has been found to produce a significant amount of skeletal fluorosis in the population.
LikeLike
Blossom – please present evidence for your claim of skeletal fluorosis in India at 0.7 ppm F in drinking water. A reference or citation/link. Otherwise I will have to assume you are telling porkies.
LikeLike
Blossom, I do not argue that. In fact I point out that we finished with that debate in the previous exchange.
It boils down to the old bait and switch trick – define medicine loosely so ohat it captures F (and just about everything else). Then change your definition if medicine to that of a powerful drug which requires accurate controlled doses and informed consent.
I am not going to debate that fallacy any further. If you want to then I suggest you take it to a court of law where people have the interest and experience of sorting out such dishonest muddles.
We have put that one to bed here, blossom.
LikeLike
Blossom, your video does not relate to this exchange and I have therefore moderated it. There is a lot of interest in discussing the issue raised in the exchange between me and Connett and I do not want to see space wasted by trolls posting propaganda videos. Please ensure your comments are relevant to the articles.
LikeLike
No, blossom! you are spamming. I have put you under permanent moderation so that I can control that behaviour.
Post something sensible and it will get through. The rest won’t.
LikeLike
Can somebody please explain why the fluoride has to be added to the public water supply so that 99 % goes down the drain. Why can’t people just add it to their water at home. Why upset an enormous amount of people by adding it to the public water supply. More than that, then attack those people who don’t want added fluoride. Let’s have a little respect for people who don’t want extra fluoride.
LikeLike
Can somebody please explain why the fluoride has to be added to the public water supply so that 99 % goes down the drain.
It’s not like fluoride is in short supply. It’s a bit silly, don’t you think?
Behold…
“Can somebody please explain why the chlorine has to be added to the public water supply so that 99 % goes down the drain.”
Why upset an enormous amount of people by adding it to the public water supply.
Enormous? Are you sure you know the meaning of the word?
Besides, science is not a popularity poll.
More than that, then attack those people who don’t want added fluoride.
Ah, so now “those people” are being “attacked”. Sounds terrible.
And just a tad untrue.
Let’s have a little respect for people who don’t want extra fluoride.
Respect is earned. Stupidity and the global scientific conspiracy theories get laughed at, and rightly so.
THE FLUORIDE CONSPIRACY IN A NUTSHELL
LikeLike
Shane –
For someone who is so “anti”- fluoride you seem concerned that 99% “goes down the drain” – why does this bother you?
“Why can’t people just add it to their water at home.”:
Because this is a public health issue, not a private health issue; many people, including children and lower socio economic groups would not gain the benefit if this was the case.
“Why upset an enormous amount of people by adding it to the public water supply”.
Firstly, you are vastly over estimating the number of people who would be upset, just look at the latest referenda in the North Island. Secondly, I would rather a few people be upset if this improved the dental health and weall being of a significant part of our community.
“More than that, then attack those people who don’t want added fluoride”.
As I see it people aren’t getting attacked here, just what they say. If you don’t like robust debate then you are probably in the wrong forum.
Lastly…respect…mmm….what to say here….if you want respect then simply put forward some cogent, substantiated arguments rather than cry foul when you “think” you are personally being hard done by
LikeLike
Ken, At the Hamilton Tribunal the DHB agreed that there is NO benefit to the pre-erupted teeth. Why have you not watched the Tribunal since it is on Youtube? You have also been given on many occasions this link http://www.marketground.co.nz/fannz/98952/1 which is the transcript (as well as video footage) of Robin Whyman admitting that fluoride does not benefit from being incorporated into the tooth.
It is also ridiculous that you try to make out that Northern Ireland may have cultural, historical etc differences than the Republic of Ireland. The Republic of Ireland was only separated from Northern Ireland less than 100 years ago. They are basically the same people and they will have just about exactly the same culture, genetics and diet.
Alison – you have been told many times that there are plenty of other countries that have the same rate, or less of decay than NZ http://fluoridealert.org/content/oecd_nations/ Only 4 countries in Europe have SOME fluoridated salt and most of the water in the other European countries is low in fluoride. This is why they were all encouraged to add fluoride chemicals but they rejected it. Seems you guys keep pretending not to know the truth.
Also, Ken, looks like you have lost the argument and now you have resorted to character assassination because you don’t know what else to say.
LikeLike
Rather put 100 % down the drain – oh sorry that is illegal but its OK to put in our water lol. Christopher and Cedric are attacking me – confirms what I said. The words nutter and tin foil hat have been used countless times in the media. You guys are like a Fluoride Police Force trying to force fluoridation. Come on guys – get your own fluoride if you want it so badly. Many low socio -economic people also don’t want fluoride so that argument doesn’t stack up any more. Rather fluoridate salt so people can choose. The NFIS discusses salt as an alternative.
LikeLike
Why can’t people just add it to their water at home. Why upset an enormous amount of people by adding it to the public water supply.
You won’t get any attack from me with this line of argument. I acknowledge that it is a political issue. It should rightly be debated as such – but without resort to the distortion of the scientific research that too often goes on.
The problem for those against fluoridation is that they struggle to make a case that fluoridation is harmful without resorting to distortion and untruths.
LikeLike
I agree with Mary. Ken seems to have lost the argument and is resorting to playing the man. Also the 12,000 people who voted against fluoride in Hamilton is not a “few”.
LikeLike
Mary, links to original sources of papers/studies please. Advocacy websites will just be ignored around here.
LikeLike
Nutter and tin foil hat
Are you trying to construct an argument Shane?
Think this debate is getting hijacked. Thought this was about the science?
LikeLike
Shane- “Many low socio -economic people also don’t want fluoride so that argument doesn’t stack up any more”
Do you have any data/citations to back this up?
LikeLike
Robin Whyman admitting that fluoride does not benefit from being incorporated into the tooth.
Yes, there is no benefit at all for the fluoride. Nobody will argue with that.
But ability of tooth enamel to resist decay is increased by exposure to fluoride.
LikeLike
Christopher and Cedric are attacking me – confirms what I said.
“Attacking”?
You keep using that word. I do not think it means what you think it means.
LikeLike
Mary’s comment is actually quite comical. First, she talks of how “fluoride does not benefit from being incorporated into the tooth”. Well, we’re really concerned with how humans benefit from water fluoridation, not about how benefits accrue to fluoride. But, okay, her confusing language aside, it can probably be assumed that what she means is that Whyman “admits” that there is no systemic benefit to fluoride. Then she provides a cite to the biased, antifluoridationist website of FANNZ where is located a “transcript” of Robin Whyman which is interspersed with FANNZ editorial comments, and FANNZ highlighting of portions of the “transcript. Weeding through the FANNZ editorializing, misspellings, and highlights, I see no such “admission” by Whyman. What the provided FANNZ version of the transcript states is:
“Do we have any common ground between the people who are proponent and people saying we shouldn’t have community water fluoridation – we are agreeing that it this is a topical effect, this is largely occurring by a topical benefit. So the question becomes why drink it if it becomes a surface effect?”
“largely occurring by a topical effect” does not translate to mean that it is NOT occurring at all by systemic effect.
Mary then moves on to assert her opinion that cultures that have been separate for nearly 100 years will still have the same “culture, genetics, and diet”.
She closes all of this with a cite to another biased, antifluoridationist website, “fluoridealert.org” supposedly as “support” for her opinion of what constitutes the “truth” about fluoridation practices of different countries.
Comical.
Steven D. Slott, DDS
LikeLike
That swallowed fluoride is unimportant in preventing cavities, as James Reeves believes, is a mistaken concept
New research shows both the swallowed fluoride incorporated into adult teeth structure as well as fluoride at the tooth surface to be important:
Children who drink fluoridated water become adults with more teeth.
see: http://www.sciencedaily.com/releases/2010/08/100826212037.htm
and the minimal degrees of enamel fluorosis associated with fluoridation protect those teeth from cavities. This proof positive of a systemic effect.
see: The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren. Hiroko Iida, Jayanth V. Kumar. JADA July 1, 2009 140(7): 855-862
http://www.ncbi.nlm.nih.gov/pubmed/19571049
An elegantly designed study from Australia showed that i the best cavity protection for school children’s adult teeth comes with drinking fluoridated water while teeth were forming and continuing to do so after the teeth erupt.
see:
Community Dent Oral Epidemiol. 2004 Dec;32(6):435-46. Relative effects of pre-and post-eruption water fluoride on caries experience by surface type of permanent first molars.
Singh KA, Spencer AJ. Australian Research Centre for Population Oral Health, Dental School, Faculty of Health Sciences, The University of Adelaide, Adelaide, Australia.
http://www.ncbi.nlm.nih.gov/pubmed/15541159
While it may be the case that the topical effect is more important in caries prevention, these and other data show that the systemic effect is also significant.
The underlying issue of this “debate” really is an easy decision . . optimized fluoride ions from community water fluoridation simply prevent cavities. The precise mechanism is not terribly important to this straightforward matter.
LikeLike
The socio-economic distribution of those who oppose is really not important in the debate about community water fluoridation (CWF).
It is simply a fact of public health science that individually based programs will be less effective and more expensive at changing disease rates.
A study in the US from Colorado showed very clearly that fluoridation is the most cost effective at decreasing preschool children with mouth fulls of cavities’ need for operations under anesthesia. If this were the only benefit, CWF would return 150% on the fluoridation investment.
see: http://www.ncbi.nlm.nih.gov/pubmed/22380939
Prev Chronic Dis. 2012 Mar;9:E66. A simulation model for designing effective interventions in early childhood caries. Hirsch GB, Edelstein BL, Frosh M, Anselmo T.
Courts in the US have ruled that CWF is not the act of forced (mass) medication because:
1. No one is forced to drink the tap water.
2. Fluoride is a natural ion generally present in drinking water at a less than optimal concentration
3. Water providers have a specific obligation to determine the nature of their product including its chemical content.
4. Fluoridated water is similar to enriched flour, iodinated salt, Vitamin D fortified milk etc.
A representative quote from the Ohio Supreme court is on point:
fluoridation is) “no more practicing medicine or dentistry or manufacturing, preparing, compounding or selling a drug, than a mother would be who furnishes her children a well-balanced diet.”
LikeLike
Mary, others have already replied to you on the pre-erupted teeth issue. My comments about you misrepresenting Robin Whyman still stand. I realise this is politically important to you as your misrepresentation of the issue is part of your organisation’s political platform.
Paul and I will probably be looking at the issue in more detail in the second round of our exchange – and I am sure the commenters here will also have more information to input then. They have proved to be a great resource.
You try to make an issue of differences between Northern and Southern Ireland. That is a diversion. Here is the issue. Paul referred to data from the WHO claiming it showed no influence of fluoride on the improvement in oral health. Leaving aside the impossibility of credibly drawing such a conclusion (I have discussed that elsewhere) the graphics he used included data from Ireland which were national – the data for the fluoridated and unfluoridated areas were averages.
My graphic simply plotted the fluoridated and unfluoridated data separately showing a clear difference resulting from fluoridation. Where Paul went wrong was to the imply the researcher were guilty of bias! For data he was quite prepared to support when averaged! It was the same data for Christ’s sake!
That is not credible scientific behaviour and I took him to task for it.
Paul was also disingenuous to “prefer” comparison between the two countries. He surely knows that whatever their common history this would introduce confounding factors and could therefore scientifically not be as acceptable as the in-country comparison WHO and I used.
Please Mary, stop trying to divert attention away from the real issues.
LikeLike
Wouldn’t it be potentially easier and more effective to fluoridate salt? I don’t know what it’s like in New Zealand, but in my state of the US (Maine), only 50% of people are on municipal water. This means that at best, fluoridated water reaches half the people (yes, I know that the halo effect plays a role too). Why not fluoridate salt instead and make it widely available. It could theoretically reach many moor people, and those who wanted to specifically avoid it would be able to buy specialty brands of non-fluoridated salt.
LikeLike
I agree salt fluoridation is an effective alternative. But the mere existence of another possibility is not a reason to repeal or cease water fluoridation. If salt were to be the method of deliver fluoride in the USA there would need be a nation decision. The FDA would need to specify and regulate a new fortified salt product. This might well prove difficult, reveal concerns which are not currently obvious and certainly would take years to implement.
If salt fluoridation were to replace community water fluoridation this should be done in a way which leaves no breaks in the public health benefits.
LikeLike
Would it be okay to start salt fluoridation even with water fluoridation, or would water fluoridation have to stop first?
LikeLike
If both ran concurrently then everyone would be getting twice the recommended exposure as a baseline.
Gawd, imagine the moaning that would arise then, doesn’t bear thinking about.
LikeLike
Can’t have both. the move from one to the other would be complicated. I don’t think it has ever been done. Again, the mere possibility that this could be done has little to do with the current debate.
LikeLike
I imagine salt fluoridation could be an alternative if the anti-fluoride argument was winning out. That is, if the country decided to stop water fluoridation the salt could become an alternative promoted by health authorities.
However, I can see a scenario where there would be campaigns against this. Just imagine if regular salt was fluoridated as well as iodised with a small alternative unfluoridated, uniodised salt?
I think activists may still oppose that. After all, the choice argument is very weak because it is actually quite easy for people to opt out of public water one way or another. Many already do. I think activists who really believe F is a poison would want to stop it completely.
In NZ the suggestion of adding folic acid to bread was actively opposed.
In the UK there have been campaigns against fluoridated milk in schools even though kids could be opted out.
Actually, fluoridated milk could be an option at least for schools in unfluoridated regions of countries.
>
LikeLike
I believe that should this be undertaken there would best be “regular” salt and “fortified” salt. I would oppose the consumer option of just iodine without the fluoride. It appears that internationally where fluoridated salt is commonly sold this is how it is done.
In the long run with physicians and dentists routinely recommending the fortified salt it is likely that the public’s acceptance would be the same as which iodinated salt currently enjoys. The truth would simply win out.
What can’t be allowed is the mere possibility of a fluoridated salt product “replacing” CWF to be used by opponents to defeat community water fluoridation as it is currently so effectively employed.
LikeLike
Haha Ken you are getting your butt whipped and appear to be a drowning rat in a sea of fluoridated facts. You are trying to turn a scientific debate into a jungian psychoanalysis of a movement you are too arrogant to analyse with any degree of subjectiveness
LikeLike
You seem upset, JDR?
Now what about stopping the abuse and contributing to the discussion. Comments like this will be moderated from now on.
LikeLike
You guys mustn’t be very intelligent if you couldn’t work out that I had a typo and the line “..Robin Whyman admitting that fluoride does not benefit from being incorporated into the tooth” was meant to be “Robin Whyman admitting that fluoride does NO benefit from being incorporated into the tooth.”. Ken certainly makes many typos in his commentaries so you can hardly denigrate me for accidentally saying “not” instead of “no”.
And this brings me back to the point I have made which you have conveniently ignored. Whyman said there was NO benefit from having fluoride incorporated into the tooth structure. Contrary to what Steve Sloth says there is only one comment from FANNZ in the transcript that is is clearly signed “ED” the rest of it is Whyman’s words verbatim. And we are not asking people to take our word for it. At the bottom is a link to the video of Whyman saying it.
So all of you fluoridationists are disagreeing with Whyman. He says that fluoride does NOT benefit teeth from the inside ONLY from the outside. As you can read from the transcript or watch him saying it, his reasoning for continuing to swallow it is that it then comes out the salivary glands to provide a topical benefit. Nor does he say there is a benefit to the teeth from fluoride brushing past it by swallowing.
LikeLike
Mary, you attempting exactly what I described in this article:
“Again and again I find anti-fluoride people using this tactic to deny any mechanism but “topical.” They thereby purposely deny any of the known beneficial effects of ingested fluoride. This bait and switch tactic is compounded by another bait and switch where the “topical” – referring to the reactions occurring at the tooth surface because of fluoride in saliva and biofilms – becomes a new “topical” – referring only to methods of application such as toothpaste and dentrifices. This tactic enables them to deny the beneficial roles of fluoride transferred from water to saliva during drinking, as well as that ingested.”
>
LikeLike
It should be very easy to show how Mary keeps misrepresenting Robin Whyman. Perhaps someone could actually get him to comment specifically on her distortions.
In the meantime I will just quote this from the document “Healthy Smile, Healthy Child ORAL HEALTH GUIDE FOR WELL CHILD PROVIDERS” which was prepared with Whyman’s participation and advice.
LikeLike
Whyman doesn’t say what Mary claims he said in the transcript Mary links to. End of that story.
LikeLike
Ken, You wrote, ‘please present evidence for your claim of skeletal fluorosis in India at 0.7 ppm F in drinking water. A reference or citation/link. Otherwise I will have to assume you are telling porkies.’
First, please note that I didn’t claim skeletal fluorosis ‘at 0.7 ppm/F in drinking water’. I wrote ‘water with between 0.7 and 1.6 ppm of fluoride’ (the 1.6 should have been 1.7 ppm/F).
I was not telling porkies. Here follows a reference/link as per your request. The (UK) Manchester Guardian published (9 July 1998 and 15 July 1998) parts one and two of ‘Ministry of not so funny walks’ which was authored by Fred Pearce. The articles relate to the grave situation in India where an estimated tens of millions of people have been chronically fluoride poisoned by naturally-occurring fluoride. Check the fifth paragraph from the bottom of part 2 – via this link http://www.nofluoride.com/guardian_india.cfm – and note the following wording, “In Britain, the Department of Health says the “optimum” fluoride dose for water supplies is 1 part per million. But in one Indian village studied in detail, Bhanakpur near Delhi, water with between 0.7 and 1.6 ppm of fluoride was enough to leave 17 per cent of the population suffering from the bent bones of skeletal fluorosis.”
Fred Pearce is an English journalist and author of numerous books who is based in London. He has reported on the environment, popular science and development issues from 64 countries and is an environment consultant for New Scientist Magazine.
LikeLike
Mary, you continue to be extremely entertaining! Now, people are not intelligent if they can’t read your mind to determine what you actually meant to say, when you said something else. That’s hilarious! Are we expected to read your mind on this latest comment, as well? Do you mean what you say here, as written, or are we supposed to discern what you actually meant to say, instead?
As far as my comment, the FANNZ version of the “transcript” of Whyman is indeed interspersed with editorial commentary and FANNZ highlighting of text, none of which is acceptable when attempting to provide accurate quotes. This just further demonstrates the fact that antifluoridationists who manage and maintain these websites have no idea as to what they are doing.
Whyman does not “admit” that fluoride has no systemic effect. That point is clear, but also irrelevant. What you seem not to understand is that in terms of a public health initiative such as water fluoridation it makes no difference what percentage is considered “topical” and what considered to be “systemic”. The success of public health initiatives are measured by the effect on the entire population exposed to the initiative. Water fluoridation has been proven in countless peer-reviewed studies to significantly reduce dental decay in the populations which were exposed to the initiative. As there is no other means of obtaining this degree of dental decay prevention for an entire population, which even approaches the cost-effectiveness of fluoridation, and as there have been no proven adverse effects of this initiative in its entire 68 year history, there simply is no valid reason not to implement and/or maintain it.
Steven D. Slott, DDS
LikeLike
Mary, with respect to the discussion of the systemic and topical anti-cavity effects of fluoride, what some individual “admits” has really little to do with the discussion.
I’ve cited some of the literature documenting a systemic (swallowed fluoride during tooth development.) If someone wishes to engage in this matter they really have to analyze the papers (like Kumar and Singh I previously cited) and explain why somehow they are mistaken.
How can tooth fluorosis protect against cavities if there is not a systemic effect? The protection is not trivial. Kumar quantifies it by comparing the protection from fluorosis to the protection from placing and maintaining sealants. Additional references can be given.
Oral public health professionals believe fluoridation is beneficial and safe. They do so because of the huge literature available.
Enough of the “he said, she said.” If you oppose you must have the discipline to actually engage the literature.
LikeLike
I don’t appreciate Charles Haynie of Hood River insinuating that I made up the delayed eruption effect of fluoride. There are many problems with Carlos and Gittlesohn’s analysis on the Newburgh- Kingston data from the early 60’s.
Just because *HE* isn’t aware of other studies that showed delayed tooth eruption doesn’t mean they don’t exist. Besides the numerous animal studies (some of the best biochemists in mineralized tissues demonstrated just HOW fluoride delays tooth eruption in many different animal models), there are several human studies that clearly point fluoride’s delay in tooth eruption.
Short EM, 1944
Ast DB & Fitzgerald 1960
Scheinen A 1964
Kunzel W 1976
Tseng et al 1989
Virtanen et al 1994
Bigeard L & Obry-Musset MA 1997
Nadler GL 1998
In these studies, the delayed eruption of permanent teeth in the fluoridated areas ranged from 0.13 years to 1.52 years.
Most of the above studies were attempts to show that fluoridation works.
When data is corrected for tooth eruption, there is no benefit of fluoridation (see http://www.ncbi.nlm.nih.gov/pubmed/15618533)
In the only prospective study in the US, Steven Levy’s group found that the fluoride intake is higher in subjects of low socioeconomic status
http://www.ncbi.nlm.nih.gov/pubmed/17138375
That is ONE of the reasons they get more dental fluorosis.
The other is a genetic predisposition.
In another paper
http://www.ncbi.nlm.nih.gov/pubmed/19054310
Levy’s group concluded
“Given the overlap among caries/fluorosis groups in mean fluoride intake and extreme variability in individual fluoride intakes, firmly recommending an “optimal” fluoride intake is problematic.”
Many studies have shown that the optimum may be 0.35 ppm or lower.
For example, see
Ekstrand KR, Christiansen ME, Qvist V, Ismail A. Factors associated with
inter-municipality differences in dental caries experience among Danish
adolescents. An ecological study. Community Dent Oral Epidemiol. 2010
Feb;38(1):29-42.
Despite this Dr. Levy served on several committees in the US and Canada supporting the recommended 0.7 ppm (EPA, Health Canada) and still is a cast-in-stone supporter of fluoridation. I can’t blame him. He’s a public health dentist. He got a lot of NIH funding to study the effects of daily low dose fluoride. Nobody in public health wants to hear that fluoridation might have been a big mistake.
Sure, many ground water sources already contain 0.3 ppm fluoride.
It occurs naturally in most water supplies.
But I really don’t understand the heavy-handed lobbying to get cities to make such a minor adjustment to the drinking water fluoride fluoride levels when the benefits are clearly not clinically relevant (after adjusting for all the confounders).
That brings up another point. None of the interventions studies involving the comparison between fluoridated and non-fluoridated communities were done properly. Dr. Levy is doing what is closest to the evidence we need. There is not a single, randomized, double blinded, prospective, placebo controlled clinical trial to prove fluoride at 0.7 ppm works. This is the gold standard that is required to approve any drug.
There must be something political about this whole issue.
As a dental scientist who served on that 2003-2006 US National Academy of Sciences Committee on Fluoride in Drinking Water, it saddens me that the science, which is actually weak on both sides of the argument, is being exaggerated for political reasons.
Dr. Hardy Limeback BSc PhD (Bochemistry) DDS
Professor Emeritus and former head of Preventive Dentistry
Faculty of Dentistry, University of Toronto
LikeLike
I can’t blame him. He’s a public health dentist. He got a lot of NIH funding to study the effects of daily low dose fluoride.
We know. We know.
It’s all a big conspiracy.
Claim CA321.1:
The conclusions of scientists are motivated by scientists’ pay; they cannot be considered objective. Claim CA321.1:
The conclusions of scientists are motivated by scientists’ pay; they cannot be considered objective.
It’s uncanny.
Science denialism always follows the same, predicable patterns.
Only the labels are different.
LikeLike
Hardy Limeback. Nice to see you join the discussion. I, for one, will be most interested to read the full text of the Bayesian study you cite in support of your delayed eruption theory as pertains to water fluoridation, as well as any others you cite which I may not have read already.
Your opinion on the validity of peer-reviewed observational studies on the effect of water fluoridation, notwithstanding, this public health initiative has been repeatedly proven beneficial in numerous such studies over its 68 year history. Your disdain for observational studies is well noted, however, public health initiatives are gauged by the effect on the entire population which has been exposed to the initiative. High quality observational studies provide entirely valid evidence of the effectiveness of such initiatives. This is especially true with fluoridation, given the near impossibility of conducting valid, randomized, double blind studies on this initiative which you and most other fluoridation opponents demand……your idea for the Alaskan study being a possible exception.
Steven D. Slott, DDS
LikeLike
Mr. Katesby.
I never said anything about a conspiracy. I have gotten to know Dr. Levy over the years. I have talked to him several times at different international meetings. I like him and he does great work.
We’re not talking about evolution here and calling ANY scientist a science denialist is a typical ad hominem approach in debating.
Let’s examine ALL the science…on both sides. Denying that the science doesn’t exist on one side of a two-sided controversial subject is not helpful. When the opposing science is an inconvenient (to use Al Gore’s adjective) problem, labelling it junk science is unfairly dismissive, especially when there are hundreds of peer-reviewed studies published in respectable international journals to support the other side.
At a National Oral Health Conference, John Warren (Warren, Levy & Broffit), using the data they had collected in the Iowa study, concluded
“For most fluoride exposure categories,
there appeared to be only slight
differences between the “caries only” and
“neither” groups, suggesting that blanket
recommendations for fluoride use may be
tenuous.”
Dr. Hardy Limeback
LikeLike
Hardy Limeback
The problem with the fluoride opponent perspective is that the evidence constantly presented as being scientific support for their arguments is generally suspect and invalid, as they have little understanding of science, and healthcare. That as well as the fact that the majority of this evidence does not pertain to fluoride at the level of 0.7 ppm. They fail to understand the difference between concentration levels, and thereby lump all effects of fluoride into one. The same pertains to dental fluorosis. You know as well or better than anyone that moderate/severe dental fluorosis is a rarity in regard to water fluoridation, yet fluoride opponents consistently seek to consider dental fluorosis to be but one single effect attributable to eater fluoridation. Those who operate the “fluoride-free” or “clean-water” whatevers, are some of the most egregious offenders. They haven’t the knowledge or understanding of science to have any idea as to what they are posting on these sites, yet they do so anyway, then do everything they can to steer people to them under the guise of being “authoritative” sources of information.
In spite of my failure to bow before you, I do respect you and your lifetime body of work. It is impressive, and I am not fool enough to not recognize that. However, with fluoridation opponents, you are the glaring exception, not the rule, by any means. With pro fluoridation advocates, just the opposite is true. If you truly want intelligent discussions on this topic, from both sides, this is where it needs to begin. Get rid of all the junk on “fluoridealert.org,” “fluorideresearch” and other such sites, and have these folks begin to utilize accurate information from reliable, respected sources, in their complete and proper context. Until that happens, there will constantly be the antagonism and lack of intelligent discourse that I know you wish to see disappear, as do I.
Steven D. Slott, DDS
LikeLike
I never said anything about a conspiracy.
Let me refresh your memory.
I can’t blame him. He’s a public health dentist. He got a lot of NIH funding to study the effects of daily low dose fluoride.
Sounds like a conspiracy to me.
We’re not talking about evolution here and calling…
Never said you were.
…calling ANY scientist a science denialist is a typical ad hominem approach….
Surely that depends if they are a science denier or not?
Duesberg, Wakefield, Behe, Sheldrake, Carter etc.
The list is extensive.
Plenty of people out there calling themselves scientists who are science deniers.
(shrug)
When the opposing science is an inconvenient (to use Al Gore’s adjective) problem, labelling it junk science….
Oh twaddle. Grow up.
Junk science is real. It exists.
Science denialism on a whole range of issues exists.
It’s a real thing.
…especially when there are hundreds of peer-reviewed studies…
Yes, yes, yes.
It’s the same ol’ same ol’.
Let’s cut to the chase, shall we?
Can you name a single scientific community that rejects the consensus on flouride?
LikeLike
@ Mr Limeback
Most of the above studies were attempts to show that fluoridation works.
Really?
They all set out with an agenda?
Sounds like conspiracy to me.
LikeLike
Hardy Limeback
Below is an email, with which I’m sure you’re well aware, between you and Chris Neurath of Paul Connett’s non-profit, American Health Studies, the umbrella for FAN. This email was generated in 2006 and is part of public records. In it you acknowledge first that it is no longer possible “to get the seemingly amazing differences between fluoridated and non-fluoridated communities that the Grand Rapids trial purportedly showed.” Exactly my point with your disingenuous demands for randomized, double blind studies.
More importantly, you also acknowledge that the early Grand Rapids study did indeed show a benefit of fluoridation even when making corrections for tooth eruption, that is not possible to show today due to the impossibility of sufficiently separating fluoridated and non-fluoridated populations. You clearly indicate that delayed eruption, if valid at all, is a matter of months, not years.
“If you make corrections of delayed tooth eruption of a few months (there’s no way it is two years delayed) there still seems to be a benefit of fluoridated water in the early Grand Rapids data (……you can’t explain away the Grand Rapids results with delayed tooth eruption).”
Lastly, as you state in your first paragraph, “No one should be critical or supportive of the fluoride and cancer literature without having some experience in epidemiology, toxicology, cancer risk assessment, clinical design and interpretation and years of experience.”
You might want to address this issue with your close affiliate, Connett, who has little or none of the qualifications you state one should have before attempting to assess the fluoride and cancer literature, yet who blusters forth anyway using the flimsy data of Bassin’s study to justify his unconscionable and irresponsible attempts to link fluoridated water to osteosarcoma.
Chris:
I think you are referring to Mark Diesendorf [mark@sustainabilitycentre.com.au]
Also, you left me a v-mail about Bassin. I’m not in a position to discuss the cancer data. No one should be critical or supportive of the fluoride and cancer literature without having some experience in epidemiology, toxicology, cancer risk assessment, clinical design and interpretation and years of experience. We had people that fit that description on the NAS committee. If you have any questions about the conclusions of the NAS report, I suggest you contact people who can address your concerns (e.g. Judith Klotz)
Regarding the Komarek study:
I posted several e-mails announcing the publication of this study as soon as it came out. In fact that group was probably the only group that read my poster at the IADR …and they read it VERY carefully (probably wondering if would scoop them….I bet they were relieved to see that I did not have a Bayesian analysis (I would need an expert statistician on my team to do that)) . My poster was about delayed eruption and the effect it would have on the various fluoridation studies going back to the early days of the Grand Rapids trial and follow all the trials (reporting DMFTs or DMFSs with increasing age). I reviewed the human literature on delayed eruption (public health people claim that the delay in eruption was simply because primary teeth were being protected and were being retained longer in the oral cavity, thereby delaying the eruption of the premolars and canines (it is well known that early extraction of primary teeth speeds up eruption of the permanent teeth) and found that there was more than a simple explanation of healthier primary teeth. There had to be an indirect endocrine effect on permanent teeth that erupt through bone to emerge into the oral cavity. Either that or more fluoride in the bone made it harder for osteoclasts to clear the way for erupting permanent teeth. The emergence time of the 6-year molar has been remarkably constant through the decades….until the introduction of fluoride in the middle of the 20th century. Virtanen’s paper in Denmark was the one that got me interested in the whole issue. I’m putting together an article that estimates the average delay.
Virtanen JI, Bloigu RS, Larmas MA. Timing of eruption of permanent teeth: standard Finnish patient documents. Community Dent Oral Epidemiol. 1994 Oct;22(5 Pt 1):286-8.
If you make corrections of delayed tooth eruption of a few months (there’s no way it is two years delayed) there still seems to be a benefit of fluoridated water in the early Grand Rapids data (……you can’t explain away the Grand Rapids results with delayed tooth eruption). What happens in the 60’s and every year after that is an increase in toothpaste exposure and the Grand Rapids results are no longer applicable. Fluoridation after fluoridation study became harder and harder to conduct to show a statistical benefit let alone a clinical benefit.
The Komarek study uses fluorosis as a measure of fluoride exposure. That’s not 100% accurate, as our graduate student (Anya Vieira) published. There are genetic influences on fluorosis and there may be other reasons for fluorotic-like lesions (e.g. antibiotics….as shown by Levy). Nowadays there is so much fluoride exposure (see our NAS review) that you can no longer get the seemingly amazing differences between fluoridated and non-fluoridated communities that the Grand Rapids trial purportedly showed. Even Kumar published a series of articles showing that the Kingston-Newburg differences disappeared over the years after fluoridation was started.
What Komarek does NOT discuss is that if the delayed teeth have fluorosis this means the fluorosis studies done to date should have corrected for this too. Comparing kids of the same age group would UNDERESTMATE dental fluorosis (unless you only look at the incisors at age 12…even then the mild cases from age 6 can turn to moderate cases and the moderate cases can turn to more severe cases.). I have case reports of dental fluorosis getting worse with age I want to publish.
It’s good that you’re reading the papers in detail. People really ignored Komarek’s work until you ‘rediscovered’ it (actually Micahel knew about it as well but I suspect he didn’t understand the math …I freely admit I don’t understand the math!…)
It took a committee of 12 people 2.5 years to thoroughly read a large part of the fluoride literature and we all didn’t read every single paper.
There is a danger to simply reading abstracts. You tend to either over-estimate the importance of a study but sometimes you miss gems like the Komarek study.
hardy
Dr. Hardy Limeback BSc, PhD, DDS Assoc. Professor and Head,
Preventive Dentistry, Faculty of Dentistry University of Toronto
124 Edward St. Rm 455
Toronto Ontario Canada M5G 1G6 416 979-4929 ext. 4461
Steven D. Slott, DDS.
LikeLike
Hello Dr. Slott:
“disingenuous demands for randomized, double blind studies???”
No, it’s an honest demand and it can be EASILY done, given the will of the public health sector to get an answer for MODERN times (not the pre-fluoridated toothpaste era that was during the Grand Rapids ‘experiment’). Stephen Levy could have designed his long-term study to do this.
The average American community could participate (you have to be in a non-fluoridated community).
You randomly select households into the study. Levy showed you only need about 600 kids from a few dozen households in Iowa at the end of the trial for a large enough sample size. You provide every household with an endless supply of drinking water in large plastic bottles. Not very costly. RO water can be made for less than $0.15/L. Everyone in the household uses the water for cooking, making beverages and of course, drinking. A log is kept on the actual water consumed in beverages. Someone from outside the study adds fluoride to the test water at 0.7 ppm. Water A and Water B are compared and the identity which is the test water is not revealed until AFTER the stats are completed. Since fluoride is odourless and tasteless, the subject is blinded. The examiners don’t know which water supply is the test until the end of the trial. In a high caries community, you could stop the trial early (like they did in for Grand Rapids) but this time the study is randomized on an INDIVIDUAL basis. There were so many errors with the Grand Rapids that the large difference found could have been explained away by many things (I found that out much later after carefully reviewing the studies from the 40’s and 50’s). How do you ‘randomize’ two towns into a study? How do you control for confounding factors when you are comparing towns and not individuals?
The nice thing about randomization is that the all the confounders that have to be taken into consideration in cross-sectional studies (toothbrushing frequency, sugar and pop intake, milk intake, vitamin D levels, etc etc), would be taken care of through the randomization process.
That’s the whole reason for doing an RCT.
Because the caries increment rates are so low these days, with half the kids not getting ANY caries, you might have to do the study for several years. But then you could answer whether kids AND adults benefit.
I doubt very much, with the widespread use of fluoridated oral care products that you’ll EVER get the same results as the Grand Rapids trial.
The York reviewers incorrectly conducted a meta analysis on studies that should never have been included because they were so weak. The should have done what any Cochrane reviewer would have done and say “Sorry, we could not find any studies with sufficient robustness in clinical protocol design and, therefore, we decided NOT to do a meta analysis.”
Instead they included the old, faulty studies of the Grand Rapids days and mixed them with a few cross-sectional ecological studies and proclaimed that fluoridation had a benefit when clearly modern studies are having a heck of a time showing ANY clinically relevant benefit at all.
Slade found a statistical reduction of caries in people after a lifetime of fluoridation
http://www.ncbi.nlm.nih.gov/pubmed/23456704
but that difference is actually only one filling saved.
This is clearly not the cost savings of $38 for every dollar spent on fluoridation. In fact his study suggests it may be less expensive to simply fix that one filling.
Regarding dose versus concentration.
“They fail to understand the difference between concentration levels, and thereby lump all effects of fluoride into one.”
When we did our Montreal vs Toronto hip bone study I was shocked to see fluoride levels in bone in Toronto (fluoridated since 63) nearly twice as high as the bone from non-fluoridated Montreal and that the upper levels reached 2500 ppm in the Toronto bone samples. Those are levels that are associated with increased bone fracture.
What bothers me, though, is the rejection of all the fluoride toxicity studies looking at high levels of fluoride, as if these high levels are never seen in the body. The kidney can have as much as 5 ppm. So can the bladder. But bone, with 2500 ppm is actually quite toxic to cells. The osteoclast has to remodel bone. It does so by forming hemidesmosomes, isolating the dorsal surface between it and the bone surface to which it is firmly attached. It then pumps protons between it and the bone surface lowering the local pH. That acid dissolves ALL apatite, including fluorapatite, releasing bound fluoride. Because the pKa of HF is 3.4, most of the fluoride will be in HF form (neutral) and it easily passes through the cell membrane into the osteoclast. Once in the cell, the intracellular neutral pH causes the HF molecules to dissociate into fluoride ions which then inhibits all sorts of intracellular enzymatic reactions.
When the osteoclast disassembles its hemidesmosomes, the fluoride-rich fluid ‘leaks out’ only to expose nearby osteoBLASTS. The osteoCLAST moves on and works on a another area of bone but eventually undergoes apoptosis (a premature death that is presumed to be programmed into the cell). It is theorized that osteoclast apoptosis is in part due to fluoride toxicity. Now you have a biological rationale as to why fluoride is so toxic to bone cells and is thought to be a promotor of bone cancer. (See our 2006 Report).
Finally, I wouldn’t be so quick to call the science on Fluoridealert.org ‘Junk’. FAN is an enormous resource for peer-reviewed studies examining fluoride toxicity that were published in respectable journals with international reputations. On the other hand it is really hard to find fluoride toxicity studies in the dental literature. I find that disappointing.
Dr. Hardy Limeback
LikeLike
Someone should do the easy randomized double blind studies, put the whole issue to bed and wait for their Nobel prize nomination.
LikeLike
Hardy Limeback
You’re kidding about your proposed study design, correct? Get the kind of strictly disciplined behavior required by your design from a few dozen randomly chosen households, over a period of years? Kids in school, parents in the workplace. Kids keeping accurate records of the beverages they consume. Eating out in restaurants. Visits to see Grandma and trips to an infinite number of other places. Relocation of residence, new jobs, different schools. You said it yourself…..Levy concluded that there are far too many variables to determine a more precise optimal level than we have. This most certainly applies to your design, as well. Again, it is nearly, if not completely, impossible to run a randomized, double blind now and obtain any useful data. You acknowledged this in your email to Neurath. I stand by my statements on that issue.
The point of Grand Rapids is that when it WAS possible to sufficiently segregate fluoridated from non-fluoridated groups, they found significant reduction in decay in the fluoridated areas. That modern studies are not finding the same differences is a function of halo and the inability to adequately segregate fluoridated from non-fluoridated. Even so, they are still finding reductions in fluoridated areas. Even the one cavity you trivialize, gone untreated, as an overwhelming amount of them do, can lead to the loss of an entire dentition, with a lifetime of associated pain, debilitation, and related, major systemic problems, as well as even death. These problems are well documented and real, not the “what ifs” constantly put forth by fluoridation opponents.
In your first comment in this section you describe fluoridation as “such a minor adjustment to the drinking water fluoride levels” in relation to benefits. Yet when considering purported systemic problems related to fluoridation, this amount all of a sudden becomes a very significant quantity. The reality is that the amount added IS nothing more than a minor adjustment to the existing level of fluoride for the purpose of attaining the optimal level. The amount added is not significant enough to be a causative factor of the myriad of disorders that opponents claim to be possibly occurring. This is exactly why it is so ridiculous to fight as long and as hard, as have opponents, against this initiative.
If you view the biased, filtered and edited information on “fluoridealert.org” to be an “enormous resource” then it is no mystery as to how you arrive at your conclusions in regard to fluoridation. I prefer unfiltered, unedited information from reliable, respected and original sources.
Steven D. Slott, DDS
LikeLike
Hardy Limeback
Your reference to York is ironic, given the dependence of Connett and his followers on Grandjean and Choi. If ever there was a meta-analysis that should have been scrapped due to poor quality of studies, it it is that Harvard Review.
Steven D. Slott, DDS
LikeLike
@ Hardy Limeback
You propose a double-blinded study of a known and proven health measure.
The same population-based study design which has shown fluoridation to be safe and effective has been used to show the causal relationship between negative health effects of:
-Alcohol
-Smoking
-STD’s
With your reasoning, is it safe to say that you would propose double-blinded studies to show that smoking does indeed cause lung disease and cancer? Alcohol and fetal-alcohol syndrome or cirrhosis? Sexually transmitted diseases and brain damage or pelvic inflammatory disease?
Certainly as a scientist I can understand the demands that you make of fluoridation. However, not only is this demand counter to arguments (& legal action) that would be brought about from your suggestion that double-blinded studies be necessary for population-based studies, it would never be approved by any human subjects committee. To withhold a known health benefit from people to prove something that a scientist desires to research is unethical, immoral, and hypocritical to suggest. Would you suggest the same for alcohol, smoking, and STD damages just to satisfy a scientist’s demand? I think not.
Johnny Johnson, Jr., DMD, MS
Pediatric Dentist
Diplomate, American Board of Pediatric Dentistry
LikeLike
Hi –
Seeing as we are touching on the subject of studies surrounding rates of
Osteosarcoma and fluoride in drinking water, could someone please elucidate whether this study is relevant to the discussion here?
“Fluoride in drinking water and osteosarcoma incidence rates in the continental United States among children and adolescents” in Cancer Epidemiology 36 (2012) e83–e88
In the conclusion it is stated;
“While causality cannot be inferred from this
ecological analysis, our findings are consistent with the hypothesis
that community water fluoridation has no influence on the
development of osteosarcoma for either sex or age group during
childhood and adolescence”
I notice on the FANNZ site there is a lot of noise surrounding the Bassin study.
Doesn’t the above study help clear all this up?
LikeLike
In response to your posting, Dr. Slott, I will cut and paste so as not to miss anything. I’m sure that is allowed. Your comments are in quotes.
“You’re kidding about your proposed study design, correct?”
No, not at all.
Without an RCT, the evidence is much less definitive. FAR less than the ‘overwhelming’ evidence claimed by fluoridationists.
The ‘overwhelming’ evidence FOR fluoridation is the same term that can be used for the evidence against, including the Harvard IQ studies.
“Get the kind of strictly disciplined behavior required by your design from a few dozen randomly chosen households, over a period of years? Kids in school, parents in the workplace. Kids keeping accurate records of the beverages they consume. Eating out in restaurants. Visits to see Grandma and trips to an infinite number of other places. Relocation of residence, new jobs, different schools.”
No. you simply pick a non-fluoridate city where there is no chance of the halo effect. Vancouver BC is such a city. The beverages (reconstituted orange juices) and even beers are bottled BC, rather than bottling them in Toronto and shipping them all a cross the country. Vancouver’s water is pristine. Almost no calcium to interfere with fluoride. Never been fluoridated. The halo effect has been an excuse by the fluoridationists all along. Without an RCT you can’t say there is a halo effect. Fluoridationists: “Gee, fluoridated water must be working because kids living in non-fluoridated areas drink pop made with city fluoridated water and eat occasionally in the the fluoridated city.”
Ah, no. That little extra fluoride has likely minuscule effect. If anyone moves out of the non-fluoridated city in my RCT they are simply excluded from the clinical trial. That’s how RCTs are set up.
It’s simple and it could have been done long ago. Don’t let the PEW people or CDC or ADA tell you otherwise. I know you’re not a researcher, so if you’re interested, you can familiarize yourself with how a properly designed RCT is set up, carried out and analyzed statistically.
“You said it yourself…..Levy concluded that there are far too many variables to determine a more precise optimal level than we have.”
So you’re finally admitting we need and RCT to answer whether fluoridation HAS in optimum dose???
“This most certainly applies to your design, as well. Again, it is nearly, if not completely, impossible to run a randomized, double blind now and obtain any useful data. You acknowledged this in your email to Neurath. I stand by my statements on that issue.”
It’s not ‘completely impossible….difficult, tricky, yes. Not impossible.
And by the way….how DID you get that PRIVATE email? It certainly was NOT in the public record. If you obtained it without any of the authors’ permission (I certainly did not give you the permission to reproduce a private email on the internet) you might have to face some consequences in the future.
I live in Canada. Are you telling me that my emails are being monitored by people in the US? Are you working for the Rupert Murdoch or something?
“The point of Grand Rapids is that when it WAS possible to sufficiently segregate fluoridated from non-fluoridated groups, they found significant reduction in decay in the fluoridated areas.”
No. It was before fluoridated toothpaste, mouthwash, fissure sealants, xylitol and sugarless chewing gum, diet soda pop etc. etc.
Those were the dirty days of WWII when recruits were rejected from the army due to huge dental decay problems. Fluoride may have provided some benefit then, but today, half of our kids’ generation is cavity free.
I discuss all that in my textbook.
“That modern studies are not finding the same differences is a function of halo and the inability to adequately segregate fluoridated from non-fluoridated.”
As I pointed out until you do an RCT you can’t say there is a halo effect.
It is minuscule at the most because of the overwhelming effects of fluoridated oral care products.
Have you read this paper?
Bratthall D, Hänsel-Petersson G, Sundberg H. Reasons for the caries decline: what do the experts believe? Eur J Oral Sci. 1996 Aug;104(4 ( Pt 2)):416-22; discussion 423-5, 430-2.
A real eye opener. Fluoridated water wasn’t even close on the top of their list for the reason for the decline of caries in modern times.
“Even so, they are still finding reductions in fluoridated areas. Even the one cavity you trivialize, gone untreated, as an overwhelming amount of them do, can lead to the loss of an entire dentition,”
Wow. This really is an exaggeration.
“with a lifetime of associated pain, debilitation, and related, major systemic problems, as well as even death.”
Gee, even the character that Tom Hanks played extracted his own infected molar with a skate blade when he couldn’t take it any more. (the movie ‘The Castaway’.)
Not too many people have a lifetime of pain from ONE infected tooth.
Most people seek a dentist if they are in such great pain and don;t suffer for more than a few days or weeks.
Oh I forgot, 80% of dentists don’t treat patients on Medicaid in the US.
Maybe they think adding fluoride to drinking water gets them off the hook and they don’t have to treat people on welfare. At least you yourself provides service to the poor. So many dentists in the US don’t.
“In your first comment in this section you describe fluoridation as “such a minor adjustment to the drinking water fluoride levels” in relation to benefits. Yet when considering purported systemic problems related to fluoridation, this amount all of a sudden becomes a very significant quantity.”
Well ya. Dental fluorosis from fluoridation is now rampant in the US. If 50% of the kids in the US are cavity free, and yet almost the same number have two or more teeth with mild to moderate fluorosis, then fluorosis is a bigger problem than dental decay. Fluoridationists keep saying….”Oh its a minor cosmetic effect. Most people don’t see it.”
When they do see it, though (about one in 10 kids these days in fluoridated cities) they WANT it treated. It’s very costly to treat. I can only assume that dentists don’t want to lose this cosmetic business and therefore continue to support fluoridation.
Nothing, other than a reduction in dental decay was supposed to happen with fluoridaiton. Dental fluorosis is a sign that the rest of the body has had too much fluoride exposure. Just ONE study showing negative effects on the body such as the thyroid (reviewed in our NRC report), pineal gland (never addressed by fluoridation proponents), bone effects of a lifetime of fluoride ingestion (delayed eruption due to increased fluoride in bone and deciduous tooth roots resulting in malocclusion), DENTIN fluorosis -we published a study on that- ….just one negative study should have brought an end to fluoridation. As these negative studies continue to pile up, fluoridationists get nastier through ad hominem attacks, rather than dealing with the published studies.
“The reality is that the amount added IS nothing more than a minor adjustment to the existing level of fluoride for the purpose of attaining the optimal level.”
Which you now agree can’t be determined so why say there is one?
The rest of the world has set the maximum at 1.5 ppm. That’s silly. Knowing the concentration of the drinking water is like knowing the concentration of banana flavoured amoxicillin for pediatric use. You need to know the body weight in order to properly figure out the dose. That’s not done with drinking water. Someone drinking 1.5 L of 1.0 ppm fluoridated water consumes the same DOSE of fluoride as a person drinking 2 L of 0.7 ppm )or 1 L of the maximum allowed at 1.5 ppm). You cannot avoid the overlap between what fluoridationists consider ‘therapeutic’ and what the European nations and most others (like Canada) consider borderline toxic.
There are millions of people in the US being poisoned by 4 ppm just because the EPA has not gotten off its butt to go along with the rest of the world and declare the MCLG as 1.5 ppm.
“The amount added is not significant enough to be a causative factor of the myriad of disorders that opponents claim to be possibly occurring.”
Really?
Dental fluorosis. Interference with thyroid. Calcification of the pineal gland. Arsenic in fluoridation chemicals.
“This is exactly why it is so ridiculous to fight as long and as hard, as have opponents, against this initiative.”
Not at all. Fluoridated water should be safe for ALL. Setting the ‘therapeutic’ level to 0.7 ppm does not protect ALL persons in the community.
If you view the biased, filtered and edited information on “fluoridealert.org” to be an “enormous resource” then it is no mystery as to how you arrive at your conclusions in regard to fluoridation. I prefer unfiltered, unedited information from reliable, respected and original sources.
I bet you’ve been to the website to look up papers otherwise you wouldn’t have the ‘opinion’ it is biased. I think you have to be careful not to libel the authors of the FAN website.
There are papers there that I never knew existed. Of course I look up the original papers. I have access to them. That’s how I determine that a lot of profluoridation studies are in fact flawed. I also recognize the limitations for many of the negative studies that FAN cites.
“Your reference to York is ironic, given the dependence of Connett and his followers on Grandjean and Choi. If ever there was a meta-analysis that should have been scrapped due to poor quality of studies, it it is that Harvard Review.”
Gee. Is that what they are telling you? Have you read the Chinese studies? Well I have. In fact I presented an analysis of the various studies at the IADR in Toronto. Some of them were done with better controlling of confounders than fluoridation studies. Look it up.
Dr. Hardy Limeback
LikeLike
Christopher
There is overwhelming scientific consensus that there is no valid evidence linking water fluoridation to ANY cancer. This is why it is so despicable that Connett uses highly questionable preliminary data from one study, Bassin, to fear-monger about osteosarcoma. Tens of millions of US citizens have been ingesting fluoridated water over the past 68 years. The incidence of osteosarcoma in the US is 500-700 per year. Enough said.
Here are a few more opinions on this issue:
A review of worldwide studies by The International Agency for Research on Cancer (IARC) concluded there was no evidence of an increase in cancer rates associated with fluoride in drinking water.
——International Agency for Research on Cancer, IARC Mondographs on the Evaluation of Carcinogenic Risks of Chemicals to Humans, Volume 27. 1982
• The San Francisco Department of Public HealthOccupational Health and Environmental Health Section states that within a search of relevant peer reviewed medical literature to September 2005, a total of seven (7) epidemiological studies were discovered, none of which showed a relationship between fluoride exposure and osteosarcoma
—— (Moss et al. 1995, Gelberg et al. 1995, Freni and Gaylor 1992, Grandjean et al. 1992, McGuire et al. 1991, Mahoney et al. 1991, Hrudey et al. 1990).
——San Francisco Department of Public Health, Current Scientific Evidence: Water Fluoridation is not associated with osteosarcoma. 2005, http://www.sfdph.org/phes/ water/fluoride/Osteosarcoma_fluoride fact_sheet.pdf
Three small case control studies of osteosarcoma (McGuire et al 1995, Gelberg et al 1995, Moss et al 1995) have been reviewed by the Australian National Health and Medical Research Council in 1999. None of these studies found any evidence of fluoride increasing the risk of osteosarcoma.
——-Ahokas, J., et al., Review of water fluoridation and fluoride intake from discretionary fluoride supplements: review for NHMRC. 1999. Available at http//www. nhmrc.gov.au/advice/pdfcover/fluocov. htm, Royal Melbourne Institute of Technology and Monash University: Melbourne.
The York Review (2000), a systematic review of 214 studies of varying quality, found no clear association between fluoridation of water and osteosarcoma.
——-McDonagh M S, et al., Systemic review of water fluoridation. BMJ, 2000. 321.
A study by Hoover et al found no relationship between osteosarcoma and fluoridation. This study is important because of the large numbers involved (125,000 incident cancers, and 2.3 million cancer deaths).
——Medical Research Council Working Group, Water fluoridation and health. 2002, Medical Research Council: United Kingdom.
In 2002 the British Medical Research Council agreed that overall, evidence does not suggest that artificially fluoridated water increase the risk of cancer.
——-Medical Research Council Working Group, Water fluoridation and health. 2002, Medical Research Council: United Kingdom.
A review of fluoride by the Scientific Panel on Dietetic Products, Nutrition and Allergies published by the European Food Safety Authority in 2005, found no increased risk of cancer from drinking fluoridated water.
——European Food Safety Authority, Opinion of the Scientific Panel on Dietetic products, Nutrition and Allergies on a request from the Commission related to the Tolerable Upper Intake Level of Fluoride. The EFSA Journal, 2005. 192: p. 1-65.
Steven D. Slott
LikeLike
Hardy Limeback
Fine, you think it’s so easy to discipline a few dozen randomly chosen households to conform to the rigid discipline necessary for such a study, then do it. Shouldn’t take too much effort on your part. Of course, once done, that will remove a major excuse that fluoridation opponents constantly seek to use, so maybe that’s a reason that you and other opponents haven’t taken it on.
As far as your lame legal threat, now that is a true, bonafide, antifluoridationist tactic. It appears that I have accorded you undue respect by not referring to you as an antifluoridationist, the term to which Connett takes exception. If you’re going to attempt bush league tactics such as that, then you’re certainly no more deserving of respect than any other antifluoridationist, and will be treated as such. Your email was on the Juneau City website as a matter of public record. If you’re so worried about your true thoughts being exposed, then don’t put them out on the internet.
Steven d. Slott, DDS
LikeLike
As these negative studies continue to pile up, fluoridationists get nastier through ad hominem attacks, rather than dealing with the published studies.
Claim CA110:
Evolution is a theory in crisis; it will soon be widely rejected.
It’s uncanny.
Science denialism always follows the same, predicable patterns.
Only the labels are different.
Can you name a single scientific community that rejects the consensus on flouride?
LikeLike
Hi Blossom,
Just commenting on your “evidence” that you furnish in support of your claim that skeletal fluorosis can occur at levels between 0.7 and 1.7 ppm of fluoride.
You provided this link:
http://www.nofluoride.com/guardian_india.cfm
Not a scientific study, a journal article, or even an op-ed written by a scientist…
Are you serious? A 15yr old newspaper article written by a journalist!!
A jounalist who has written articles questioning climate change no less!!
Is it any wonder people opposing fluoridation attract criticism.
LikeLike
Exactly Christopher. And Limeback wants respect for antifluoridationist arguments?
Steven D. Slott, DDS
LikeLike
firstly No, it’s an honest demand and it [randomized controlled studies] can be EASILY done, given the will of the public health sector to get an answer for MODERN times
later It’s not ‘completely impossible….difficult, tricky, yes. Not impossible.
are we confused yet? and what happened to the all caps?
LikeLike
Hey Dr. Limeback,
Seriously, again with the fluorosis claim:
“Fluoridationists keep saying….”Oh its a minor cosmetic effect. Most people don’t see it.”
When they do see it, though (about one in 10 kids these days in fluoridated cities) they WANT it treated. It’s very costly to treat. I can only assume that dentists don’t want to lose this cosmetic business and therefore continue to support fluoridation.”
I have to admit, I’m surprised at your statement again that you truly believe that 1 in 10 kids “WANT” fluorosis treated, let alone see that they may have it. You mentioned this in an exchange we had in another forum. You stated how these folks want treatment so badly that it’ll cost them $1000’s of dollars to treat.
However, you then went on to state that YOU had a patient that had fluorosis that wanted it treated. You recommended a minimally invasive procedure, enamel microabrasion, to treat the patient. The patient did not agree with your tx plan, and went to a classmate of yours who treated the fluorosed teeth with veneers as I recall. I could go back and check my notes on this, but that was your point. Someone else treated your patient and essentially it upset you.
Your empirical observations of fluorosis and treatment requests from your patient pool appear to be quite skewed. Certainly, you do not give supporting literature to substantiate your position. Only your anecdotal observations. And as a practicing pediatric dentist of 30 years in the United States, I will tell you that you are skewed as well in your extrapolations of your observations to the general population. Your perceptions are your opinions, same as mine. They are not a consensus opinion, only observations and personal opinions.
Perhaps re-reading the following reference may help you understand the fluorosis and perception here in the United States, where 0.7ppm fluoride in the water is considered safe by even the 2006 NRC Review Panel, for which you were 1 of 12 members:
“A literature review of aesthetic perceptions of dental fluorosis
and relationships with psychosocial aspects⁄oral health-related quality of life”
Community Dent Oral Epidemiol 2010; 38: 97–109, Chankanka O, Levy SM, Warren JJ, Chalmers JM.
“More recent studies with methodological improvements to assess impact on quality of life clearly showed that mild fluorosis was not a concern.”
I have to believe that children and adults in Canada are similar in their experiences to those here.
Two last points.
1. If a double blind study is easy (or not) to do, as you’ve stated, why don’t you do it?
2. If you’ve read the Chinese studies you said that you did above, please direct me to the English translated versions of these studies. As far as anyone can see, only one of these studies was translated into English. You can email the pdf’s to me if you’d prefer instead of directing me to FAN’s website.
Thanks Hardy.
Johnny Johnson, Jr., DMD, MS
Pediatric Dentist
Diplomate, American Board of Pediatric Dentistry
LikeLike
<emDr. Johnny Johnson | November 10, 2013 at 5:43 am |
Are you comparing the negative health effects of STDs with the fluoridation issue?
This seems quite strange. I can’t imagine that anyone thinks there is a “debate” around the pros and cons of STDs or any other disease.
Is there a group on the internet promoting the positive benefits of having chlamydia or AIDS?
LikeLike
Are you comparing the negative health effects of STDs with the fluoridation issue?
This seems quite strange. I can’t imagine that anyone thinks there is a “debate” around the pros and cons of STDs or any other disease.
Is there a group on the internet promoting the positive benefits of having chlamydia or AIDS?
(facepalm)
LikeLike
Hello Dr. JJ.
Dr. JJ: Your empirical observations of fluorosis and treatment requests from your patient pool appear to be quite skewed. Certainly, you do not give supporting literature to substantiate your position. Only your anecdotal observations.
response: The increased fluorosis in fluoridated communities has been documented in several studies. See the York review, where one in every 8th child had ‘objectionable’ fluorosis. And they included earlier studies where the fluorosis rates were lower which means the fluorosis prevalences of ‘objectionable’ fluorosis was even higher in modern times.
See my blog for a discussion.
http://cof-cof.ca/2012/09/dr-hardy-limeback-bsc-phd-biochemistry-dds-dental-fluorosis-permanent-tooth-scarring-caused-by-fluoridation/
DR. JJ: If a double blind study is easy (or not) to do, as you’ve stated, why don’t you do it?
Response: I was busy studying enamel development (isolating and sequencing amelogenins), then turning to studying the effects of fluoride on bone, enamel and dentin.
It is actually the public health dental researchers that have failed to do a proper RCT. It’s their mandate. Instead of conducting an RCT, they have spent MILLIONS of US tax payer dollars looking at stats. Do the study already.
Thank goodness I’m out of the ‘publish or perish’ rat race of academia. I’ve retired from academics. I’d rather treat patients than to put up with the crap I got from my colleagues over my public stand against fluoridation.
Dr. JJ: If you’ve read the Chinese studies you said that you did above, please direct me to the English translated versions of these studies. As far as anyone can see, only one of these studies was translated into English. You can email the pdf’s to me if you’d prefer instead of directing me to FAN’s website.
Response: Here’s what we reported in the 2006 NRC report.
“A few epidemiologic studies of Chinese populations have reported IQ
deficits in children exposed to fluoride at 2.5 to 4 mg/L in drinking water. Although the studies lacked sufficient detail for the committee to fully assess their quality and relevance to U.S. populations, the consistency of the results appears significant enough to warrant additional
research on the effects of fluoride on intelligence.”
Only one of these studies in English? Why…because you said so? Did you check?
Fluoridationists have misrepresented ‘lacked sufficient detail’ with ‘were not conducted properly”. They simply accuse ALL Chinese epidemiologists studying in this field to be crappy researchers. I can tell you that they are actually very careful researchers for the most part. Some of their research puts North American research to shame.
Furthermore, there have been a lot of studies published since the 2006 NRC report. Some have been conducted in other countries and published in English. Some have done a better job controlling for confounders than many fluoridation cross-sectional ecological studies. Choi et al from Harvard thought there there were enough studies to do a meta analysis and found a consistent negative association between fluoride intake and lowered IQ. In some cases, the clinical investigators actually measured the urine fluoride levels, something that public health dentists RARELY do in fluoridation studies.
Then fluoridationists say that the fluoride levels were too high in the Chinese studies. In actual fact the intakes were comparable to US intakes for some of the studies, since the subjects were living in remote areas where fluoridated toothpaste and mouthwash were not being used.
They were especially relevant to some US and Canadian communities where fluoride in drinking water ranges from 2 to 4 ppm. People in those areas who can’t afford water filtration units, are increasing their risk of raising children with lowered IQ. The concern for this is real. If it is true that the overall normal IQ distribution curve is shifted to a lower IQ of only 5 points (when the average is 100), it means there will be millions of fewer geniuses and millions more mentally challenged in the US (these occur at the tail ends of the normal distribution curve).
If you want to read the studies for yourself, Dr. J., I suggest you contact FAN. They paid for them to be translated. It’s kind of odd that the studies were criticized by people who actually never read them.
The NRC committee made a list of suggestions for more research. Every 10 years a new committee is struck to look at fluoride. I started on the NRC panel in 2003. It’s time another committee were struct. But the EPA has yet to act on our recommendation to lower the MCLG of 4 ppm. I wouldn’t be surprised if a few more years pass and the research we suggested will not have been done and fluorosis rates will continue to rise.
I think Americans should wake up and smell the roses. There are far too many studies now that show fluoride toxicity. There is no such thing as an ‘optimum’ dose that ‘guarantees’ safety.
Dr. Hardy Limeback
LikeLike
Thank goodness I’m out of the ‘publish or perish’ rat race of academia. I’ve retired from academics. I’d rather treat patients than to put up with the crap I got from my colleagues over my public stand against fluoridation.
Gosh, that sounds so very familiar.
“I’ve just gotten kind of blase about submitting things to journals where you often wait two years to get things into print. And I find I can actually get the turnaround faster by writing a book and getting the ideas expressed there. My books sell well. I get a royalty. And the material gets read more.” [Chronicle of Higher Education, December 21, 2001]
William A. Dembski
Then we could do some label swapping.
Shall we? We shall.
Paging Dr Deusberg. Paging Dr Deusberg….
“Thank goodness I’m out of the ‘publish or perish’ rat race of academia. I’ve retired from academics. I’d rather treat patients than to put up with the crap I got from my colleagues over my public stand against the link between HIV and AIDS”.
“Dr” Wakefield? Are you out there?….
“Thank goodness I’m out of the ‘publish or perish’ rat race of academia. I’ve retired from academics. I’d rather treat patients than to put up with the crap I got from my colleagues over my public stand against vaccination.”
Yep, it’s the same ol’ same ol’.
Evolution vs. Creationism:Experts vs. Scientists-Peer Review
LikeLike
Dr Limeback – Thank you for speaking out. We really appreciate it. Keep up the good work.
LikeLike
I would like to express my thaindividuals’ve been meaning to raise some of your mentioned issues but lacked the time, and with my lower levels of expertise often what has been mentioned is ignored, despite the hours of reading on the topic, and footwork generated.
It also saddens me that many of these individuals here claim to be pro science, and express a desire for reasoned debate, and yet fall so far with poor rhetoric
LikeLike
“We” being people like Shane. How comically sad.
LikeLike
I think this comment best highlights what I have just said.
Lets leave this red herring alone and move away from the ad hominems eh?
LikeLike
Arthur, in regard to your question as to whether there is a group promoting the “positive benefits of chlamydia or AIDS”……. it would not surprise me in the least if there were.
Steven D. Slott, DDS
LikeLike
Doc Jones,
The sole point in mentioning the population-based studies which clearly showed an association between health effects of STD’s, smoking, and alcohol use are the same which have been used in reviewing water fluoridation in the United States.
No one has called for randomized clinical trials for proof positive that STD’s, smoking, and alcohol use cause detrimental health effects. If they have, they certainly need their heads examined. And to suggest that anyone is comparing and contrasting any detrimental effects of STD’s with fluoridation is either confusion on your part, or willful denigration of the messenger.
Community water fluoridation in the United States has never been shown to cause any adverse health effects in anyone. To suggest otherwise is to take one’s own opinion over the consensus opinion of The Community Preventive Services Task Force, and expert group tasked with critical review of the latest and best science available, and to arrive at a consensus opinion for the best care recommendations for communities. Taking one’s own opinion over an expert group is fine for opinion, but not scientific facts.
Calling for RCT for fluoridation, a practice with a safe and effective 68 year history in the U.S., is a thinly veiled position of those opposed to fluoridation in general. Hardy Limeback takes the same approach. Thankfully, it takes more than one scientist to arrive at consensus. We might still be traveling by foot when we weren’t dying from preventable childhood diseases if this rationale were followed.
LikeLike
Lets leave this red herring alone and move away from the ad hominems eh?
Speak English.
Find out what a “Red Herring” actually means.
Look it up.
Same diff with “ad hominem”.
Look it up, you idiot.
(Hint: No, I didn’t just use an ad hominem.)
LikeLike
Hardy,
Did I check on the translated studies? Better yet, why don’t you supply a pdf of the translated studies?
FAN had them translated? Since when does a group paying to translate studies from another language for self-benefit get to use their own translations to publish literature in a peer-reviewed journal? Would you accept this type of protocol if you were dealing with studies published in another language if only I were to interpret them on fluorosis? Be honest with yourself and the others here. Of course you’d be objecting. Perhaps not if they agreed with your empirical observations. But I suggest that your objections would be vehemently opposed if they did not agree with you.
Your TF scale is quite interesting I must admit. It departs from the Dean Index, yet uses the same definitions that Dean used, with some notable exceptions. You classify as “Moderate, TF 6” teeth that clearly exhibit enamel hypoplastic defects. This departs from the Dean Index in a major, and perhaps purposefully intended manner.
You state in your blog:
“Having treated dozens of children for dental fluorosis I can say from my own experience as a practicing dentist that these children are psychologically and socially affected by their dental ‘scarring’.”
I find it extremely disappointing for a scientist of your calibre to base your entire objection to what you’ve seen and treated on the “dozens of children” you’ve had in your practice. Your experiences are minimal, and are biased by your own opinion. My experiences are vast, having treated 10’s of thousands of children over a 30 year clinical practice as a Pediatric Dentist. My opinion is biased by my clinical experiences. I too have treated children with what appeared to be fluoride-related enamel discolorations. Interestingly, my 3 decades of treating only children has led me to the conclusion that less than 1 child per year had an enamel discoloration that not only bothered them when they smiled, but also desired some minimally invasive treatment. Enamel microabrasion treatment. Not EVER the aggressive crowns or veneers as you make sound commonplace.
I again refer you to the reference:
“A literature review of aesthetic perceptions of dental fluorosis
and relationships with psychosocial aspects⁄oral health-related quality of life”
Community Dent Oral Epidemiol 2010; 38: 97–109, Chankanka O, Levy SM, Warren JJ, Chalmers JM.
“More recent studies with methodological improvements to assess impact on quality of life clearly showed that mild fluorosis was not a concern.”
You have a bone to pick. That’s ok. It’s your own opinion. Write a blog. Write a book. Or perhaps jump back into the rat race and have your opinions peer-reviewed for publication in a credibly recognized referred journal. Failing that, your opinions are no more valid than mine. The only difference is that you’ve been in the sheltered halls of academia too long, with few years of dental practice in the private sector as you’d stated previously to me. In that vein of clinical experience, my experiences are far more vast and valid than yours for the population that I’ve seen in the U.S.
Nice chatting with you Dr. HL.
Dr. Johnny Johnson
LikeLike
We are here to debate fluoridation not semantics, get back on topic, and quit with the personal attacks ( clear enough english for you?)
LikeLike
Social beverage, even the most pro-science person is human. We all get emotional – it’s part of being human.
However, the level of discussion here has been excellent. I have certainly learned a lot. And I have been moderating to stop the usual abuse and sterile copy and paste trolling we get on this subject.
I think the best way for you to contribute is to get stuck into the issues. Don’t worry that some of us are getting a bit emotional.
LikeLike
We are here to debate fluoridation….
What do you mean “we”? I haven’t noticed you debating flouride at all.
Feel free to quote yourself where you got stuck into the debate.
(…crickets chirping…)
Hmm.
You are in the wrong. There was no “red herrring”. There was no “ad hominem”.
Look the terms up. Renounce ignorance.
Google is not your friend.
If I had a dollar for every dill that trolled past this blog bleating about ad hominem when no such thing occured, I’d be rich.
LikeLike
Are there studies published in reputable journals that show there is no correlation between reduced IQ or impaired thyroid function among children and adults exposed to fluoride at levels within the expected daily intake ranges in fluoridated communities?
If the Chinese IQ studies are an anomaly, and contradict a large a body of research that says otherwise, that would be quite reassuring to me. What concerns me is that the only reassurances that I have read seem to rely on the premise that the Chinese studies and the Harvard meta-analysis “don’t prove anything”. I too cringe and roll my eyes when I see some fluoridation opponents saying things like “Harvard study proves fluoride makes us dumb”. This is a perfect example of the type of anti-science rhetoric that is so damaging to the discussion, because certainly the studies do not prove anything. There are a large number of potential confounding variables. However, the fact that something has not been proven harmful is not a substitute for comprehensive research that shows no effect.
Lead is a good example, in the United States at least, of a complete failure of government and science to sufficiently study and respond to the threat of lead based paint and additives. In 2011, just 2 years ago, the CDC cut in half the action level for blood lead levels in children. The level known to cause harm has been slowly coming down for years. In other words, the very same blood lead levels that were believed safe by doctors 20 years ago are now known to cause harm. The League of Nations in 1922 banned lead based paint, but it took the United States until the late 1970s to begin phasing it out. What assurance can the large body of peer reviewed research offer that these questions have been sufficiently studied and answered with respect to fluoride?
LikeLike
Alison, I can’t believe you are unaware of the fallacy you promote by asking for studies showing no correlation of F with ill effects at fluoridation concentrations. The next step is to claim that in the absence of such studies we must assume there are ill effects. This fallacy has been exposed again and again here.
LikeLike
Dr. Limeback is offended with my criticism of his use of a graphic image in a fluoridation political campaign which showed fluoridation to have no effect on caries if there is a year’s delay in tooth eruption caused by the fluoridation. My apologies for a few day delay in responding.
His post contained 9 references he claimed proved his point. His citations follow each with a very short comment.
1. Short EM, 1944
this paper actually found NO difference in eruption if fluoride was below 2.0 ppm
2. Ast DB & Fitzgerald 1960
I could find no reference for 1960
3. Scheinen A 1964
Not in PubMed database
4. Kunzel W 1976
German paper. Full text not available. Ascribed eruption delay to healthier deciduous teeth. Length of delay not stated in abstract.
5. Tseng et al 1989
Found no difference except for premolars which were delayed 2.5-4.5 months with “fluoridation.”
6. Virtanen et al 1994
Study of 911 children with naturally occurring drinking water fluoride. Neither the fluoride level nor the eruption delay time were clear in the abstract.
7. Bigeard L & Obry-Musset MA 1997
A meeting presentation, not in a PubMed indexed journal publication
8. Nadler GL 1998
Orthodontic journal article, The paper did not study a possible relationship between fluoride to eruption.
9. Komarek 2005
This paper uses very complex statistical methods which required 5 days of computer computation time. I am unable to have an opinion as to their statistical methods. They found fluoridation delayed eruption although the length of delay was not clear to my reading. The oldest children were only 12. It is well known that the effect of fluoridation on adult teeth increases with age. At age 17 there is approximately 2.5 times more tooth surfaces saved by fluoridation than at age 12. (Pollick, Int J Env Health 2005:11:2, p 323). They studied the impact of dental fluorosis on delayed eruption, not water fluoridation. Toothpaste and fluoride supplements cause over 90% of the fluorosis (Pendrys 1995). While interesting, it is not directly applicable to the question of community water fluoridation and eruption.
Dr. Limeback, other than Short 1944, makes no references to studies which found no evidence for delayed eruptions. These include:
Carlos JP, Gittelsohn AM. Longitudinal Studies of the Natural History of Caries. I. Eruption Patterns of the Permanent Teeth Journal of Dental Research 1965 44: 509-516
this study included 16,000 children and “Consumption of fluoridated water (1.2 ppm) for varying periods of time had no discernible influence on eruption times or sequence.”
ElBadray, HE, Dental Development in Optimal and Suboptimal Fluoridated communities. J Canadian Dent Assn, 1984, p 761-ff
Children’s dental development in non-fluoridated and fluoridated communities were the same.
Virtanen JI, Bloigu RS, Larmas MA. J Dent. 1996 Jul;24(4):245-50. Effect of early or late eruption of permanent teeth on caries susceptibility.
They found no effect of the eruption times of permanent teeth on caries risk.
It seems particularly egregious for an academic of Dr. Lime back’s stature to cite Virtanen 1994 but not the 1996 study which opposes his thesis.
Leroy R, et al. (2003). The effect of fluorides and caries in primary teeth on permanent tooth emergence. Community Dentistry and Oral Epidemiology 31(6):463-70.
A study of 4468 Flemish children found the effect of fluoride on emergence was “relatively minimal.”
Jolaoso A, Kumar J, et al.
Presentation 2012 National Oral Health Conference – American Association Public Health Dentistry
Does Fluoride In Drinking Water Delay Tooth Eruption?
An analysis of 13,348 children from the 1986-87 National Survey of Oral Health of U.S. School Children found that fluoride in drinking water did not delay the eruption of permanent teeth.
In 2011 an analysis of Paul Connett’s claims about fluoride and delayed eruption was published by the New Zealand National Fluoridation Information Service Advisory. See: http://www.rph.org.nz/content/b418f9b0-12f9-4ab7-a7f3-3d72cbfa424d.cmr
Lastly, Dr. Limeback himself stated in materials submitted to the Juneau, Alaska fluoridation task force that “you can’t explain away the Grand Rapids results with delayed tooth eruption.”
It is possible that given the size of the water fluoridation literature I simply have yet to read of data supporting a one year delay in permanent dentition eruption. It is possible that this can be found in the complete text of a paper to which I have only access to the abstract. I believe what is not possible is that there exists a scientific consensus that community water fluoridation causes a year delay in the eruption of adult dentition to warrant including this in an image designed to convince voters to oppose.
Both Dr. Limeback and Paul Connett have used such images for the purpose of convincing scientifically naive voters to vote “No.”
Particularly because Dr. Limeback was a tenured academic dentist specializing in Preventive Dentistry and must surely be aware of the contradicting literature I stand by my earlier post.
Charles C. Haynie, M.D.; FACS
Hood River, OR
LikeLike
Are there studies published in reputable journals that show there is no correlation between reduced IQ or impaired thyroid function among children and adults exposed to classical music?
Perhaps now the logical fallacy will spring up in front of you.
In other words, the very same blood lead levels that were believed safe by doctors 20 years ago are now known to cause harm.
Think about it.
What did medical researchers do back in the 60’s/70’s?
We don’t have a problem with the dangers of lead-based paints.
None at all.
That’s fine.
What’s different?
Think about it.
LikeLike
Getting into citation competitions and/or waving (cherry picked) studies at opponents of either side of argument won’t change the science.
The consensual position of the science is evaluated by the professional associations and public organisations whose role it is to do so. Done diligently the science will always speak for itself. Such organisations then inform the policy makers and public.
At least, that’s how it is supposed to work.
Events in New Zealand and elsewhere indicate that long running campaigns by those who do not accept the consensual scientific position arising from the scientific literature shortcut this process. They, the antifluoridationists, apply political pressure and cherry picked science outside the scientific consensus directly to public and policy makers.
One question they never answer.
How and why do all the health and scientific authorities get it so wrong?
Never mind waving studies about and debating the weight and merit of each. As a lay person I’m much more interested in the question posited immediately above.
I have to be convinced that all of these authorities have got it wrong. That requires more than endless repetition each side’s favoured literature.
That requires a mechanism for the failure of process.
So, Dr Limeback and others, before you continue further, can you please pause and provide a plausible reason and mechanism for the failure of process.
LikeLike
JDR: And comparing opponents of fluoridation to creationists? C’mon mate
How much time have you got?
I’m fairly sure Cedric will put you right on this.
LikeLike
Ken, I was asking a legitimate question. Are there studies? I thought the answer might be yes. In fact, I assumed there would be studies like this. Are you honestly saying that it’s not important to do any such studies? Surely, there already have been a few done on thyroid and IQ…
LikeLike
Ken, I was asking a legitimate question.
No, you weren’t.
You are indulging in a logical fallacy. That’s not legitimate.
That’s why it’s called a logical fallacy in the first place.
“I can’t believe you are unaware of the fallacy you promote by asking for studies showing no correlation of classical music with ill effects. The next step is to claim that in the absence of such studies we must assume there are ill effects from classical music.”
Can you see now how silly you are being?
Think!
LikeLike
Alison, just change one word in your question.
LikeLike
Alison, you should take Cedric’s warming of fallacies on board.
It is significant that anti-fluoride campaigners have to search the scientific literature in detail, and select papers from often unreliable journals, about studies done in far off countries, and the studies themselves usually of poor quality. This does not mean that there have not been studies done of better quality in other countries. Why should it? So I would expect if one can very rarely find Chinese studies, or Indian studies there would also have been studies done in the West. The thing is that no one is interested in these, and they are very often not published, because they are negative. Fluoride Alert is not going to tell you about such negative studies, are they?
The fallacy of claiming that because no one is reporting the negative effects you seem to want does not mean either that no work has been done or that there must be negative effects we have just not found. Such thinking would lead you to assume all sorts of silly things like salt causes cancer just because no-one has reported salt causes cancer (leading you to conclude that no work has been done and because no one has therefore proved salt does not cause cancer then it must cause cancer).
>
LikeLike
C’mon, guys. Just run the tests to prove that water fluoridation does cause any disorder known on this planet, or any other in the universe, that has ever occurred since the Big Bang, or before………and that will put the question to rest. Why is no one willing to do this? Follow the money…….
Steven D. Slott, DDS
LikeLike
Wow, Ken. Are you suggesting that doing a study to look at the correlation between fluoride intake and IQ or fluoride intake and thyroid function is analogous to calling for a study on whether salt causes cancer?
The funny thing is, Ken, that they do studies on salt and cancer (and the consensus is that salt intake likely plays a role in stomach cancer).
Click to access WJG-15-2204.pdf
Why any scientist would advocate not studying something is perplexing. If asking a simple question about whether or not you’re aware of certain studies is an example of a logical fallacy, so be it. I will do a medline search myself. I was just thinking that you or Steve might already know of some and could provide me with further links. You know that studies still get published and are available in the database even if they do not show an effect. It should be perfectly easy to find out about these studies and I mistakenly assumed that you might have looked.
LikeLike
If asking a simple question about whether or not you’re aware of certain studies is an example of a logical fallacy, so be it.
Are you serious?
Do you think we’re just making this whole logical fallacy thing up just to annoy you?
Look it up for yourself.
Logical fallacies exist.
They often occur in the form of a question. Nothing strange about that.
If you’re makea logical fallacy then…stop.
Stop right now.
Whatever it is that is going on inside your head to justify it.
Stop it
You’re wrong.
Look it up for yourself.
At the moment, you are doing a self-parody.
LikeLike
Alison, requiring proof of a negative is an endless process which is not valid science. It is frequently used as a stalling tactic by antifluoridationists. In order to require proof that there is not a problem, there must first be valid evidence that there is a problem. The 27 Chinese studies which Connett is so fond of citing, do not constitute valid evidence of anything.
However, here is for what you have asked:
“The relationship between duration of exposure to fluoridated public water supplies and measures of child health and behaviour was studied for a birth cohort of Christchurch children. This study showed no association between exposure to fluoridated water and a large range of measures of child health and behaviour taken during the period from birth to seven years, even when the possible effects of family social background were taken into account statistically.”
—–Shannon FT, Fergusson DM, Horwood LJ. Exposure to fluoridated public water supplies and child health and behaviour. N Z Med J 1986;99(803):416-8.
“It is noteworthy in particular that fluoride does not potentiate the consequences of iodine deficiency in populations with a borderline or low iodine intake. Published data failed to support the view that fluoride, in doses recommended for caries prevention, adversely affects the thyroid.”
—Klin Wochenschr. 1984 Jun 15;62(12):564-9.
Fluorine and thyroid gland function: a review of the literature.
Bürgi H, Siebenhüner L, Miloni E.
Steven D. Slott, DDS
LikeLike
Thank you, Steve. As usual, you are the only one to respond with actual science rather than a philosophical argument. Ken and Cedric, I am well aware of the type of logical fallacy you accuse me of “indulging in”. It is often referred to as an “argument from ignorance”. I agree that if there had been no studies done, and I were to point to this as evidence that fluoride has an effect on the developing brain, then I would be guilty of such indulgence. For example, if I were to say, “you can’t prove that it doesn’t lower kids’ IQs” then I would be falling into this logical fallacy. Which is outlined here: http://en.wikipedia.org/wiki/Argument_from_ignorance
However, we do have some evidence of concern. The authors of the Harvard meta-analysis had this to say:
I do not understand how you can read the Harvard analysis, and then read these clarifying statements by the authors, here:
http://www.hsph.harvard.edu/news/features/fluoride-childrens-health-grandjean-choi/
And here:
Click to access Media-Statement_Fluoride-9-12-12-Revised.pdf
Steve and Ken, what has convinced you that these authors are wrong and that a potential link between fluoride and IQ is NOT a research priority? I understand that we cannot draw conclusions from theses studies, but why does the analysis, published and peer-reviewed, not at least establish the issue as a research priority?
LikeLike
Alison, here is what I normally post in regard to Choi and Grandjean. I got tired of writing it out time, after time, after time, so I finally just saved my comment and now paste it. It’s self explanatory.
The Harvard study you reference was actually a review of 27 Chinese studies found in obscure Chinese scientific journals, of the effects of high levels of naturally occurring fluoride in the well water of various Chinese, Mongolian, and Iranian village. The concentration of fluoride in these studies was as high as 11.5 ppm. By the admission of the Harvard researchers, these studies had key information missing, used questionable methodologies, and had inadequate controls for confounding factors. These studies were so seriously flawed that the lead researchers, Anna Choi, and Phillippe Grandjean, were led to issue the following statement in September of 2012:
“–These results do not allow us to make any judgment regarding possible levels of risk at levels of exposure typical for water fluoridation in the U.S. On the other hand, neither can it be concluded that no risk is present. We therefore recommend further research to clarify what role fluoride exposure levels may play in possible adverse effects on brain development, so that future risk assessments can properly take into regard this possible hazard.”
–Anna Choi, research scientist in the Department of Environmental Health at HSPH, lead author, and Philippe Grandjean, adjunct professor of environmental health at HSPH, senior author
As it seems there have been no translations of these studies into English by any reliable, objective source, it is unclear as to whether they had even been peer-reviewed, a basic for credibility of any scientific study. These studies were flawed that NOTHING could be “concluded” from them.
Just to add to this, I now understand that FAN may have paid to have these studies translated. This brings up two questions. First, FAN is not an independent source whom I would trust. Second, if these are the only English translations of these studies, then how did the Harvard Researchers review them? Assuming that Choi could understand them, unless Grandjean and the others are fluent in Chinese, then they would have been solely dependent on Choi’s tranlation and interpretation, which eliminates the whole purpose of having a “team” of reviewers.
There are simply way too many flaws in these studies for them to have any credibility.
Steven D. Slott, DDS
LikeLike
Hi Alison,
The study you cite was recently reviewed by the NZ Medical Council.; Journal of the New Zealand Medical Association, 31-May-2013, Vol 126 No 1375.
In this they heavily slated this study as “… A number of validity issues about the study have been overlooked, disregarded, ignored, or misunderstood”
Please read it, it is a refreshing reminder why we need to sometimes take these studies with a grain of salt.
LikeLike
I understand that we cannot draw conclusions from theses studies, but why does the analysis, published and peer-reviewed, not at least establish the issue as a research priority?
There are these things called P.R.A.T.Ts.
Creationists have their PRATTs.
Climate deniers have theirs.
Anti-fluoridationists have theirs etc.
Alison, here is what I normally post in regard to Choi and Grandjean. I got tired of writing it out time, after time, after time…
Yeah, this.
People like you seem to think that you are the first to ever discover “X” study.
Some nutty website goes “OMG!! OMG!!! OMG!!!” and that settles it for you that it’s really OMG. As in “OMG, this changes everything. How come nothing has been done about this??? Feel the beat of the world revolution!!!”
No.
Science doesn’t work like that.
One single study is worth bugger all.
The study is flawed. It doesn’t say what they told you to think it said.
It never occurred to you to read about the criticisms of that particular study or check out what the actual authors had to say when they realised that the nutters were jumping all over it on the blogosphere.
You continue to cherry-pick isolated studies. Or rather, you meeky cut-and-paste those websites that have cherry-picked the studies for you. A quick google search will reveal that “X” study touted by the loons is famous.
Famous for being used as propoganda by the anit-fluoridationists. Not so famous as an example of good science.
I understand that we cannot draw conclusions from theses studies, but…
Here it comes…
… why does the analysis, published and peer-reviewed, not at least establish the issue as a research priority?
Not that you’re drawing any conclusions or anything.
Sheesh.
Do us all a favour.
Before you breathlessly announce to the world some study or other that has been spoon-fed to you from some dopey blog, how about you do a bit of homework on it?
We do.
Steve and Christopher were very quick off the mark. Neither of them would tell you that what they did in vetting those studies was very hard.
You could have done that yourself.
So it might be a good idea to pre-empt any possible objections and save us all time and embarrassment, yeah?
Make google your friend.
Found an objection?
Then chuck it. Go for another one.
That has an objection too?
No problem. Chuck that too.
Keep going until you come across something that holds water.
LikeLike
Alison
The attempts to associate diminished IQ with fluoridation date back to the very beginnings of the initiative in the 1940’s and early ’50s. It’s an evolution of the paranoia of the ultraconservative John Birch Society and others of like mind who sought to establish fluoridation as a Communist plot to control our minds. It has progressed, through the decades, from that nonsense to the argument of diminished IQ which fluoride opponents such as Connett have sought far and wide to find ANYthing to support this unsubstantiated concept. Digging through obscure Chinese scientific journals to find highly questionable studies of fluoride and IQ is demonstrative of the extent to which they will go to maintain this “sacred cow” of fluoridation effects on the mind.
Steven D. Slott, DDS
LikeLike
One question they never answer.
How and why do all the health and scientific authorities get it so wrong?
Never mind waving studies about and debating the weight and merit of each. As a lay person I’m much more interested in the question posited immediately above.
I have to be convinced that all of these authorities have got it wrong. That requires more than endless repetition each side’s favoured literature.
That requires a mechanism for the failure of process.
Words worth repeating.
Even if you really deeply, truly, madly feel you have found “X” which is oh so OMG! OMG!! OMG!!!….then how come only you and some blogs are jumping up and down about it?
How and why do all the health and scientific authorities get it so wrong?
What’s the mechanism?
LikeLike
Steve, why did the Harvard analysis make it through peer review? Whenever I have questioned a study that you post, your response has been that peer review is the gold standard and that my criticism flies in the face of expert evaluation. I agree that the studies don’t prove anything, but is it your opinion that something must be “proven” to be a research priority? Ate you questioning the integrity and analysis of Philippe Grandjean? Don’t you think that peer review takes into account the exact concerns that you cite in terms of quality control and conflict of interest?
Are you opposed to further research on the issue simply because you worry that it would be a concession to the anti-fluoride group? More research doesn’t exacerbate paranoia, it calms it. Vaccines are a good example. The more research is published addressing public concerns, the more comfortable people feel with vaccines. It is so easy to read the claims that anti-vaccine people make, and then find studies which show that the paranoia is misguided. Why not just do the research?
LikeLike
So much stupid. So little time.
Are you opposed to further research on the issue simply because you worry that it would be a concession to the anti-fluoride group?
Yeah, that must be it.
The more research is published addressing public concerns, the more comfortable people feel with vaccines.
Which is why anti-vaxxer groups don’t exist.
Not.
LikeLike
One problem faced is that outside of water fluoridation political campaigns, many of these issues are seen as unimportant; the biological likelihood of there being a relationship is not sufficient to warrant the funding.
For example here is the European Union SCHER statement: Available human studies do not clearly support the conclusion that fluoride in drinking water impairs children’s neurodevelopment at levels permitted in the EU. A systematic evaluation of the human studies does not suggest a potential thyroid effect at realistic exposures to fluoride. The absence of thyroid effects in rodents after long-term fluoride administration and the much higher sensitivity of rodents to changes in thyroid related endocrinology as compared with humans do not support a role for fluoride induced thyroid perturbations in humans. The limited animal data can also not support the link between fluoride exposure and neurotoxicity at relevant non-toxic doses. SCHER agrees that there is not enough evidence to conclude that fluoride in drinking water at concentrations permitted in the EU may impair the IQ of children. SCHER also agrees that a biological plausibility for the link between fluoridated water and IQ has not been established.?
In the US IQ has been increasing 3 points per decade for at least 50 years. See: Personality and Individual Differences 26 (1999) 381±389. Secular gains in IQ not related to the g factor and inbreeding depression – unlike Black±White differences – A reply to Flynn. J. Philippe Rushton http://psychology.uwo.ca/faculty/rushtonpdfs/PAID-1999.pdf
Improving IQ scores is called the Flynn Effect and has been documented in most industrialized countries. While the concurrent increases in fluoridation penetrance and improving IQ does not disprove neurodevelopmental harm from fluoridation, it is clearly true that progressive IQ improvement has co-existed with large population level fluoride intake increases from the combination of water fluoridation, fluoride containing dental products and supplements.
On the other hand, studies have been funded on matters which are politically significant. Two examples are vaccine preservative thimerisol’s non-relationship to autism and breast prostheses non-relationship to auto-immunne disease. I’ve been arguing for a well designed US study on IQ and fluoridation for quite a few years. It isn’t likely to be done. Firstly there no biological plausibility for an effect. Secondly, designing a study with sufficient statistical power to detect a weak effect of low fluoride exposure increment from fluoridation and to also deal with the many know cofounders of IQ will be very difficult. Certainly there are no current fluoride intake data from which an analysis could be done. Quite clearly such a study would carry a large price tag.
In Portland, Or with great political success fluoridation opponents argued that fluoridation is a clear and present danger to cause disorders of thyroid, pineal, arthritis, bone, cancer, neurodevelopment and other organ systems. Well designed studies on bone fractures, including the demostration that optimal fluoride is associated with fewer fractures has not quieted opponents. Proving that thimerisol does not cause autism did not helped anti-vaccinationists correct their false claims.
Quite sadly, the political discourse which in the US blocks or removes fluoride from drinking water about half the time is largely unresponsive to scientific reality.
As has been pointed out many times in this discussion there is overwhelming unequivocal scientific and professional consensus that fluoridation is beneficial and safe. This consensus is the product of the real debate amongst legitimate scientists.
LikeLike
Thank you, Chuck. That was an excellent explanation. Very helpful and reassuring. It would be wonderful if this type of response could be articulated on a regular basis by the appropriate health professionals. Thank you for taking the time to respond. I’m looking forward to reading a little more from the sources you cite. This is exactly what I was looking for, and assumed there must be someone who could produce an explanation… A scientific response that pointed me to the scientific reasoning and sources, rather than an attack on anyone that asks the question.
LikeLike
Most environmental issues seem to revolve around banning or stopping things. For example, lead was removed from petrol, CFCs removed from refrigerants, people get concerned about small amounts of chemicals used in fracking, and so on.
All these issues have resulted in these industries beign curtailed or regulated.
Water fluoridation is the opposite. We artificially add fluoride to water to solve the supposed problem of tooth decay.
It is incumbent on those doing this to the water to show that it is an effective, safe, and economically sound process.
It is not incumbent on the “anti” group to prove that fluoridation is dangerous, or undesirable for some other reason. The “pro” group are changing the chemical makeup of the water supply. It is entirely their responsibilty to justify the process, and science can only play an advisory role in this.
LikeLike
Alison, I was waiting for you to raise the peer-review question. You didn’t disappoint. Yes, I consider peer-review to be critical for credibility of scientific study, and I take it very seriously. However, that doesn’t preclude me, or anyone else, from questioning the validity of a study. It’s simply a matter of how my arguments against the validity stack up against the reader’s opinion of the validity of the peer-review. People will have to make their own assessment on that.
In this case, although the Harvard Review itself was peer-reviewed, as I said, it is questionable whether any of the 27 studies themselves had been peer-reviewed. Choi and Grandjean admitted that the methodologies of these studies were questionable, which is one parameter assessed by review. I personally question how this Harvard Review even made it through peer-review, and yes, I absolutely am questioning the integrity and analysis of Phillippe Grandjean. They originally dug up 37 such studies. Ten were so seriously flawed that even they rejected them as not being sufficiently valid for review. Given the flaws of the rest of them, it is questionable why they didn’t reject them, as well.
I put my arguments, my support for those arguments, and my opinion about the Harvard Review up against the fact that it was peer-reviewed. Readers are free to weigh that any way they wish. You are certainly free to put your arguments and opinions up against any peer-reviewed article, as well.
Finally, no, I am certainly not against further study of any scientific issue. Just the opposite. What I am against is the endless use of unsubstantiated claims to demand an infinitive amount of testing, using that as an excuse to cease, or not begin a valuable public health initiative as water fluoridation.
Steven D. Slott, DDS
LikeLike
Janet
The “supposed problem” of tooth decay? Are you seriously that out of touch with reality that you consider the worldwide, overwhelming amount of rampant, untreated dental disease, to be a “supposed problem”?
Do I really need to post for you, yet once again, a list of peer-reviewed scientific studies that clearly demonstrate the effectiveness of water fluoridation? Do I really need to ask you yet once again to provide valid evidence of ANY adverse effects of water fluoridation? Do I really need to state, yet once again, that at $1 per person per year, there IS no other more cost effective measure that reaches the numbers of people and delivers the amount of dental decay protection as does water fluoridation?
Lastly, adding a miniscule few more parts per million of a fluoride ion identical to that fluoride ion which already exists in water, changes the chemical composition of that water……..how?
Water fluoridation is safe and effective. If you have valid evidence to the contrary, provide it. Otherwise, your statements and claims continue to be entirely meaningless.
Steven D. Slott, DDS
LikeLike
I’m sorry Steven, you didn’t understand my point.
LikeLike
Janet, you never have a valid point to understand. Just your unsubstantiated opinions.
Steven D. Slott, DDS
LikeLike
Steve
Tooth decay is a problem in some communities but fluoridation is not the solution.
Do you have the details of one high-quality scientific study to support the safety and efficacy of adding fluoride to drinking water?
“Lastly, adding a miniscule few more parts per million of a fluoride ion identical to that fluoride ion which already exists in water, changes the chemical composition of that water……..how?”
Where does one buy these fluoride ions that you believe we should be force-fed via the water supplies we pay good money for?
Robert Brentwood
LikeLike
Robert
1. What qualifications do you have to make the assessment that “fluoridation is not the solution”?
2. At the end of this comment is listed 5 high quality, peer-reviewed scientific studies which clearly demonstrate the effectiveness of water fluoridation. Let me know if you would like more. As far as safety, it is not valid to demand proof of safety of a substance without valid evidence of its non-safety. Provide valid evidence of a problem with water fluoridated at 0.7 ppm and I will gladly address that with you.
3. One doesn’t “buy” fluoride ions, and nothing is force-fed to anyone in regard to fluoridated water. The vast majority of fluoridated water systems are done so by the addition of hydrofluorosilic acid (HFA). HFA is derived from naturally occurring phosphorite rock as a co-product of the process used to derive the other co-product, phosphoric acid. At the pH of drinking water, HFA is immediately and completely dissociated into fluoride ions identical to those which exist in eater “naturally” and trace contaminants in miniscule concentrations far below the EPA mandated maximum levels of safety. After that point, HFA no longer exists in that water. It is thus not ingested, and is of no concern. Fluoride ions and harmless, trace contaminants are the only substances ingested as a result of water fluoridation.
Efficacy studies:
1). http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2925001/
Results
Children from every age group had greater caries prevalence and more caries experience in areas with negligible fluoride concentrations in the water (<0.3 parts per million [ppm]) than in optimally fluoridated areas (≥0.7 ppm). Controlling for child age, residential location, and SES, deciduous and permanent caries experience was 28.7% and 31.6% higher, respectively, in low-fluoride areas compared with optimally fluoridated areas. The odds ratios for higher caries prevalence in areas with negligible fluoride compared with optimal fluoride were 1.34 (95% confidence interval [CI] 1.29, 1.39) and 1.24 (95% CI 1.21, 1.28) in the deciduous and permanent dentitions, respectively.
——Community Effectiveness of Public Water Fluoridation in Reducing Children's Dental Disease
Jason Mathew Armfield, PhD
2) http://www.ncbi.nlm.nih.gov/pubmed/23550501
CONCLUSIONS:
Children with severe dental caries had statistically significantly lower numbers of lesions if they lived in a fluoridated area. The lower treatment need in such high-risk children has important implications for publicly-funded dental care.
——Community Dent Health. 2013 Mar;30(1):15-8.
Fluoridation and dental caries severity in young children treated under general anaesthesia: an analysis of treatment records in a 10-year case series.
Kamel MS, Thomson WM, Drummond BK.
Source
Department of Oral Sciences, Sir John Walsh Research Institute, School of Dentistry, The University of Otago, Dunedin, New Zealand.
3). http://www.ncbi.nlm.nih.gov/pubmed/23488212
CONCLUSIONS:
The survey provides further evidence of the effectiveness in reducing dental caries experience up to 16 years of age. The extra intricacies involved in using the Percentage Lifetime Exposure method did not provide much more information when compared to the simpler Estimated Fluoridation Status method.
—–Community Dent Health. 2012 Dec;29(4):293-6.
Caries status in 16 year-olds with varying exposure to water fluoridation in Ireland.
Mullen J, McGaffin J, Farvardin N, Brightman S, Haire C, Freeman R.
Source
Health Service Executive, Sligo, Republic of Ireland. joej.mullen@hse.ie
4) http://www.ncbi.nlm.nih.gov/pubmed/8500120
Abstract
The effectiveness of fluoridation has been documented by observational and interventional studies for over 50 years. Data are available from 113 studies in 23 countries. The modal reduction in DMFT values for primary teeth was 40-49% and 50-59% for permanent teeth. The pattern of caries now occurring in fluoride and low-fluoride areas in 15- to 16-year-old children illustrates the impact of water fluoridation on first and second molars.
—-Caries Res. 1993;27 Suppl 1:2-8.
Efficacy of preventive agents for dental caries. Systemic fluorides: water fluoridation.
Murray JJ.
Source
Department of Child Dental Health, Dental School, University of Newcastle upon Tyne, UK.
5). http://www.ncbi.nlm.nih.gov/pubmed/23252588
CONCLUSIONS:
Data showed a significant decrease in dental caries across the entire country, with an average reduction of 25% occurring every 5 years. General trends indicated that a reduction in DMFT index values occurred over time, that a further reduction in DMFT index values occurred when a municipality fluoridated its water supply, and mean DMFT index values were lower in larger than in smaller municipalities.
—-Int Dent J. 2012 Dec;62(6):308-14. doi: 10.1111/j.1875-595x.2012.00124.x.
Decline in dental caries among 12-year-old children in Brazil, 1980-2005.
Lauris JR, da Silva Bastos R, de Magalhaes Bastos JR.
Source
Department of Paediatric Dentistry, University of São Paulo, Bauru, São Paulo, Brazil. jrlauris@fob.usp.br
Steven D.Slott, DDS.
LikeLike
Steve Slott | November 12, 2013 at 10:08 am |
Janet, you never have a valid point to understand. Just your unsubstantiated opinions.
Steven D. Slott, DDS
My unsubstantiated opinions are not on the merits or otherwise of water fluoridation and its effects on dental health. I was not intending to make any value judgement on the benefits or otherwise of the process.
My point was relating to the nature of the problem compared to other environmental and health issues.
I was making the point that in most other environmental and health issues, various processes become regulated or banned. What you are doing in this debate is inverting the position of the pro- and anti- flurodationists.
I could, for example, make the claim that the small amount of chemicals use in hyraulic fracturing for shale gas is harmless (true, in my opinion) and that anyone who disagrees with me is an anti-science flat-earther.
These statements are no very helpful in furthering discussion on the topic at hand.
LikeLike
There is a basic problem with your assumptions, Janet. You are seeing fluoride as an environmental or health problem akin to something like lead. When if fact F plays a beneficial role at low concentrations. But like a lot of beneficial elements it can also be toxic at high concentrations.
This does raise the question of regulation – both to prevent excess but also to overcome deficiency. But unlike lead it does not mean banning. We don’t ban selenium or iodine, do we? But we regulate them.
I don’t know where people get these flat earther accusations from.
>
LikeLike
Janet, certainly you may make whatever philosophical points you wish to make about any issue you wish. I prefer to stick with accurate facts on water fluoridation which are supported by valid, peer-reviewed science.
Steven D. Slott, DDS
LikeLike
There is a basic problem with your assumptions, Janet. You are seeing fluoride as an environmental or health problem akin to something like lead
No, I am not
LikeLike
A brief comment about peer review and the claim it is a gold standard. I do get annoyed at the way both sides use the “peer review” description as an argument.
Peer review, in the very limited sense of reviewing submitted papers before publication is a very human process. It can be good, it can be bad. It can be shocking or practically non-existent (or existent in name only for some journals). It’s often said that it is a hopeless process but way ahead of the alternatives – like democracy.
Certainly many scientists do acknowledge problems and look for alternatives.
Having often been on both sides (reviewer and author) I have seen it warts and all. My advice is don’t use it as your only yard stick. The scientific literature should always be approached intelligently and critically. If we do so we can see that the so-called Harvard study is really useless despite being “peer reviewed.”
My concept of proper scientific peer review is that it is the constant ongoing processes scientific work gets subjected to by one’s peers. At the proposal level, at the experimental level, at the seminar and institutional review level, at the publication level and at the post publication level.
The criticism that the so-called Harvard meta-study currently gets is just peer review at the post publication level. The intelligent and critical assessment of the published work.
I wish people would provide reasons for using quoted papers, showing an intelligent and critical assessment of them, and not just say they are “peer reviewed” and therefor unquestionable.
LikeLike
Janet: I was making the point that in most other environmental and health issues, various processes become regulated or banned.
Fluoridation is already well regulated.
Whatever point you are trying to make immediately evaporates.
LikeLike
If Fluoridation of water is universally accepted as a good thing, why does only 5% of the world fluoridate their water?
LikeLike
Janet, fluoridation is not universally accepted “as a good thing.” But all international health authorities accept that fluoride is beneficial for oral health.
Fluoridation of public water supplies is more a political or technical question than a scientific one. In a couple of countries it is opposed on grounds of “freedom of choice.” But there are many other reasons – decisions to fluoridate salt or milk, unsuitable water supply systems, cultural questions like preference for bottled water and high or adequate natural levels of f in the water supply.
The argument that we should not do it because some others don’t is simplistic and inadequate.
>
LikeLike
Fluoridation of public water supplies is more a political or technical question than a scientific one
Yet Steven Stott only wants to discuss peer reviewed studies. Do these peer reviewed studies have any analysis of political or technical issues?
If it is more a political and technical issue than scientific, then why are some of your commenters comparing people who are opposed to bulk fluoridation of water as “anti-science”, and akin to creationists?
Maybe they are opposed because of the political, technical, or cultural issues that you admit may be more important than the scientific ones?
LikeLike
Janet, I criticise anti-science attitude because they either represent an attack on science and scientists or because they misrepresent the science. In many ways this is similar to what creationists do.
However, no-one is using those terms to describe people opposed to fluoridation of water supplies. Really that only comes up when the scientific issues get discussed and the distortions and misinformation starts.
People can have a variety of reasons to oppose fluoridation. Often they will declare simply a freedom of choice argument. That is OK by me (although I many not have the same values or political outlook as them). But when the so-called values reasons start disappearing and science get distorted then that is not OK by me.
LikeLike
Fluoridation of public water supplies is more a political or technical question than a scientific one
I agree this seems odd, I’d say the statement should have made clear it is premised on the fact that the science is effectively settled in regard to the fluoridation mechanism and health benefit/potential harm.
I’n not presuming to answer for Ken.
LikeLike
Ken, I agree with you about peer-review. It is not infallible by any means. However, it does set a baseline standard of credibility. There is so much garbage put out by fluoride opponents that there must some standard from which to begin proper assessment. Take Declan Waugh’s paper for example. For a pretty good while, fluoride opponents were posting links to it and touting it as credible evidence of all the disorders they claim. The baseline was that it had not even been peer-reviewed, the mechanism utilized by mainstream science to assure, as well as possible, basic credibility of published works. It was also discredited by his own Irish government, but the lack of peer-review meant it did not rise to any real level of credibility in the first place.
My criticism of Connett’s book is that he wants it both ways. He constantly attempts to steer people to it as validation of his claims, as if it is scientifically authorative, while on the other hand, there has been no proper review of it to at least offer some assurance that he has used his cited references accurately, appropriately, in the proper context, or even at all. Readers are simply expected to take his word that he has done so.
Conversely, when studies are presented as having been peer-reviewed, it sets the bar much higher in terms of arguing against their validity. It does not mean that the argument cannot be made, but that it takes far more than just unsubstantiated opinion to overcome the basic credibility established by peer-review. Thus my statement about weighing my opinion against the fact that Harvard had been peer-reviewed. Whether or not my arguments and opinions overcome the bar set by peer-review is simply left up to readers to decide.
Fluoride opponents have, for far too long, been utilizing invalid claims based on invalid literature, to make their case. Requiring peer-review simply holds their feet to the fire in terms of weeding out the mounds of total nonsense, and making them provide more credible evidence than just citing “fluoridealert.org”.
Steven D. Slott, DDS
LikeLike
Yes, but also specific decisions about fluoridating water will depend on the technical aspects – it is just not suitable in some situations. It will also depend on the political acceptance of the community – the attitudes may well be quite unscientific but nevertheless real.
LikeLike
Janet the argument about “5% of the world” is exactly the point about requiring peer-reviewed science. The reasons other countries do not fluoridate is, more often than not, presented by fluoride opponents as being due to “concern for health risks”. If this is allowed to stand without requesting valid, accepted evidence of its validity, then readers are left with the misleading, unwarranted perception that the “rest of the world” is somehow much more astute than is the United States, and more on top of the “risks” of water fluoridation. Challenging this statement with requests for valid peer-reviewed, or other validly documented evidence to support it, exposes the flaw in attempts to imply that the “rest of the world” knows what it is doing far better than the US.
Science and healthcare are evidence based, not unsubstantiated opinion based. Peer-review sets a baseline to weed out unsubstantiated claims and refocus attention to facts which are supported by valid science.
Steven D. Slott, DDS
LikeLike
Agreed, Ken. As long as the unscientific attitudes are not presented as valid science, I have no problem with them, and respect the rights of people to have them. When these attitudes are presented as “the science that supports their position” is when I have the problem. That’s when I request peer-reviewed evidence.
Steven D. Slott, DDS
LikeLike
When these attitudes are presented as “the science that supports their position” is when I have the problem.
There are many examples of science that supports a particular position being promoted by NGOs and governments. Perhaps this also applies to Fluoridation?
I don’t have the answers to this, but I get suspicious when science is presented as settled, 100% correct and of asbolutely no question.
Not that long ago (1950s), women were given hysterectomies for suffering from “hysteria” (hence the name) which has since been identified as sexual frustration.
This was settled science back then. A sexually frustrated woman had her womb surgically removed.
LikeLike
If I could just make an observation, Janet. I regard peer-review as a bare minimum standard for evidence. Not as a gold standard.
For all its flaws, peer-review does indicate that a paper has been checked over for flaws or problems by people knowledgeable in the field. This is not a guarantee that there are no flaws present (as has been noted, it is a human process, subject to errors), and indeed I’m sure a few of us could point to severely flawed papers which should never have passed peer-review. Consequently, peer-reviewed papers are not immune to critical assessment.
However, if a paper never passed peer-review in the first place, this is a pretty good indicator that the reviewers found substantial flaws in it. Often, if scientists encounter such a paper, it’s pretty straightforward to identify what those flaws were, whether they were problems with the methodology or unwarranted conclusions being drawn from the evidence.
Hence why, when people discuss evidence on any particular topic, they ask for peer-reviewed papers as an initial filtering mechanism. An imperfect system of review still beats no review at all.
LikeLike
Janet, science is ever changing. To ignore the infinite amount of times that the consensus of mainstream science has gotten it right, in lieu of the relatively few times it did not, is to ignore where we are today. We do not have the unbelievable advances we have in science, healthcare, and technology because mainstream science got it wrong the majority of time.
To ignore the overwhelming consensus of respected science and healthcare, on the issue of water fluoridation, is to accept the opinions of the relatively few, vocal activists who haven’t the qualifications to make proper healthcare recommendations. Whom do you believe is more apt to get it right, mainstream science and healthcare, or unqualified activists? There are no guarantees with anything. It just boils down to where you want to place your trust.
Steven D. Slott, DDS
LikeLike
Steve
1. I’m human being who believes he has the right to refuse consent to what is I believe fluoridation is i.e. medication. Apart from a DDS, what qualifications do you have? Are you a scientist?
2. Are the studies to which you refer Randomized Controlled Trials?
3. So, everyone around the world is drinking fluoridated water has given their individual, informed consent have they? Medication should always be undertaken with pharmaceutical grade chemicals with individual, informed consent.
Are any of the studies you cite for efficacy Randomized Controlled Trials?
Robert Brentwood
LikeLike
Steve
“Whom do you believe is more apt to get it right, mainstream science and healthcare, or unqualified activists?”
In the 17th century, Galileo challenged the Church of Rome’s geocentric view of our solar system with the Copernican heliocentric view. Who would have sided with? Galileo, the activist, or the papacy, the self-appointed authority on matters celestial?
Robert Brentwood
LikeLike
Robert
Believe what you wish. However, fluoride at 0,7 ppm is not “medication”, and it is not forced upon anyone. Fluoride is a mineral which the FDA must classify as a drug for the sole reason of its stated use in water as a therapeutic rather than as a disinfectant. No other reason. As the EPA regulates all mineral additives to water, it is the EPA, not the FDA, which controls and regulates fluoride in water. Fluoridated water meets all NSF Standard 60 certification requirements as mandated by the EPA. There are no dosage requirements for fluoride, nor is there any need for such, any more than is there any need of dosage requirements of chlorine in water. The “forced medication” gambit has been repeatedly attempted by antifluoridationists in courts. It has been rejected each and every time by those courts.
I am a dental healthcare professional who is commenting on a dental/healthcare issue. Equally as important, if not moreso, I can and do cite valid scientific evidence to support my statements and claims.
Your call for “randomized controlled trials” is the standard antifluoridationist argument copy/pasted off of antifluoridationist websites. The reality is that RCTs are nearly impossible for water fluoridation due to halo effect and difficulty in adequately segregating fluoridated groups from non-fluoridated for the purpose of study. Water fluoridation is a public health initiative. As with all such initiatives fluoridation is measured by its effect on the entire population to which it is exposed. Therefore, observational studies of the effect on the entire population are not only entirely acceptable, but preferable for this purpose. The studies I have presented are high quality, peer-reviewed. I will gladly provide you with more if you so desire.
Steven D. Slott, DDS
LikeLike
I am not making any claims with regard to water fluoridation. I am looking at the bigger picture of the role of science in public decision making
LikeLike
Ah,the Galileo gambit, Robert. It is amazing how many people pull that rabbit out of the hat when they don’t have the science.
The difference here is that Galileo did have the science and argued for it (although gave in at the end). His argument for relying on evidence and reason rather than scripture and authority was fundamental to the scientific revolution.
That is quite different to many forms of activism today, especially the anti-fluoride activism. Often these people ridicule the science, the evidence and reasons. They argue from authority (as did the church), they cherry pick and misrepresent.
Activism has its place but always has the risk of emotive confirmation bias and promotion of misinformation in the interests of strongly held ideological beliefs.
>
LikeLike
Robert
Sure, there are times when mainstream science has been challenged and found to be wrong. That’s one of the ways which science progresses. If you want to equate antifluoridationists with Galileo that certainly is your prerogative. I prefer to trust the overwhelming consensus of respected science and healthcare on this issue.
Steven D. Slott, DDS
LikeLike
Journal’s editorial peer review has a very large range of quality and validity. A nice explanation of this is this YouTube video:
It is my opinion that many of the journals with the word environment in their title fall short of what we expect for medical journals. For example, William Hirzy, a lifelong politically active fluoridation opponent published this paper:
Reference: Hirzy JW, Carton RJ, Bonanni CD, Montanero CM, Michael F, Nagle MF. 2013. Comparison of hydrofluorosilicic acid and pharmaceutical sodium fluoride as fluoridating agents – A cost – benefit analysis. Environmental Science & Policy 29: 81-86 (May).
Hirzy then petitioned the EPA to require pharmaceutical grade NaF be used for water fluoridation. Analysis by EPA scientists showed Hirzy made a calculation mistake which invalidated his conclusions. Other important errors were overlooked by the journal’s review such as not using the known threshold concentration for arsenic carcinogenicity and the inconsequentially small arsenic dietary increment from fluoridation.
So while a paper may appear in a PubMed indexed journal, that certainly is no guarantee of quality information.
LikeLike
It sounds a bit like the “overwhelming” evidence for dangerous global climate change that is disputed by many scientists.
LikeLike
Janet, the evidence for climate change and our contribution to it is really overwhelming. Very few scientists would dispute that it is happening – even the climate “sceptics” who these day agree it is happening and only argue about the quantitative aspects.
>
LikeLike
Thanks . . glad that was helpful.
LikeLike
Janet, the evidence for climate change and our contribution to it is really overwhelming
I said the evidence for dangerous climate change. I guess you didn’t read that bit, or like to play with words. Maybe the evidence that Fluoride is 100% safe is not so strong then.
LikeLike
It sounds a bit like the “overwhelming” evidence for dangerous global climate change that is disputed by many scientists.
A new chew toy for Cedric.
LikeLike
Steve
Therapeutic? Medicine!
Your a dentist who can’t cite any RCTs.
Didn’t you do some cutting and pasting above?
I believe the halo effect to which you refer can be accounted for in an RCT.
Observational studies are totally unacceptable for subjecting hundreds of millions of people to medication through their water supplies. Without RCTs, your claims of efficacy for fluoridation are meaningless.
Robert Brentwood
LikeLike
Observational studies are totally unacceptable for subjecting hundreds of millions of people to medication through their water supplies. Without RCTs, your claims of efficacy for fluoridation are meaningless.
Eppur si muove
LikeLike
A new chew toy for Cedric.
Is Cedric your dog?
LikeLike
Alison, Steve
I think also it is important to remember that meta-analyses of the very highest quality of studies, randomized blinded trials, are in error compared to the eventually completed definitive analysis over 1/3 of the time
See:
Discrepancies between Meta-Analyses and Subsequent Large Randomized, Controlled Trials. Jacques LeLorier, M.D., Ph.D., Geneviève Grégoire, M.D., Abdeltif Benhaddad, M.D., Julie Lapierre, M.D., and François Derderian, M.Sc. N Engl J Med 1997; 337:536-542 August 21, 1997
The Harvard researchers said: “each of the articles reviewed had deficiencies, in some cases rather serious, which limit the conclusions that can be drawn.” Meta analysis will not rescue a conclusion from poor studies.
The authors said the difference in IQ was small and within the measurement error for IQ testing.
The average fluoride concentration of the control or low-fluoride groups — the ones who may have slightly higher IQs — was about 0.7ppm. The meta analysis conclusion is really that fluoridation is neurodevelopmentally safer than high fluoride.
A full 20% did not even study drinking water, rather environmental pollution from fluoride.
Only one of the Chinese studies compared high, low & optimal fluoride levels. It found IQ was lower at both high & low fluoride drinking water.
Quoting the study which found fluoridation best for IQ: “By testing of the intellectual ability of 447 elementary school students ranging in age from 9 to 10 1/2, it was discovered that both high and low fluoride had an effect on child intelligence. Fluoride levels greater than 2.0 mg/L or less than 0.2 mg/L can disrupt intellectual development.”
SOURCE: Qin LS, Cui SY. (1990). The influence of drinking water fluoride on pupils IQ, as measured by Rui Wen’s standards. Chinese Journal of the Control of Endemic Diseases 5:203-204.
A similar case exists with respect to bone health. The fewest fractures occur when fluoride ion concentrations is optimized. Very low fluoride is associated with as many fractures as is concentrations two times higher than what the EPA allows as safe in drinking water.
Li’s study has been generally recognized as very well done. In an article coauthored by the antifluoridationist dental professor Hardy Limeback, the Li paper was judged conclusive.
Li and Qin thus show that fluoridation, compared to both low and high fluoride is associated with fewer fractures and better IQ.
LikeLike
Is Cedric your dog?
Stick around. You’ll be meeting Cedric presently.
LikeLike
Ken
I don’t need to cite any science as I’m not trying to mass-medicate anyone.
Robert Brentwood
LikeLike
Ken
Hasn’t the earth’s climate always changed? Aren’t you referring to global warming? Oop’s, the earth’s now cooling. Er, let’s change global warming to climate change, quick! Has anyone noticed? Yes!.
Wasn’t warming detected on Mars about fifteen years ago? Martian’s must therefore exist and are influencing their atmosphere.
Robert Brentwood
LikeLike
Hasn’t the earth’s climate always changed? …Oop’s, the earth’s now cooling….blah blah blah
It’s wholly predictable. In they fly, right on cue, like moths to a flame.
AGW deniers, anti-vaxers, anti-fluoridationists, creationists etc,.
Science deniers. Peas in a pod.
LikeLike
Hi Robert,
“I don’t need to cite any science as I’m not trying to mass-medicate anyone.”
I’m confused…so how do you back up (scientific) claims you make?
Or do you not make claims?
LikeLike
Hey Alison,
Have you managed to have a look at the citation I gave re: the critique of the Chinese IQ study?
What do you think?
LikeLike
Janet, “dangerous” is a subjective term – but nevertheless we can certainly use it with climate issues as any Philippino will probably tell you today. Aomwhomis playing with words?
As for Cedric – he could be described as a Rottweiler.
LikeLike
Part of the political discussion of fluoridation must concern social justice.
One of the most compelling benefits of community water fluoridation’s (CWF) effectiveness is prevention of about 2/3rds of the operations for terrible cavities in preschool children.
The graph of data from New South Wales can be viewed here:
http://photos.oregonlive.com/photogallery/2013/09/far_fewer_operations_w_fluorid.html
These under anesthesia procedures include extractions root canals & stainless steel crowns & in the US cost up to $15,000. Clearly they happen more often in Australian communities without CWF.
In addition to Australia, this remarkable benefit has been confirmed in Texas, New York, Scotland and Oregon.
The largest study is from Louisiana – see: Water Fluoridation & Costs of Medicaid Treatment for Dental Decay. MMWR. CDC 09/03/1999
In addition to avoiding 2/3rds of these operations, in Louisiana 50% of the dental bills for the kids studied are avoided.
If this were the only benefit 150% CWF returns in lower dental bills
see: Prev Chronic Dis. 2012 Mar;9: A simulation model for designing effective interventions in early childhood caries. Hirsch GB, et al
It is my bet that few public health programs Australia might undertake will have a return on investment of even 150%. That number doesn’t include the saving for dental care of permanent teeth estimated by the CDC to be $38 for every $1 invested.
This is an important Social Justice issue. While fluoridation is not a silver bullet cure, it blunts the poor oral health burden those with socioeconomic disadvantage, especially disadvantaged children.
We all need to worry more about caring for society’s vulnerable members and less worrying over theoretic and unproven harms.
Save for those blinded by the passion of their opposing beliefs, supporting community water fluoridation is an easy decision.
LikeLike
Modern science is open. The half life of baloney is pretty short. Community water fluoridation has been and continues daily to be debated and discussed amongst professionals young and old, and it is clear that the overwhelming expert consensus is that oral health is thereby improved.
“Ruthlessness towards mistakes has always been one of the engines of scientific enterprise” – G. Farmelo in “To Err is Human” New Scientist, 28, Nov 1998
There are profound philosophical reasons that expert consensus is the very best, even all we have, as an anchor to reality in matters like fluoridation.
You may find errors in past science, but that those errors were corrected should give confidence not skepticism to the easily verified fact that the overwhelming professional and scientific consensus is that community water fluoridation is beneficial and safe.
LikeLike
Dr. Haynie (first post): “I am unaware of any study ever done showing a full year’s difference in eruption due to fluoridation. This claim is a fabrication.”
Me: I presented them. I was simply responding to the accusation it was a ‘lie’ (fabrication).
Dr. Haynie (second post): Now acknowledges them. He cant find all of them so is he questioning that they exist?
He doesn’t understand the stats in the Komarek study and doesn’t think they corrected for tooth eruption and claims they failed to find a benefit of fluoridation when eruption timing was corrected. The paper showed what it says it showed: that after correcting for emergence times (eruption times) the effects of fluoride on caries were not seen.
He says that I was leaving out studies that failed to show the fluoridation effect on tooth eruption. I never denied they existed.
I know about them. They aren’t good studies. Neither are the ones I listed. However, Dr. Haynie said the delayed eruption effect was a ‘fabrication’.
If we want to do a thorough search of ALL the papers (including the animal studies……we should NOT leave those out), and do a quality assessment analysis of all of them, this comment section is going to be very long. Use ‘fluoridation’ for a search word in PubMed, you get over 6000 hits. Want me to comment on all of them here?
I acknowledge there are difficulties in designing clinical studies in this area. In fact I did a study to look at pre- and post fluoride effects on tooth eruption. (using the Burlington Growth Study orthodontic records of hundreds of children that grew up pre-fluoride (1960s). The effects were not only profound on tooth eruption but also on skeletal development (I used the hand radiographs on file to look at matacarpal phalangeal mineralization- which is used to estimate skeletal age). I presented that study at an IADR meeting. Publishing was a different story. One reviewer claimed it could have been the effect of growth hormones in chickens introduced at about the same time into the food supply as fluoride through fluoridation (I would never have thought to control for THAT!). Critics made all kinds of excuses why the study could not be published. It was a good study….but flawed. Just like most others of the same kind (except the Komarek study)
Dr. Haynie (Second post): “Lastly, Dr. Limeback himself stated in materials submitted to the Juneau, Alaska fluoridation task force that “you can’t explain away the Grand Rapids results with delayed tooth eruption.”
Response: Grand Rapids was 1945- 68 years ago. It was the end of WWII. Caries rates were so high in the US they couldn’t send soldiers to fight in Europe suffering from painful abscesses. It’s one of the reasons a branch of the NIH was formed (NIDR,,,now NIDCR, after my friend Hal Slavkin convinced Congress that craniofacial research was important to support.) Up until the 60’s the the IADR spent tons of money on researchers who wanted to show the benefits of fluoride. Fluoridation schemes, fluoride supplement programs, school rinse programs, professional fluorides. The makers of OTC fluoride toothpastes and mouthwashes basically funded their own research but donated a lot of money to IADR research (scholarships, grants etc.) Fluoride was the IADR’s pride and joy. Caries declined radically over the decades since Grand Rapids and there were many reasons: better hygiene, improved nutrition, Vitamin D in milk, better access to dentists, preventive education and successful marketing of fluoridated toothpaste etc. Eventually the difference between fluoridated and non-fluoridated cities was so small it could no longer be measured. I can provide a list of MODERN studies to support this.
Dr. Haynie used the term ‘egregious’ referring to my presentation of diagrams and ‘omission’ of studies. Was that really ‘outstandingly bad’?
People need to know that there is NOT overwhelming evidence that fluoridation is ‘safe and effective’. There are no double blinded RCT and the cross-sectional ecologic studies on fluoridation effectiveness did not examine all the potential side effects. Actually, the early experiments such as the Grand rapids one, where the ONLY source of extra fluoride was from the water, there were changes from fluoridation that were documented (earlier menses, boney exostoses, or benign bone tumours), but of course these were ignored.
The policy makers advising city council without doing due diligence by reading every single available study (as we did over 3.5 years on the NRC committee) are the ones who are ‘outstandingly bad’ (egregious).
Why use terms like egregious? That’s just throwing gasoline on the fire. It’s not helpful.
LikeLike
People need to know that there is NOT overwhelming evidence that fluoridation is ‘safe and effective’.
Well the overwhelming judgment of essentially every public health and scientific organisation on the planet say otherwise.
Until you provide a plausible reason, and mechanism, as to how they all got it so wrong I have no good reason to accept you word over theirs.
LikeLike
Antifluoridationist’s call for randomized studies is a classic straw man argument. Firstly, if one were done they would still just as aggressively oppose on the basis of their “mass medication” pseudo argument.
A randomized double blind study ostensibly to “prove” that drinking water fluoride prevents cavities would be found unethical by every Independent Review Board world wide.
Studies on fluoridation simply cannot be designed as randomized clinical trials. Random allocation of study subjects is not possible when a community begins to fluoridate the water because all residents in a community have access to and are exposed to this source of fluoride. In addition, clinical studies cannot be conducted double-blind because both study subjects and researchers usually know whether a community’s water has been fluoridated.
Outside of anti-fluoridation political rhetoric there are no calls for randomized studies of fluoridation’s effectiveness.
That there are no randomized studies is counterbalanced by the existence of similar results from numerous well-conducted field studies by many scientists of thousands of persons throughout the world.
You might read this regarding the advantage observations studies which include real-world complexity which is missing with randomized trial.
Silverman SL.
Am J Med. 2009 Feb;122(2):114-20.
From randomized controlled trials to observational studies.
One of the most compelling observations studies is the huge Louisiana Medicaid study which showed that 2/3rds of the operations for mouth fulls of rotten baby teeth are avoided with fluoridation. This has been confirmed in Australia, New York, Texas, Scotland and Oregon.
Water Fluoridation and Costs of Medicaid Treatment for Dental Decay — Louisiana, 1995-1996. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention September 03, 1999 / 48(34);753-757
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4834a2.htm
We have over 68 years of large population fluoridation experience. The US National Library of Medicine’s database has about 6,000 papers on fluoridation and over 40,000 papers which reference fluoride. There is an enormous knowledge base upon which to confidently believe that fluoridation is beneficial and safe.
LikeLike
Does anyone know the cost (in dollars) of Fluoridating water, and the related savings in dental care?
Apologies if this has been already covered
LikeLike
Some figures from Hamilton NZ. The fluoridation costs (to the council) was NZ$48,000 per year. The estimated cost of the extra dental work (to the taxpayer) on stopping fluoridation is NZ500,000 per year. Money that isn’t budgeted for which probably means decreased service in other areas.
LikeLike
I don’t have the answers to this, but I get suspicious when science is presented as settled, 100% correct and of asbolutely no question.
Not that long ago (1950s), women were given hysterectomies…
Claim CC001:
“In 1912, Charles Dawson and Arthur Smith Woodward announced the discovery of a mandible and part of a skull from a gravel pit near Piltdown, England. The mandible was apelike except for humanlike wear on the teeth; the skull was like a modern human. These bones became the basis for Eoanthropus dawsoni, commonly known as Piltdown Man, interpreted as a 500,000-year-old British ape-man. But in the early 1950s, it was found that the jawbone was stained and filed down to give its appearance and that the skull was a recent human fossil. In short, Piltdown Man was a fraud. British scientists believed it because they wanted to. The failure to expose it sooner shows that scientists tend to be guided by their preconceptions.”
Source:
Gish, Duane T., 1985. Evolution: The Challenge of the Fossil Record. El Cajon, CA: Creation-Life Publishers, pp. 188-190.
LikeLike
I said the evidence for dangerous climate change. I guess you didn’t read that bit, or like to play with words.
Projection.
It’s climate deniers that play with words.
NASA is very clear on the subject of climate change. They don’t play with words at all.
If you want to tell us how NASA and every single scientific community has it all wrong, then by all means share.
http://climate.nasa.gov/
LikeLike
In the 17th century, Galileo challenged the Church of Rome’s geocentric view of…
That’s worth 40 points on the Crackpot Index. Let the ritual dance continue.
LikeLike
Steve Slott | November 12, 2013 at 9:37 am |
Do I really need to post for you, yet once again, a list of peer-reviewed scientific studies that clearly demonstrate the effectiveness of water fluoridation? Do I really need to ask you yet once again to provide valid evidence of ANY adverse effects of water fluoridation? Do I really need to state, yet once again, that at $1 per person per year, there IS no other more cost effective measure that reaches the numbers of people and delivers the amount of dental decay protection as does water fluoridation?
Janet | November 12, 2013 at 8:13 pm |
Does anyone know the cost (in dollars) of Fluoridating water, and the related savings in dental care?
Apologies if this has been already covered.
How very sad.
LikeLike
Robert
“Observational evidence is totally unacceptable…..” You’re certainly welcome to your opinions, Robert. Science disagrees with your assessment.
Yes, I did copy and paste the studies, as I frequently do when addressing the same verbatim, antifluoridationist nonsense for the one hundredth time. The difference is that my copy/pastes are of information I have put together myself, through proper research from accurate, reliable sources, and saved for the next time an antifluoridationist attempts to make the same invalid argument. I have a full understand of what I post. Conversely, you and most other antifluoridationists, simply click on an antifluoridationist website and copy/paste what they have on them, having little understanding as to what it is you’re copying. You then regurgitate what you’ve been fed, out onto a comment section, not realizing that your “information” has been posted, verbatim, by other uninformed antifluoridationists, all over the internet.
Steven D. Slott, DDS
LikeLike
Yes, “Rottweiler” Cedric. A very entertaining one, at that. He keeps me laughing as he slices and dices antifluoridationist arguments down to the core.
Steven D. Slott, DDS
LikeLike
(…I take a bow…)
🙂
LikeLike
Steve
On other sites you’ve digged at others for cutting and pasting. I couldn’t resist highlighting that you have resorted to doing it.
How do you find the studies you cite? Are you accessing some pro-fluoridation abstract database that someone has put together?
“Yes, “Rottweiler” Cedric. A very entertaining one, at that. He keeps me laughing as he slices and dices anti-fluoridationist arguments down to the core.”
Steve , you’re seeing something I can’t see. I think someone above asked if Cedric was Ken’s dog and I think that was a good question.
Robert Brentwood
LikeLike
Hi Robert,
Just wondering what on earth you are doing as this blog is supposed to be a (science based) debate; you don’t seem to be doing either?
….or answering my politely framed question?
LikeLike
Robert
I haven’t resorted to anything. I’ve been pasting my own information for some time. That just saves me from having to retype it each and every time. The point about disingenuous copy/pasting is when people copy information off of websites, having no understanding of what they are even copying, its accuracy, or its validity. I see the same, verbatim comments constantly pasted on site after site. The same, verbatim arguments copy/pasted off of the same websites. Everything I save is information I have put together from reliable, accurate sources, not some misinformation off of “fluoridealert”. The information is specifically what I seek out, and is that of which I have full understanding.
I have no idea as to what a “pro fluoridation abstract database” may be, but the majority of studies I cite are directly from the full studies, themselves, which I have obtained by accessing original sites of the studies and downloading from there or, in many instances, paid $35 or so for them when they are not available for free. I have a pretty good collection of such studies on my computer, which I have obtained in this manner. When i come across a cite of a study with which I’m not familiar, which is becoming few and far between, i look up the study on a primary site. I have no interest in what some third party website such as “fluoridealert” claims a study says, I am only interested in reading the information directly from the study itself. If I am confident that what I read in the abstract fully satisfies what I need to know in the proper context, then I’m often okay with that. If I have any questions about it, however, I download the entire study, either for free or for a price, and I read it.
The same applies to the sites I access for other information. I’m not interested in the least in what some third party website tells me that the CDC, EPA, or any other authoritative source says, I am only interested in reading the information directly from the sources. I frequently cite information directly from the CDC, the EPA, the National Sanitary Foundation, the ADA, the World Health Organization, and other respected sources from their original sites. Accurate information on water fluoridation is readily available to anyone directly from these sites. Therefore, when I see, as I constantly do, antifluoridationists citing biased, antifluoridationist websites as their “references” I know that they are either too lazy to seek out the information themselves and are content to have misinformation spoon-fed to them, or are intentionally trying to steer readers to these websites in blatant efforts to deceive. If they weren’t, they would simply cite the original sites as do I.
Cedric is a very astute commenter who has the knowledge and ability to cut through antifluoridationist BS and expose the true foundation of their objections.
Steven D. Slott, DDS
LikeLike
I am shocked (SHOCKED!!) to find a convergence of climate denialists with anti-fluoridationists.
Who would have guessed it?
LikeLike
Where I come from, Rottweilers are considered a public menace and are neutered and muzzled in public places.
I think it is largely down to their owners though. I don’t blame the dogs
LikeLike
I am shocked (SHOCKED!!) to find a convergence of climate denialists with anti-fluoridationists.
Who would have guessed it?
It’s harder with the anti-fluoridationists to get them to answer the question as to how the the scientific consensus get ut so wrong.
They just don’t appear to have thought that far, or it hasn’t occurred to them to ask themselves the question.
Whereas the climate deniers…well, it’s all on no hold barred… they seldom have a problem identifying the reason: in a full-on global conspiracy of “hard-left Marxist” eco fascist scientists on the take run by Al Gore.
LikeLike
Where I come from, Rottweilers are…
Poor Janet. She’s still confused.
Science denialism happens.
Today it’s the anti-fluoridationists but tomorrow it could just as easily be the anti-vaxxers or the moon landing deniers or the climate deniers or the HIV deniers.
There’s no effective difference.
It’s always the same lame thinking. The same logical fallacies.
The same endlessly resurrected zombie PRATTs.
They never die.
The thinking that that gets you deny the scientific consensus on “X” works just as well to deny the scientific consensus on “Y”.
Only the labels are different.
LikeLike
This discussion is leagues more civilized and logical than average. If you have the impression that community level anti-fluoridation “debates” are much different from what you know of global warming opponents I would suggest you haven’t been out and about enough.
LikeLike
This discussion is leagues more civilized and logical than average If you have the impression that community level anti-fluoridation “debates” are much different from what you know of global warming opponents I would suggest you haven’t been out and about enough.
Lol. Probably true. The fluoride hoo-hah is new arena to me, I certainly observe similar levels of stoopid on display.
LikeLike
Poor Janet. She’s still confused.
About what? Why are you talking about “science denialism”
I looked up dental fluorosis on the CDC website and reported my findings. I’m not quite sure how that constitutes “denialism”
I don’t have any axe to grind on this issue. I was just pointing out that Alison was being a good parent by looking up information about potential risks to her child’s health, and she and I seem to be in general support of Fluoridation within certain constraints.
LikeLike
Why are you talking about “science denialism”…
Lost in a world of her own. How sad.
LikeLike
Mind you, Richard, I have come across quite a number of anti-fluoride activists who talk about Agenda 21 and even claim F is used to control the population through lowering fertility and killing off the oldies.
>
LikeLike
Agenda 21.
(sigh)
I love that conspiracy. It’s got that extra-special nutty flavour.
Labor’s Evil Plan for Australia- Agenda 21 Genocide Plan
LikeLike
I thought the discussion was about dental health. What has Agenda 21 got to do with dental health and Fluoride?
I am being accused of being lost in my own little world. You folks need help
LikeLike
Janet, Agenda 21 really has nothing to do with the fluoridation issue except that a number of anti-fluoridation activists believe that fluoridation is a conspiracy carried out under Agenda 21 to dumb down the population, reduce fertility and kill off old people.
Yes, really mad, I know. But these people are serious, very committed to their view and strongly linked with the organised anti-fluoridation groups. I am always amazed at how many of them there are.
I don’t think we need help here – I have actually been actively moderating contributions to the discussion to weed these extremists out. They are the last people we need.
>
LikeLike
Oh, OK, thanks Ken. I had no idea
LikeLike
I don’t know much about Agenda 21 but during the recent Portland, OR (USA) fluoridation battle a new video titled “The Great Culling,” featuring rather prominently Paul Connett was a significant political element stirring public paranoia.
The first 33 minutes of that can be seen here:
While these outlandish ideas may have little effect on normal voters they are an important element in energizing many of the volunteers who gather signatures, go door to door, steal lawn or vandalize lawn signs (1000 stolen in Portland), walk in parades, or do whatever else assists the campaign.
A very important reason public health science lost in Portland was the peer to peer politics which swept through the blue collar neighborhoods. One of the liberal, alternative life style newspapers (which supported fluoridation) well described the grass roots opposition.
http://www.portlandmercury.com/portland/the-sanest-arguments-against-fluoride/Content?oid=9212701
Politically it does absolutely no good to denigrate these ideas as stupid (pick your adjective). What public health advocates must do is to come to a better understanding of the political and psychological reasons for mistaken belief, and perhaps even more difficult, how to disabuse the general public of these mistakes. Water fluoridation has faced opposition out of step with mainstream scientific consensus from the beginning. Paul Connett and his core supporters has elevated anti-fluoridation political activism world-wide to greater effectiveness.
Australian psychologist Lewandowski is an important resource for helping understand these issues. I highly recommend the following for all who seek to make clear main-stream scientific consensus to the general public
http://www.skepticalscience.com/New-Slideshow-Myth-Debunking-Educators-Science-Communicators.html
http://www.skepticalscience.com/Debunking-Handbook-now-freely-available-download.html
http://www.psychologicalscience.org/index.php/news/releases/misinformation-psychological-science-shows-why-it-sticks-and-how-to-fix-it.html
Click to access LskyetalPsychScienceinPressClimateConspiracy.pdf
Click to access LewandowskyEcker.IP2012.PSPI.pdf
http://www.scientificamerican.com/article.cfm?id=how-to-stop-misinformation-from-becoming-popular-belief
LikeLike
Australian psychologist Lewandowski is an important resource for helping understand these issues.
Are you serious? This guy is unhinged
LikeLike
I would be very interested in hearing your views of Lewandowski’s with respect to his advice on how to overcome the “motivated rejection of science.” This is a bit afield from fluroidation advocacy/opposition.
LikeLike
Lewandowsky recently did a study that involved a sample size of zero. You might be familiar with this Billy Budd
LikeLike
I’m rather surprised hearing of the city of Portland”s decision.
I thought the city was more enlightened than many, so I expected that its citizens would recognise any disinformation campaign as such.
LikeLike
Are you serious? This guy is unhinged
Maybe, but from the strength of your argument, maybe not.
He seemed to nail AGW deniers pretty well
NASA Faked the Moon Landing—Therefore, (Climate) Science Is a Hoax
An Anatomy of the Motivated Rejection of Science
http://pss.sagepub.com/content/24/5/622.abstract
LikeLike
Janet, I have seen no evidence of support for fluoridation from either you or Alison, regardless of any constraints.
Steven D. Slott, DDS
LikeLike
Billie Budd
Perhaps you need Ken to moderate fluoridation discussions in Portland. He allows no garbage to get through him. That probably would eliminate at least 95% of opposition arguments there.
Steven D. Slott, DDS
LikeLike
Janet, I’m not familiar with agenda, but I’m guessing that’s the point. It has nothing to do with fluoride and dental. However, that little detail has never seemed to deter antifluoridationists from invoking such “arguments”.
Steven D. Slott, DDS
LikeLike
“I’m rather surprised hearing of the city of Portland”s decision.
I thought the city was more enlightened than many, so I expected that its citizens would recognise any disinformation campaign as such.”
Richard
You’ve seen Connett’s arguments here, you’ve seen a small sampling of the lack of knowledge and understanding put forth by antifluoridationists who present themselves as authoritative, and you’ve seen the way opponents constantly cite antifluoridationist websites as “support” for the mounds of misinformation they post. Now, think of this with little or no moderation, ten times as ugly and ignorant as has been this discussion, all unleashed onto an area of 900,000 people, with the force of a Class 5 hurricane (typhoon). That may give you some idea of what Connett and his followers did in Portland. Even with that, only 23% of all registered voters carried the day for fluoridation opponents. Yes, that was a 60% to 40% margin of all voters, but it’s not difficult to imagine that had the percentage of voter turnout of fluoride supporters been equal to that of opponents, the outcome would have been much different. The extreme passion of fluoridation opponents brings them out to vote in much greater percentages than fluoride advocates.
Steven D. Slott,,DDS
LikeLike
Lewandowsky recently did a study that was supposed to demonstrate that conspiracy theorists could hold multiple contradictory views simultaneously.
He based his study on the idea that Diana faked her own death, and that MI6 killed Diana
The problem is, the population size who held these contradictory views was zero.
So I don’t really have much confidence in these studies with sub-optimal population sampling.
LikeLike
Steve Slott | November 14, 2013 at 1:49 am |
Janet, I’m not familiar with agenda, but I’m guessing that’s the point. It has nothing to do with fluoride and dental.
You are probably right. A quick search for Agenda 21 and Fluoride leads to one notable place -Alex Jones and PrisonPlanet
LikeLike
‘Nuff said, Janet. I believe you’ve just very nicely clarified the credibility of agenda 21!
Steven D. Slott, DDS
LikeLike
Lewandowsky recently did a study that….
No, don’t do that.
Don’t “helpfully” interpret. Just give us the peer-reviewed research.
No filters. No middlemen. No creative interpretation.
Just the research.
LikeLike
Could you please give some sort of reference
LikeLike
Could you please give some sort of reference
Who? What?
LikeLike
Could you give some sort of reference to Lewandowski’s zero subject study?
LikeLike
Whilst nothing to do with water fluoridation, I will answer Billy’s request here:
LikeLike
Not very impressive, Janet. Basing your claim about Lewandowsky on the opinions of a blogger.
Steven D. Slott, DDS
LikeLike
The opinions of a blogger involved an FOI request to the University for the data, which revealed this information.
Perhaps you could do the same?
Mr McIntyre was one of Time Magazine’s “people of the year” a while back. Maybe you’d like someone of more standing in society to do the same study, like yourself perhaps?
LikeLike
Agenda 21 has plenty of credibility, since it was created by the United Nations at around the time of the Rio Earth Summit.
What doesn’t have credibility is that water Fluoridation is part of that agenda. I think most of it is about sustainability and stuff like that.
LikeLike
Thanks. . that is of interest to me.
LikeLike
If I where a betting man I’d put a wager on Janet being an Andy sockpuppet .
LikeLike
Janet, you make a statement that someone is “unhinged” based on the opinion of someone else. I have no desire to find anyone with an alternative opinion on that. I don’t care. The point I’m making us is that you, like most fluoride opponents, present “facts” as if they are authoritative, yet when pressed for sources, have no foundation other than someone’s opinion. More often than not, this type of support is what opponents purport to be the “science” that supports their position.
Steven D. Slott, DDS
LikeLike
It’s not the opinion of someone else, it is my personal opinion.
If you think this is relevant to the issue at hand, then it is of importance to you.
I can’t understand why.
LikeLike
The point I’m making us is that you, like most fluoride opponents, present “facts” as if they are authoritative, yet when pressed for sources, have no foundation other than someone’s opinion
Steven Stott, I am not a “fluoride opponent”
I have never ever said that I am opposed to fluoride.
You just made that up
I never presented my personal opinion that Lewandowsky is unhinged as a fact. It is my personal opinion.
Maybe you don’t like people having personal opinions.
LikeLike
Janet, it might be best to hold back opinions like suggesting an author is “unhinged.” Especially without any evidence. It is, perhaps, a comment that I should have moderated.
My understanding is that Lewandowsky and others have published on the degree of prevalence of conspiracy theories held by deniers/contrarians/sceptics of climate science. The results are interesting, and anecdotally I have observed such congruence of conspiracy theories on issues of climate change and fluoridation. Agenda 21 is a very common one – and in NZ both opponents of climate change science and fluoridation often resort to it. Have a look at this video attacking science, scientist (and me) made in NZ by a conspiracy theorist (Vinny Eastwood) closely connected with FANNZ (and on excellent terms with Connett by the way) – https://openparachute.wordpress.com/2013/10/05/cyber-bullying-of-science/
However, I am sure that as a sociological study there will be a lot to debate about the findings reported in his paper. There certainly have been many attacks on the work by climate change deniers – as would be expected. All I ask as that discussion on his work here be in good faith and not make claims of him being “unhinged.”
>
LikeLike
OK, fair enough Ken.
I was really basing my opinion on this video of Lewandowsky.
Comments have been disabled for the video. Not surprising really.
LikeLike
…video of Lewandowsky…
Sound message, terrible delivery.
LikeLike
Janet, your statements in regard to Lewandowsky are relevant to the issue of fluoridation only because they demonstrate the type of evidence upon which you base your opinions.
Steven D. Slott, DDS
LikeLike
What are you basing your opinions on Steven?
Just because I think one psych Professor is a crackpot doesn’t make me an anti-fluoridationists or a conspiracy theorist.
Are you aware that some of his papers have been retracted after complaints from people that were targeted in them, for example?
LikeLike
Janet, based on your comments in this section, there is very little doubt that you are an opponent of fluoridation. You are either deluding yourself or being disingenuous if you maintain otherwise. Attempts to portray themselves as “open-minded”, of “no-opinion” , or other such denials of opposition when their statements belie those claims, are a common trait of fluoridation opponents.
Steven D. Slott, DDS
LikeLike
Janet, based on your comments in this section, there is very little doubt that you are an opponent of fluoridation. You are either deluding yourself or being disingenuous if you maintain otherwise
Wow, I had no idea that I was an opponent of fluoridation. I just looked at this debate, found some interesting arguments on both sides.
Which comments in particular lead you to the conclusion that I am an opponent of fluoridation?
LikeLike
Janet, your opinion of Lewandowsky plays no part in my concluding that you are a fluoridation opponent. Here is upon what I base my assessment:
“Maybe the evidence that Fluoride is 100% safe is not so strong then.”
—————-
“There are many examples of science that supports a particular position being promoted by NGOs and governments. Perhaps this also applies to Fluoridation?
I don’t have the answers to this, but I get suspicious when science is presented as settled, 100% correct and of asbolutely no question.”
—————-
“Yet Steven Stott only wants to discuss peer reviewed studies. Do these peer reviewed studies have any analysis of political or technical issues?
If it is more a political and technical issue than scientific, then why are some of your commenters comparing people who are opposed to bulk fluoridation of water as “anti-science”, and akin to creationists?
Maybe they are opposed because of the political, technical, or cultural issues that you admit may be more important than the scientific ones?”
—————
“Water fluoridation is the opposite. We artificially add fluoride to water to solve the supposed problem of tooth decay.
It is incumbent on those doing this to the water to show that it is an effective, safe, and economically sound process.
It is not incumbent on the “anti” group to prove that fluoridation is dangerous, or undesirable for some other reason. The “pro” group are changing the chemical makeup of the water supply. It is entirely their responsibilty to justify the process, and science can only play an advisory role in this.”
————–
AND, this classic antifluoridationist comment ripped directly from the headlines of “fluoridealert.org”!! ……..
“If Fluoridation of water is universally accepted as a good thing, why does only 5% of the world fluoridate their water?”
————-
I rest my case.
Steven D. Slott, DDS
LikeLike
Yes, all these statements I stand by.
It doesn’t make me an “anti-Fluoridationist”
However, Steven Stott, I have come to the conclusion that you are a narrow-minded zealot.
I certainly wouldn’t trust anything that you said or wrote, based on what I have read here.
I came here with an open mind looking for a reasonable debate, and I find the “pro” side the most dogmatic, just like the climate change crazy people
LikeLike
The comment I wrote about 5% of the world using Fluoride was mine alone. If someone else wrote it too then it is pure coincidence
LikeLike
I agree, Richard, I do not see anything wrong with the message in the video. He makes some important points.
>
LikeLike
Janet, please – you destroy your own credibility by putting people down with words like “crackpot.” Rather than use emotive terms what about being specific? – showing us the papers retracted and why and enabling us to form our own judgements.
Unfortunately it is this sport of innuendo and backstabbing that climate deniers resort to all the time as a diversion from real evidence. And this also happens with activist opponents of fluoridation.
>
LikeLike
Janet, you just keep digging yourself deeper and deeper.
I guess you just happened to ferrett out the nugget about “5% of the world” on your very own, after hours and hours of combing relentlessly through statistical analyses of fluoridation practices of other countries. It truly is an amazing coincidence that I have seen that comment no fewer than a hundred times posted all over the internet by antifluoridationists.
Will wonders never cease.
Steven D. Slott, DDS
LikeLike
Janet, I am putting you back into moderation. Let’s nip this in the bud. Name calling is not helping promote good faith discussion.
LikeLike
I read that 5% number somewhere on this blog I think. I have never ever been to any anti-fluoridation website ever, in my entire life.
I was interested in the topic I had a genuinely open mind about something I knew (and still know) little about.
Just asking a few reasonable questions (and concurring that Alison was being a good parent) and quoting from the CDC website somehow makes me anti.
If you want to get people to see your point of view, hectoring them and name calling really doesn’t win anyone over.
LikeLike
As fun as this is, i must now double my dose of blood pressure medication and dive into Dr. Connett’s next response, which undoubtedly will be every bit as enlightening as his others…….
Steven D. Slott, DDS
LikeLike
Ken, you can read about the retracted Lewandowsky paper at Retraction Watch blog
http://retractionwatch.wordpress.com/2013/03/28/why-publishers-should-explain-why-papers-disappear-the-complicated-lewandowsky-study-saga/
LikeLike
Janet, I think there is some confirmation bias going on here. That link does not show what you claim. And is certainly no justification for name calling.
LikeLike
The importance of Lewandowski’s work has not to do with documenting paranoid conspiracy theories but rather on strategies which might more effectively communicate scientific information in the face of prior motivated beliefs opposing a variety of issues.
With that in mind, I personally thought Janet’s opinion potentially helpful. It is always a good idea to try to scrutinize those whom we turn for guidance.
LikeLike
Hey Janet,
So…would you describe yourself as pro, anti or sitting on the fence?
The…” I have never ever been to any anti-fluoridation website ever, in my entire life” is intriguing as you appear quite adept in the blogosphere.
Really! after all these posts you haven’t even taken a peek…?
LikeLike