
This is Paul Connett’s second response to Ken Perrott’s original article – Fluoride debate: Why I support fluoridation In it he is responding to Ken’s article Fluoride Debate: Why I support fluoridation – response to Connett.
I am going to ignore most of the personal criticisms in Ken’s response to my critique of his opening statement and focus largely on the science and scientific studies in question.
1. Different interpretations of the Li et al. (2001) paper
I am very familiar with the Li et al. (2001) paper on bone fractures in the elderly in six Chinese villages with fluoride concentrations in well water ranging from about 0.25 to 8 ppm. In fact, I reviewed a pre-publication copy of this paper sent to me by the lead author as part of my invited peer review of the York Report (McDonagh et a., 2000).
Had Ken taken advantage of my sending him the full pdf text of our book he would have quickly seen that the charge he levels at me of selectively using the Li et al (2001) text on bone fractures from China is grossly inaccurate.
Instead of relying on the misleading commentary of pro-fluoridation activist Kurt Ferre, he could have read Chapter 17 of our book (The Case Against Fluoride, CAF), where we covered both parts of Li’s paper. The part Ken and Ferre cover, shows a U-shaped curve for all fractures combined. This shows a minimum for fracture rate at the village at 1 ppm. It could be argued – as Ken does – that at 1 ppm fluoride may confer some benefit in strengthening of elderly bones after a lifetime of exposure. However, such an argument is somewhat muted by the second part of Li’s paper that deals with hip fractures, which is the most critical bone fracture for elderly people, since about half of the elderly never regain an independent existence after such a fracture. In this part of the study there is no U-shape – i.e. no apparent protection offered by fluoride against hip fracture – and the hip fracture prevalence appears to increase in a linear fashion above 1 ppm (actually maybe from 0.25 ppm).
This systematic increase becomes more apparent when one checks our re-plot of the data– see Figure 17.2 on p.179.
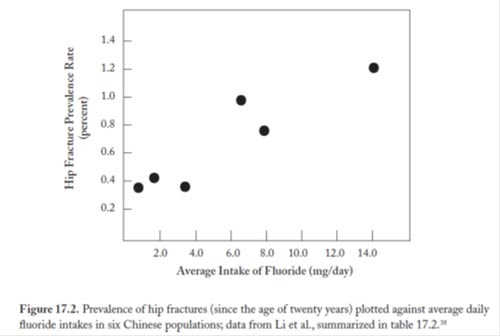
Please note I say replot because the graphs provided by Li et al (2001), including the one used by Ken, are not real plots at all. They are only illustrative. The points on the x-axis neither represent an average of the fluoride concentration in each village nor the estimated dose (mg/day) calculated by the authors, the six data points are simply evenly spaced out to illustrate which village is being represented for the fracture data on the y-axis. In the case of Figure 17.1 it makes little difference when one puts in the average dose in mg/day, but in the case of Figure 17.2 it makes a big difference and shows up this “apparent” linear trend more clearly.
While Ken is correct when he says that the only individual village to show a statistically significant increase in hip fractures is village 6, based on our replot the increases in villages 4 and 5 appear to be “real,” even though they are not statistically significant individually. In fact, the data for the whole set of villages appear consistent with a linear regression. Statistical significance is not the final word on whether a data point or data set is real or not. In our view, a linear increase in fracture rate for villages 3 through 6 (and maybe even villages 1-6) looks a more reasonable interpretation of the data than a threshold (i.e. a sudden tripling of the hip fracture rates) at village 6, the interpretation that Ken prefers.
It is unfortunate that Ken uses an inaccurate commentary from Ferre to mischaracterize what we did here.
2. Other studies of fluoride and the bone
However, there is a great deal of literature available on fluoride’s impact on the bone (see the references to Chapter 17, CAF). Ken will need more than the Li et al (2001) paper to establish that there is an overall benefit to the elderly bone when people are exposed for a lifetime to an approximate ten-fold increased exposure to fluoride via artificially fluoridated water. This is especially true for people with poor kidney function and high water drinkers (miners in Western Australia drink between 10 and 12 liters of water a day). Can you provide more studies that support the possibility that fluoride protects the elderly bone Ken?
Nor is it just the bones of the elderly that is in question. I am still waiting to see Ken’s response to the finding in the Schlesinger et al (1956) study of the second fluoridation trial (Newburgh-Kingston, NY, 1945-55) in which they reported a statistically significant increase in the prevalence of cortical bone defects (the ratio was about 2 to 1) in children in the fluoridated community versus the non-fluoridated community. The cortical bone is the outside lamellar structure of the bone whose integrity is important in resisting fractures. We discuss Schlesinger’s work in CAF (p.96).
I am not aware of any health agency in any fluoridated country comparing fracture rates in children in fluoridated versus non-fluoridated communities or even examining fracture rates in children as a function of the severity of dental fluorosis. Scientists did this in Mexico (Alarcón-Herrera et al., 2001) and found an increase in fractures as the severity of dental fluorosis increased (see P.169, CAF). No attempt has been made to reproduce this result or conduct a similar study in any of the fluoridated countries.
3. Fluoride’s topical action and saliva
As far as the mechanism of fluoride’s topical mechanism on the teeth is concerned, Ken quotes the CDC from 2001,
” . . drinking fluoridated water, brushing with fluoride toothpaste, or using other fluoride dental products can raise the concentration of fluoride in saliva present in the mouth 100-to 1,000-fold. The concentration returns to previous levels within 1–2 hours but, during this time, saliva serves as an important source of fluoride for concentration in plaque and for tooth remineralization.”
I went back to this CDC Oral Health Division statement from 2001 and found the sentences that preceded Ken’s quote most revealing. These preceding sentences read:
“Saliva is a major carrier of topical fluoride. The concentration of fluoride in ductal saliva, as it is secreted from salivary glands, is low – approximately 0.016 parts per million (ppm) in areas where drinking water is fluoridated and 0.006 ppm in nonfluoridated areas (27). This concentration of fluoride is not likely to affect cariogenic activity. However, drinking fluoridated water, brushing with fluoride toothpaste…
These few sentences further strengthen Ken’s arguments that it is fluoride delivered directly into the mouth that provides the saliva with concentrations, which may or may not do something and not, the meager concentrations reached systemically through the salivary gland, a position I erroneously attributed to him. My apologies.
As the CDC states the concentration of fluoride delivered by the saliva gland “is not likely to affect cariogenic activity.” However, if it is the fluoride levels reached when fluoridated water has entered the mouth that is the key dynamic for fighting tooth decay, then I think this weakens the need to force people to drink fluoridated water. Maybe we should be suggesting that people swish with fluoridated bottled-water and then spit it out! I also have to wonder why we are giving fluoridated water to babies before their teeth have erupted.
Let me ask for the third time how Ken feels about an alternative delivery system for fluoridated water. This would involve using fluoridated bottled-water in one-liter bottles at 0.7 – 1.2 ppm. These could be made freely available in dental offices (supermarkets, pharmacies or clinics). With this approach one could a) use pharmaceutical grade sodium fluoride; b) could control the dose and c) avoid not forcing it on people who don’t want it. Nor does it involve giving up the central paradigm of the fluoridation program.
As far as the rest of the 2001 CDC quote is concerned I think the Oral Health Division is using a slight of hand here by mixing up a discussion of fluoride in food and water with the fluoride in toothpaste. That 100-1000 fold increase might take place when toothpaste containing 1000 or even 1500 ppm is used but is hardly likely with water at 0.7- 1.2 ppm.
I think the CDC put the “cat among the pigeons” among both fluoridation opponents and proponents when it admitted in 1999 that:
“Fluoride’s caries-preventive properties initially were attributed to changes in enamel during tooth development… However, laboratory and epidemiologic research suggest that fluoride prevents dental caries predominantly after eruption of the tooth into the mouth, and its actions primarily are topical…” (CDC, 1999).
It maybe that the CDC Oral Health Division in its 2001 paper was scrambling to salvage some kind of role for fluoridated water, sufficient to justify continuing its long-time support and promotion of the fluoridation program, despite its admission of the predominance of a topical effect. However, It would have been better if, in 1999, the CDC had changed the focus of its efforts from delivering fluoride systemically to delivering it topically, as well as addressing other key issues of diet, regular brushing and providing early interventions for children of low-income families.
In the latter respect I do not understand why Ken completely ignored the exciting news that I provided from unfluoridated Scotland, where they are having great success with teaching toothbrushing to infants as well providing better diets and earlier interventions.
As far as the mechanisms that Ken offers for a topical benefit derived from fluoridated water directly to the saliva in the mouth (and not via systemic exposure), he discussed “fluoride ions transferring from the water (or food) to saliva (and biofilms on the teeth).”
My experience when drinking water is that it hits the tongue, the back of the top front teeth and the palate before it swiftly goes down the gullet (unless it is deliberately swished). It seems to me that the fluoride ions have little opportunity to form a biofilm on any teeth other than the back of the front teeth. Nor is there much time to mix with the saliva. But this is only conjecture based on simple personal observations on my part and if Ken has a study that shows the level of fluoride in the saliva is dramatically increased immediately after someone has swallowed a glass of water that would be very helpful.
4. The work of Xiang et al (2003) on IQ
Ken suggests that I am “cherry picking” the data by “singly pulling out the Xiang et al. study from 2003.” In actuality, I gave that as a specific example of a human study where effects were found at concentrations very close to the level at which we artificially fluoridate (0.7 to 1.2 ppm). This was in response to Ken’s claim that he was not impressed by all the high concentration animal studies that have found fluoride causes harm. I cited Xiang in the larger context of 37 (out of 46 human studies that have found an association between fluoride exposure and lowered IQ.) These studies come from India, Iran, Mexico and China, with the majority coming from China. 27 of them were reviewed by a Harvard team (Choi et al., 2012). Of these 27 studies 26 found a lowering of IQ (average of 7 IQ points). These results are remarkably consistent even though they have been performed in several different countries and many different parts of China. However, proponents of fluoridation have dismissed them on the basis that in two of these studies the range in the high fluoride village went up to 11.5 ppm. However, I pointed out that nine of the studies found a lowering of IQ at or less than 3 ppm, which offers no adequate margin of safety for a whole population drinking water in the range 0.7 to 1.2 ppm. So I wasn’t cherry picking here. We have to see Xiang’s work in the context of all these other studies as well as the other studies that show that fluoride is a neurotoxicant (discussed below). I chose Xiang’s study because it is one of the better studies. It controlled for more potential co-founders than others (including lead and iodine intake). Recently, Xiang has confirmed that as far as arsenic was concerned there were higher levels in the low fluoride village, so clearly arsenic was not a factor in the lower IQs found in the high fluoride village.
Yes, there are weaknesses in many of these IQ studies but the greatest “weakness” is the fact that countries that practice water fluoridation have made virtually no attempt to reproduce them or pursue the matter in any way. That is why, as Ken complains, I have not quoted studies from a wider range of countries: apart from a small early study in NZ (Shannon et al., 1986) and small behavioral study in the US (Warren et al., 1998) there aren’t any. At the very least these studies from China, India, Iran and Mexico represent a serious red flag on this practice and the health agencies in fluoridated countries are ignoring this red flag.
In his further attempt to downplay Xiang’s 2003 study Ken asks
“Why did the authors choose to publish in the journal “Fluoride?” It is certainly not considered of high quality. It is actually rather suspect because of the ideological committment of the editors. This gives the impression that even suspect papers will be published if the story is right.”
I discuss these derogatory comments about Fluoride and its editors, and the double standard that Ken and other proponents of fluoridation exercise on this matter below, here I would like to discuss more about Xiang’s work.
5. Xiang and the journal Environmental Health Perspectives
Xiang almost certainly chose to publish in the journal Fluoride because it has probably given more coverage to the possibility that fluoride affects the brain of animals and lowers IQ in humans than any other journal in the world.
That being said if Ken is going to make judgments based on what journal the article appears in, then he might be interested by the fact that in 2010 Xiang et al submitted an updated version of their work to one of the leading environmental health journals, Environmental Health Perspectives, which is published by the National Institute of Environmental Health Sciences (NIEHS) a division of the National Institute of Health (NIH). After peer review this journal agreed to publish Xiang’s work and posted a pre-publication copy on the internet (see Xiang et al., 2010).
However, Xiang was asked to withdraw his article for the technical reason that some of the material had already been published by this team (and that was the Fluoride article from 2003). But the key fact from the point of view of this discussion is that despite Ken’s criticisms Xiang’s work was peer-reviewed by this prestigious journal and was found acceptable for publication.
The update from Xiang was very important for this discussion and it is a pity that this was withheld from the mainstream scientific community. Xiang found that the lowering of IQ in his study correlated with the fluoride levels in the children’s plasma. This greatly strengthens Xiang’s finding by moving from a population (or ecological) study closer to a study based on individual exposure. Xiang finally published this part of his finding in Fluoride (Xiang et al., 2011).
Despite all of this, Ken considers Xiang’s paper “a minor piece of evidence” and argues that,
“it should be objectively considered together with all other publications in this area of research. The fact that it is taken in isolation (except for a few other low quality Chinese studies), and nothing of higher quality or from different regions is considered, makes me suspicious. After all, a number of countries with highly qualified scientists (and activists claiming negative effects) have had many years to look at possible health effects from fluoridation. The fact that more credible papers are not produced is hardly good evidence for the claims made by anti-fluoride activists. Why would they rely on low quality research if better research supporting their claims was available?”
First of all, I argue that this study by Xiang is part of a large body of work that indicates that fluoride can damage the brain and I have summarized this large body of work previously (and it can be found at www.FluorideAlert.org/issues/health/brain )
So when Ken argues that “Papers are selected and then values are pulled out of them to make assertions or claims that really are not warranted – and certainly not by a balanced reading of the literature.”
I must ask Ken what “balanced reading of the literature” on fluoride’s potential to damage the brain are you talking about? I have cited a large body of work and it almost all goes in one direction: fluoride is a potent neurotoxicant. Can you cite an extensive body of literature Ken that points in the opposite direction?
6. Fluoridated countries are not doing studies on key health concerns
Sadly, as I have already indicated the health agencies in those countries that support and promote fluoridation show absolutely no inclination to study their populations with respect to this effect, i.e. lowered IQ.
In fact the scientist who published one of the earliest animals studies on fluoride and animal behavior, Dr. Phyllis Mullenix, was fired after her paper was accepted for publication (Mullenix et al., 1995). Mullenix was the chairperson of the first toxicology department in any dental school in the US. She was hired specifically to look at the neurological effects of the chemicals used in dentistry. However, when she found changes in animal behavior related to fluoride exposure and published it, she was told that her work was “no longer relevant to dentistry.” I would argue that her work conflicted with dental establishment’s determination to continue the fluoridation program at all costs. The treatment meted out to Mullenix did not go unnoticed by members of the research community, who have treated doing research on fluoride like touching the third rail as far their careers were concerned.
In addition to their lack of interest in pursuing the lowering of IQ, neither health agencies nor those “highly qualified scientists” Ken talks about, have been inclined to fully investigate many other serious concerns such as lowered thyroid function, accumulation in the pineal gland (Luke 1997, 2001), arthritis rates in fluoridated populations, bone fractures in children (discussed above), earlier onset of puberty, behavioral problems in children and the plight of those who claim to be highly sensitive to fluoride’s toxicity.
All these concerns cry out for attention and certainly the attention of those critical of the epidemiology of studies conducted in those countries that are investigating some of these issues because they are legitimately concerned about what naturally fluoridated water is doing to their citizens. I have expressed my own thoughts on the reason for this lack of attention, but I would be interested in Ken’s thoughts on this overwhelming lack of scientific interest in investigating fluoridation’s potential health effects in the many years since the US Public Health Service endorsed fluoridation in 1950? Why in fluoridated countries are we getting an endless stream of studies on teeth but virtually none on other tissues in the body?
7. What other authorities are saying about fluoride as a neurotoxicant
Meanwhile, I am not the only scientist who is expressing concerns about fluoride’s neurological affects. According to the report by US National Research Council (NRC, 2006):
“A few epidemiologic studies of Chinese populations have reported IQ deficits in children exposed to fluoride at 2.5 to 4 mg/L in drinking water. Although the studies lacked sufficient detail for the committee to fully assess their quality and relevance to U.S. populations, the consistency of the results appears significant enough to warrant additional research on the effects of fluoride on intelligence.” p.8
(Note from PC: this comment was based on a review of only five of these IQ studies, there have now been 42.)
“On the basis of information largely derived from histological, chemical, and molecular studies, it is apparent that fluorides have the ability to interfere with the functions of the brain and the body by direct and indirect means.” p.222
“histopathological changes similar to those traditionally associated with Alzheimer’s disease in people have been seen in rats chronically exposed to AlF.” p.212
“Fluorides also increase the production of free radicals in the brain through several different biological pathways. These changes have a bearing on the possibility that fluorides act to increase the risk of developing Alzheimer’s disease.” p.222
“More research is needed to clarify fluoride’s biochemical effects onthe brain.” p.222
“The possibility has been raised by the studies conducted in China that fluoride can lower intellectual abilities. Thus, studies of populations exposed to different concentrations of fluoride in drinking water should include measurements of reasoning ability, problem solving, IQ, and short- and long-term memory.” p.223
“Studies of populations exposed to different concentrations of fluoride should be undertaken to evaluate neurochemical changes that may be associated with dementia. Consideration should be given to assessing effects from chronic exposure, effects that might be delayed or occur late-in-life, and individual susceptibility.” p.223
EPA researchers listed fluoride among those chemicals for which there was “substantial evidence of developmental neurotoxicity” (W. Mundy et al. http://www.epa.gov/ncct/toxcast/files/summit/48P%20Mundy%20TDAS.pdf
The EPA headquarters scientists made this request to the U.S. Senate in 2000 (Hirzy 2000):
“We ask that you order an epidemiology study comparing children with dental fluorosis to those not displaying (fluoride) overdose during growth and development years for behavioral and other disorders.”
And according to Dr. Philippe Grandjean, one of the authors of the Choi et al (2012) study:
“Fluoride seems to fit in with lead, mercury, and other poisons that cause chemical brain drain. The effect of each toxicant may seem small, but the combined damage on a population scale can be serious, especially because the brain power of the next generation is crucial to all of us.” (Harvard Press Release)
As such it seems reckless to me – and many others – that we should knowingly increase the whole population’s exposure to this neurotoxicant by putting it into the public water supply.
Meanwhile, according to my son Michael Connett, who is the special project director at FAN, and compiled FAN’s Health Database, research on fluoride and the brain in animals has been rolling in at a steady pace over the past year — with over a dozen new studies, including some at notably low doses. One such study that is worthy to have on the radar is a study on mice by Liu et al, 2013. It reports that exposure to fluoride in drinking water (at 5 and 10 ppm) 4 weeks after weaning not only impaired cognition, but caused “anxiety- and depression-like behavior” as well. Here’s an excerpt from the discussion:
“Almost all existing epidemiological surveys on areas with high-fluoride drinking water have focused on cognition; however, our data suggest the need for a large-scale epidemiological survey to investigate whether drinking water with high levels of fluoride can lead to human emotional behavior changes. In summary, we found developmental fluoride exposure through drinking water 1) caused cognitive impairment and 2) led to anxiety- and depression-like behavior in adult mice. Therefore, consideration should be given to the neurotoxicity of fluoride used to combat dental caries, and attention should be paid to the concentration and dosage of fluoride, especially in young children. Our data suggest that excessive fluoride intake should be avoided to prevent its adverse effects.”
So the weight of evidence that fluoride impacts both the brain of animal and humans keeps piling up. About the only animal study that proponents can produce that has not found an effect is one performed by Whitford et al., 2009, who used behavioral tests on rats. They found no neurotoxic effects in their study setting. The study is limited because the rats were not dosed in utero or even during earliest post-natal development, but only after they had been weaned, which roughly translates to adolescence in rats.
Even if this had been a strong animal study, it is one of a small minority that found no evidence of neurotoxicity of fluoride. So, taking the scientific evidence on this topic as a whole, the weight of evidence from both animal and human studies is that fluoride is a developmental neurotoxicant.
8. The journal Fluoride and the ISFR
In his commentary on Xiang’s IQ paper Ken chose to do what a number of proponents of fluoridation do and that is to try and trash the journal Fluoride. He claims that Fluoride “is certainly not considered of high quality. It is actually rather suspect because of the ideological commitment of the editors.”
Why is it Ken you see proponents’ support of fluoridation as being “scientific” and opponents’ opposition to fluoridation as being “ideological”? Isn’t it possible that opponents of fluoridation are opposed for scientific reasons?
Fluoride is the only journal in the world, which is completely devoted to research on fluoride in many different areas of study (geological, biological, biochemical, toxicological, epidemiological, medical and dental to name a few). To its discredit the US National Institute of Health (NIH) has refused to cover the contents of this journal in PubMed, thus depriving many researchers valuable information on fluoride’s toxicity. This has been particularly true of depriving the mainstream medical community (many of whom use PubMed as their primary research tool) knowing about the extensive database indicating that fluoride is a neurotoxicant. It has done this despite covering the contents of far lesser journals and even trade magazines.
There have been three editors of Fluoride since it began its quarterly publication in 1968: Dr. George Waldbott, Dr. John Colquhoun and Dr. Albert Burgstahler (who passed away a few weeks ago). You would be correct in asserting that each of these editors was opposed to fluoridation, however that opposition was rooted in science not some ill-defined ideology. I think you can get a glimpse of the caliber of both Dr. George Waldbott and Professor Albert Burgstahler in the book they co-authored “Fluoridation: The Great Dilemma.” (Coronado Press, Lawrence, Kansas, 1978).
I met Dr. John Colquhoun (briefly before he died in 1998) and videotaped an interview with him during to trip to NZ. I count this interview one of the great moments of my scientific career. Never have I been more impressed by someone’s character than I was by John. He had been an avid promoter of fluoridation both as the chief dental officer of Auckland and as a city councilor. When during a world tour in 1980 (he went to Australia, Asia, North America and Europe) he found that talking behind the scenes to leading dental researchers that they were not finding much of difference between tooth decay in fluoridated and non-fluoridated communities and found the same in “confidential reports” from the NZ dental authorities on his return, he had the enormous courage and scientific integrity to come out publicly against water fluoridation and spent the rest of his life trying to right the wrong he had done. But while he was at the reins he never hesitated to allow pro-fluoridation voices and articles to be published in Fluoride.
I worked with professor Albert Burgstahler for many years and I can vouch for his scientific integrity. In fact for me he represented one of the pinnacles of scientific integrity and that is why FAN named an annual award in his name.
I never met Dr. Waldbott, but I know that his position was that neither the journal nor its supporting organization (the International Society for Fluoride Research, ISFR) should adopt a formal opposition to fluoridation (and its membership included both pro and anti-fluoridation scientists), but to publish as much science as they could on the subject – and as far as water fluoridation was concerned from both sides – and to let the chips fall where they may. He and his successors also believed that if the science was aired fully and openly it would lead most independent scientists to an anti-fluoridation position.
9. The double standard
Unfortunately, none of the dental journals have adopted the same openness on this issue. By and large they do not entertain any anti-fluoridation editorial or even a review that conflicts with their mantra that fluoridation is “safe and effective.” So I think Ken is exercising a double standard here.
I should also point out that there have been several occasions where dental journals have gone out of their way to publish papers that have provided an “ideological” as opposed to a “scientific” support for one side of a controversial matter. Take the example of osteosarcoma. In 1991, shortly after the 1990 NTP animal study had found an association in male rats between fluoride exposure and osteosarcoma, the Journal of the American Dental Association (JADA) rushed to give prominence (i.e. the front cover was devoted to it) to an article, in which the authors clearly reveal their bias in favor of fluoridation. In this very small epidemiological study they proposed that far from causing osteosarcoma fluoride was actually protective against it (see P.187 in The Case Against Fluoride, CAF).
I think the following comments reveal a greater sensitivity to the need to protect the fluoridation program than protecting a few young boys from a life threatening disease:
“An incorrect inference implicating systemic fluoride carcinogenicity and its removal from our water systems would be detrimental to the oral health of most Americans, particularly those who cannot afford to pay for increasingly expensive restorative dental care . . .Because of its strengthening action, fluoride has been widely accepted as the responsible agent for the dramatic declines in the tooth decay rates of U.S. children and adolescents . . . A disruption in the delivery of fluoride through municipal water systems would increase decay rates over time . . . Linking of fluoride ingestion and cancer initiation could result in a large-scale defluoridation of municipal water systems under the Delaney clause. (McGuire et al., 1991, quoted on p. 187, CAF).
In my view the commentary (above) plus the JADA editors’ choice to give it this article full-front page coverage is an example of “ideology” not science at work. The authors and the journal both had a need to protect the fluoridation program at all costs – even if it meant downplaying the concerns about the fate of the young boys in question. I will pick up the osteosarcoma story again in a later submission.
10. A request to Ken
Finally, Ken I think it would save us all a lot of time if – putting the rhetoric and your general disdain for the opponents of fluoridation to one side – you would be kind enough to list the primary studies that you have read that have most convinced you that fluoridation is both safe for the bottle-fed baby and for the adult over lifelong exposure.
References
Alarcón-Herrera et al., 2001. “Well Water Fluoride, Dental Fluorosis, Bone Fractures in the Guadiana Valley of Mexico,” Fluoride 34, no. 2 (2001): 139–49
http://www.fluorideresearch.org/342/files/FJ2001_v34_n2_p139-149fig.pdf
CDC, 1999. Centers for Disease Control and Prevention, “Achievements in Public Health, 1900–1999: Fluoridation of Drinking Water to Prevent Dental Caries,” Mortality and Morbidity Weekly Review 48, no. 41 (October 22, 1999): 933–40, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4841a1.htm
CDC, 2001. Centers for Disease Control and Prevention, “Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States,” Morbidity and Mortality Weekly Report 50, no. RR14 (August 17, 2001): 1–42, http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5014a1.htm
Choi AL, Sun G, Zhang Y, Grandjean P. 2012. Developmental fluoride neurotoxicity: a systematic review and meta-analysis. Environ Health Perspect 120:1362–1368.
Connett, P., Beck, J and Micklem HS. The Case Against Fluoride. Chelsea Green, White River Junction, Vermont, 2010.
Harvard School of Public Health. (2012). Impact of fluoride on neurological development in children. July 25. Available online at: http://www.hsph.harvard.edu/news/features/fluoride-childrens-health-grandjean-choi/
Hirzy, 2000. Statement of Dr. J. William Hirzy, National Treasury Employees Union Chapter 280 before the Subcommittee on Wildlife,
Fisheries and Drinking Water, United States Senate. June 29, 2000.
Li, Y et al., 2001. “Effect of Long-Term Exposure to Fluoride in
Drinking Water on Risks of Bone Fractures,” Journal of Bone and Mineral Research 16, no. 5 (2001): 932–39.
Liu F. et al., 2013 (online) (hard copy 2014). “Fluoride exposure during development affects both cognition and emotion in mice.” Physiology & Behavior 124 (2014) 1–7.
Luke, J, 1997, “The Effect of Fluoride on the Physiology of the Pineal Gland,” PhD thesis, University of Surrey, Guildford, UK, 1997. Excerpts at http://fluoridealert.org/studies/luke-1997/ and a complete copy of Dr. Luke’s dissertation can be downloaded at http://www.fluoridealert.org/wp-content/uploads/luke-1997.pdf (with the author’s permission).
Luke, J, 2001. “Fluoride Deposition in the Aged Human Pineal Gland,” Caries Research 35, no. 2 (2001): 125–28.
McDonagh et al., 2000. “Systematic Review of Water Fluoridation,” British Medical Journal 321, no. 7265 (2000): 855–59, http://www.bmj.com/cgi/content/full/321/7265/855 Note: The full report that this paper summarizes is commonly known as the York Review and is accessible at http://fluoridealert.org/re/york.review.2000.pdf
McGuire et al, 1991. “Is There a Link between Fluoridated Water and Osteosarcoma?” Journal of the American Dental Association 122, no. 4 (1991): 38–45.
Mullenix, PJ et al., 1995. “Neurotoxicity of Sodium Fluoride in Rats,” Neurotoxicology and Teratology 17, no. 2 (1995): 169–77.
Morgan, L. et al. 1998, “Investigation of the Possible Associations between Fluorosis, Fluoride Exposure, and Childhood Behavior Problems,” Pediatric Dentistry 20, no. 4 (1998): 244–52.
NRC, 2006. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards (2006) http://www.nap.edu/catalog.php?record_id=11571
NTP, 1990. National Toxicology Program, “NTP Technical Report on the Toxicology and Carcinogenesis Studies of Sodium Fluoride (CAS no. 7682-49-4) in F344/N Rats and B6C3F1 (Drinking Water Studies),” Technical Report 393, NIH publ. no. 91-2848, National Institutes of Health, Public Health Service, U.S. Department of Health and Human Services, Research Triangle Park, NC, 1990.
E. R. Schlesinger, D. E. Overton, H. C. Chase, and K. T. Cantwell, “Newburgh-Kingston Caries-Fluorine Study XIII. Pediatric Findings After Ten Years,” Journal of the American Dental Association 52, no. 3 (1956): 296–306.
Shannon, FT et al., 1986. “Exposure to Fluoridated Water Supplies and Child Behaviour,” New Zealand Medical Journal 99, no. 803 (1986):416–18.
Waldbott, GL, Burgstahler,AW and H. L. McKinney, Fluoridation: The Great Dilemma (Lawrence, Kansas: Coronado Press, 1978).
Whitford, GM et al. 2009. “Appetitive-based Learning in Rats: Lack of Effect of Chronic Exposure to Fluoride,” Neurotoxicology and Teratology 31, no. 4 (2009): 210–15.
Q. Xiang, Y. Liang, L. Chen, et al., “Effect of Fluoride in Drinking Water on Children’s Intelligence,” Fluoride 36, no. 2 (2003): 84–94, http://www.fluorideresearch.org/362/files/FJ2003_v36_n2_p84-94.pdf
Q. Xiang, Y. Liang, M. Zhou, and H. Zang, “Blood Lead of Children in Wamiao-Xinhuai Intelligence Study” (letter), Fluoride 36, no. 3 (2003):198–99, http://www.fluorideresearch.org/363/files/FJ2003_v36_n3_p198-199.pdf
Xiang, Q. et al., 2010. “Serum Fluoride Level and Children’s Intelligence Quotient in Two Villages in China.” Environmental Health Perspectives. EHPonline.org
Xiang, Q. et al. 2011. “Analysis of children’s serum fluoride in relation to intelligence scores in a high and low fluoride village in China.” http://www.fluorideresearch.org/444/files/FJ2011_v44_n4_p191-194_sfs.pdf
Anyone wanting to follow the debate and/or check back over previous articles in the debate can find the list of articles at Fluoride Debate.
See also:
Similar articles on fluoridation
Making sense of fluoride Facebook page








From the outset, Paul Connett is using a convenient sentence structure to mix the issue of fluoridation vs naturally occurring fluoride in the water:
per Paul Connett:
“I am not aware of any health agency in any fluoridated country comparing fracture rates in children in fluoridated versus non-fluoridated communities or even examining fracture rates in children as a function of the severity of dental fluorosis. Scientists did this in Mexico (Alarcón-Herrera et al., 2001) and found an increase in fractures as the severity of dental fluorosis increased (see P.169, CAF). No attempt has been made to reproduce this result or conduct a similar study in any of the fluoridated countries.”
Alarcón-Herrera’s report was on NATURALLY HIGH OCCURRING LEVELS OF FLUORIDE in the water in Mexico, NOT on optimally fluoridated. There is a distinct difference Paul.
LikeLike
I am struggling to see the difference between the two be honest Johnny Johnson. Naturally occurring or otherwise it does demonstrate the potential harm from overexposure at micro-molar levels of exposure.
and on the subject, If we were to set a base level of exposure at 0.7ppm it would take not less than one mediocre cup of tea to push the individual in questions risk of chronic exposure to fluoride into a higher risk band.
Therefore, these studies looking at higher micro-molar exposure levels are of importance to this debate.
LikeLike
I am struggling to see the difference between the two
Please allow me to be of assistance:
NATURALLY HIGH (caps in original)
vs
optimally fluoridated [levels]
LikeLike
Paul, inexplicably still keeps hanging on to the bizarre notion that these discussions should center around his non peer-reviewed book. That not going to occur, he needs to get past this and understand that legitimate science has no interest in discussing non peer-reviewed literature as if it were a valid source of scientific information.
Too, Paul needs to cease cluttering the discussion with his unsubstantiated opinions and conjecture on why this organization did this, why that person was fired, all the conspiracies occurring at this level or that, and so on and so on. That kind of irrelevant nonsense serves no useful purpose in a scientific debate such as this.
So, okay…….Where is the evidence of the disorders Paul keeps trying to link to water fluoridation? This public health initiative has been in place for 68 years. There have been tens of millions of people ingesting fluoride at the optimal level, continuously for decades.
Osteosarcoma:
“No significant association between bone fluoride levels and osteosarcoma risk was detected in our case-control study, based on controls with other tumor diagnoses.”
An assessment of bone fluoride and osteosarcoma.
Kim FM, Hayes C, Williams PL, Whitford GM, Joshipura KJ, Hoover RN, Douglass CW; National Osteosarcoma Etiology Group.
Collaborators (9)
Source
Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA.
The United States has a population of 315 million with 73% fluoridation. Given this, there should be astronomical numbers of osteosarcoma each year, were there the associations with water fluoridation that Paul so desperately keeps trying to establish. However:
“Osteosarcoma is not a common cancer. Each year, about 800 new cases of osteosarcoma are diagnosed in the United States. About 400 of these are in children and teens.”
—http://www.cancer.org/cancer/osteosarcoma/detailedguide/osteosarcoma-key-statistics
Hip Fractures:
“Overall, we found no association between chronic fluoride exposure and the occurrence of hip fracture. The risk estimates did not change in analyses restricted to only low-trauma osteoporotic hip fractures. Chronic fluoride exposure from drinking water does not seem to have any important effects on the risk of hip fracture, in the investigated exposure range.”
——Estimated Drinking Water Fluoride Exposure and Risk of Hip Fracture
A Cohort Study
P. Näsman, J. Ekstrand, F. Granath, A. Ekbom, C.M. Fored
JDR October 1, 2013
The Ever-present 27 Chinese IQ studies:
Once again………The Harvard Review was of 27 Chinese studies found in obscure Chinese scientific journals, of the effects of high levels of naturally occurring fluoride in the well water of various Chinese, Mongolian, and Iranian village. The concentration of fluoride in these studies was as high as 11.5 ppm. By the admission of the Harvard researchers, these studies had key information missing, used questionable methodologies, and had inadequate controls for confounding factors. These studies were so seriously flawed that the lead researchers, Anna Choi, and Phillippe Grandjean, were led to issue the following statement in September of 2012:
“–These results do not allow us to make any judgment regarding possible levels of risk at levels of exposure typical for water fluoridation in the U.S. On the other hand, neither can it be concluded that no risk is present. We therefore recommend further research to clarify what role fluoride exposure levels may play in possible adverse effects on brain development, so that future risk assessments can properly take into regard this possible hazard.”
–Anna Choi, research scientist in the Department of Environmental Health at HSPH, lead author, and Philippe Grandjean, adjunct professor of environmental health at HSPH, senior author
As it seems there have been no translations of these studies into English by any reliable, objective source, it is unclear as to whether they had even been peer-reviewed, a basic for credibility of any scientific study. These studies were flawed that NOTHING could be “concluded” from them.
And the “Journal Fluoride”:
“There are some periodicals that pose as peer-reviewed scientific journals but are not. One such is the journal “Fluoride.” This quarterly publication, which is also available also on the Internet, appears biased toward anti-fluoridation opinion and presents experimental work of questionable quality. Whereas their instructions to authors (found at http://www.fluoride-journal.com/papers.htm) suggest a review process, an examination of a few dozen articles reveals that the same authors appear repeatedly (and tend to cite each other) and the experimental work is poorly describe
and executed. There may be quality science aired in this journal, but ALL articles we examined have an anti-fluoride theme, and many contained significant technical or scientific errors.
For example one study (Chlubek et al., 1998) attempted to assess the fluoride levels of maternal plasma, and the marginal- and central-placentas of 30 pregnant women, ages ranging from 19 to 40 years old, living in an area with relatively low water and air fluoride (fluorine) content. They concluded that the placenta could accumulate fluoride in healthy women who are exposed in pregnancy to relatively low fluoride concentrations in water and in the air. However, an examination of their data show that in Table 1 and Table 2, they shift units between “m M/L” (a meaningless unit: it should be either m mol/L or m M) and m g fluoride/g of tissue ash (a unit that is not comparable to exposure data in their publication) makes their findings meaningless, and makes one wonder whether these workers are competent in elementary chemistry. Moreover, their study included no controls that are critical to interpreting the results as they intended.”
Impact of Fluoridation of the Municipal Drinking Water Supply:
Review of the Literature
Prepared for:
Escambia County Utilities Authority
Prepared by:
The Center for Environmental Diagnostics and Bioremediation
University of West Florid
Joe Eugene Lepo & Richard A. Snyder. May 2000
Steven D. Slott, DDS
LikeLike
Paul makes a big thing of Dr. Phyllis Mullenix,studies in 1996 but there have been similar studies done by Reddy2011
supposedly found that fluoride accumulated at very high levels in rats’ brains. The researchers used 2 groups of male rats: one experimental group, one control. There were only 6 animals in each group, which is a very small sample size. The control group supposedly received no fluoride, but then there were no data on fluoride levels in the tap water they drank or the rat chow they ate. This is a significant flaw & I’d have thought it should have been picked up by peer review.The experimental rats apparently received 20ppm fluoride by nasogastric tube for 2 months. Actually, it’s not actually clear what dose they received: the abstract says 20ppm NaF, but the methods section says “20ppm concentration of fluoride”. These are 2 different things. Either way the dose is about an order of magnitude higher than you’d find in fluoridated municipal water in New Zealand, in which case the paper didn’t really support the commenter’s assertions.And in addition, both groups of rats lost a great deal of weight during the course of the study. While the average body weight of the animals was 180g (+/-20g), after 2 months the control animals weighed on average 111g, while the experimental group was down to 93g (both +/- 2g). This strongly suggests they were either ill, or not receiving adequate food.
Michael Connett says his mice recieved 5-10PPM at 4weeks old, now that is a good dose to evaluate brain damage, they probably died of fluoride poisoning
And then he bring up our own john Colquhoun and his mate Waldbott , and we all know how credible he was, so if the mud sticks it stands to reason that the 2 of them are suspect
LikeLike
Paul says: “Yes, there are weaknesses in many of these IQ studies but the greatest “weakness” is the fact that countries that practice water fluoridation have made virtually no attempt to reproduce them or pursue the matter in any way”.
Once again,
Harvard, Columbia, Georgetown, Duke, U. of Michigan, U. of Wisconsin, Vanderbilt, U. of Minnesota, USC, UCLA, Stanford, UC-Berkeley, U. of Washington.
What do all these fine universities have in common? They are all located in fluoridated communities.
The idea that the citizens in each of these communities, including the professors and their families that live there have lower IQ’s than in non-fluoridated communities is ludicrous.
Convince me, Paul, that the similar demographics in 50+ years fluoridated Corvallis, OR are dumber than their counterparts in non-fluoridated Eugene, OR. You showed up in little Philomath, OR, spouting this IQ rubbish, and guess what? The citizens of Philomath voted fluoridation back into their public water supply despite your fearmongering.
Even Paul’s Fluoride Action Network’s world headquarters in Burlington, VT. enjoys the public health benefit of fluoridation.
Lastly, here’s a study, Paul, you can digest:
Appetitive-based learning in rats: Lack of effect of chronic exposure to fluoride
Gary M. Whitford, Jennifer L. Whitford, Stephen H. Hobbs
Neurotox Teratol (2009), doi:10.1016/j.ntt.2009.02.003
Conclusion: Chronic ingestion of fluoride at levels up to 230 times more than that experienced by humans whose main source of fluoride is fluoridated water had no significant effect on appetitive-based learning.
LikeLike
based on our replot the increases in villages 4 and 5 appear to be “real,” even though they are not statistically significant individually. This looks like an example of going back & doing a subgroup analysis when the initial analysis didn’t show what they wanted. Also, special pleading.
Reddy2011 supposedly found that fluoride accumulated at very high levels in rats’ brains. The researchers used 2 groups of male rats: one experimental group, one control. CITATION for this quote: http://sci.waikato.ac.nz/bioblog/2013/09/fluoridation-it-pays-to-read-carefully.shtml
LikeLike
Professor Connett insists that Dr. Kurt Ferré’s evaluation is mistaken and that Li’s paper raises serious concern over the effect of community water fluoridation on bone health.
6 matters come to my mind.
1. Professor Connett’s analysis of the Li paper is contrary to what the study’s authors explicitly state. Quoting from the abstract: “Water fluoride levels at 1.00-1.06 ppm decrease the risk of overall fractures relative to negligible fluoride in water.” The authors believe the skeletal effect to potentially be an important world wide public health benefit.
2. Li, et al clearly state that the “U-shaped” response curve was not present for hip fractures. This is one of the findings of the research. It does not invalidate the authors’ view that “Water fluoride levels of 1.00-1.06 ppm decrease the risk of overall fractures relative to negligible fluoride in water”
3. There were not “two parts” of this paper. Data gathered included: “. .the site (22 sites using an illustrative drawing of the human body), age, and frequency of each fracture as well as circumstances associated with the fracture, including cause (eight categories), location (six categories), ground condition, and fall or without fall.” . . .”initial analysis of bone fracture data included overall, spinal, and hip fractures since the age 20 years.” Only hip and overall fractures had sufficient numbers for analysis.
4. Professor Connett’ graph misleads. He says: “the graphs provided by Li et al (2001), including the one used by Ken, are not real plots at all.” Professor Connett believes them “only illustrative” because his graph of fluoride “dose” reveals the truth.
By careful dietary surveys and analyses Li et al showed the subjects to have no extraneous fluoride exposure from dental products, air pollution, food or tea consumption. The subject’s intake “was largely determined by the fluoride concentration of water used. The fluoride content in ambient air was negligible (,3 mg/m3) in all populations. The calculated average total daily fluoride intake was *** proportional *** to the water fluoride concentration.”
[*** – my emphasis]
Thus Professor Connett is mathematically incorrect in saying that Li’s graphs are merely “illustrative” but his graph of fluoride “dose” reveals the truth. Li’s statement that “daily fluoride intake was proportional” means that there is simply a constant multiplier relating the water fluoride concentration to estimated dosage. There are no experimentally determined factors any non-linear relationship to dose and water concentration for the various villages.
It is simply impossible to claim an important insight based on Professor Connett’s replot of Li’s data. Any apparent difference is due to different choices in the graph scaling. Professor’s Connett graph compresses the X axis and truncates and expands the Y axis compared to Li’s Fig 2. The resulting increased slope of the point plots enlarges the apparent differences between the three low fluoride villages. Whatever Professor Connett sees “more clearly” in the graph on page 172 of his book (for sale at $24.95) is due to scaling choices and not the underlying data.
5. Kurt Ferré’s complaint comes from one of Professor Connett’s “50 reasons to oppose fluoride.” The paragraph in question only addresses “Hip Fractures” and specifically of Li’s study only says: “One very important study in China, which examined hip fractures in six Chinese villages, found what appears to be a dose-related increase in hip fracture as the concentration of fluoride rose from 1 ppm to 8 ppm (Li 2001) offering little comfort to those who drink a lot of fluoridated water.”
Professor Connett makes no mention that Li found overall fractures lessened. While “rose from 1 to 8 ppm” is technically not false, the more complete truth is that only at the highest water fluoride level were hip fractures significantly greater than any of the three low to optimal fluoride levels.
6. Readers may be interested in the literature which Li cites consistent with his conclusions:
“The data appear to suggest that there may be a “beneficial window” of fluoride intake for bone health, because an increased risk of overall bone fractures was detected in both the populations with deficient and excessive fluoride in drinking water. This finding is in agreement with the results reported by a study in Germany, which found that 1 ppm of fluoride in drinking water did not influence peak bone density but may reduce the incidence of
osteoporotic hip fractures in older individuals.[Lehmann (1998)] A recent study in osteoporosis patients also suggested that low fluoride doses resulting in a moderate increase in bone mineral density (BMD) may be advantageous in terms of fracture reducing potency.[Ringe (1999)] Further investigations are warranted to confirm our findings and to define the possible beneficial window of fluoride exposure observed in the present study.”
Professor Connett’s choice of fracture category discussion, the ad-hoc creation of a visually more compelling graph, the verbal linkage of optimal fluoride to an effect present at about 13 times more water fluoride than the current target and drawing conclusions from research at odds to the author’s opinions are clear and legitimate reasons why New Zealanders should ignore his advice and listen to local professional and public health experts.
LikeLike
Thank you Billy Budd, that is helpful.
LikeLike
Mr S Slott tries to discredit science published in ‘The Journal of the International Society for Fluoride Research’ by using a quote from this paper:
Impact of Fluoridation of the Municipal Drinking Water Supply:
Review of the Literature
Prepared for:
Escambia County Utilities Authority
Prepared by:
The Center for Environmental Diagnostics and Bioremediation
University of West Florid
Joe Eugene Lepo & Richard A. Snyder. May 2000
Well goodness me, not only does the paper not appear in a peer-reviewed journal, it apparently appears in no journal at all. Non-peer reviewed and non-published. Yet earlier in Slott’s post he claims that only peer reviewed publications have scientific standing or relevance to this debate. I think that Slott’s ‘cherry picking’ is taken to an extreme that nobody else comes close to. Probably for the purposes of this interesting debate we should ignore Slott’s contributions and stick with those that have a more scientific approach to their commentaries.
LikeLike
David, I will be providing a more in-depth analysis of the journal Fluoride in my next article which will be posted tomorrow or Monday. Steve’s cynicism about the journal is well warranted.
I see nothing wrong with a report such as you quote making a judgment about the reliability of this jounral. Surely that is a responsible and intelligent thing to do – after all it is a report for people who probably do not have any expertise in the area or any experience of the journal.
Let every commenters comments stand on their merit. I personally find a lot of good material in Steve’s comments. So, come on, play the ball – not the man.
LikeLike
Sure David. Ignore my posts. They are not meant for antifluoridationists anyway. They are meant to counter the mounds of misinformation posted by antifluoridationists such that those intelligent persons who truly seek accurate information about water fluoridation will have accurate facts on which to formulate their opinion. As far as the journal “Fluoride”, take my post on that any way you wish. The content of that journal speaks for itself.
Steven D. Slott, DDS
LikeLike
Can anybody besides a dentist explain to me why their opinions should be given any scientific credibility regarding the matter of systemic ingestion of fluorides? Their credentials should be left at the door with their shoes. If you want a deck built, you contract a carpenter. If you want a toilet or sink installed, you call a plumber. If you need electrical work done, you seek an electrician. If you’re interested in how fluorides interact systemically with the chemistry of the human body and what the affect of these interactions are you seek the advice of a scientific researcher, chemist or toxicologist and not a dentist. Most dentists indocrinated with a set belief are clearly trying to preserve their own and their chosen fields reputations and credibility in light of ever increasing obviously contradicting evidential science. And yes this all comes round to whether the desired effect of fluorides on teeth is necessarily accomplished with systemic ingestion or topical application and as most authorities are of the opinion that topical application derives the primary benefit and systemic ingestion is likely to have no benefit you have to wonder why credence is given to dentists and why we’re debating this at all. Thanks to Connetts revelation, it would appear that Ken was wearing blinders when he selectively quoted from the CDC 2001, Oral Health Statement. Ken acuses of cherry picking, selective quoting and insists on playing the man but yet falls short of these virtues himself. I give Ken and Paul a lot of credit for setting this debate up, think it is an excellent forum for the expression of opposing ideas but believe it falls short in one department and that is having an impartial moderator. If this forum was moderated by Connett, I would be of the same opinion. Regardless, thank you Ken and Paul for your contributions, efforts. and hats off to all the participants!
LikeLike
Myles26
Here’s the difference between the opinions of this dentist and most antifluoridationists, including you…….I provide valid evidence for my claims. It is this evidence that I encourage readers to trust, not my opinions.
My educational background and experience give me the ability to understand the science and mechanisms of fluoridation far better than most, but, more importantly, I don’t recommend to people that they trust me because of who or what I am. I simply recommend to them to look at the valid, accurate literature, from legitimate, primary sources, and base their opinions on that, rather than on biased “information” gleaned off of antifluoridationist websites such as Connett’s own “fluoridealert.org”. I either provide direct cites of valid evidence to support my claims, or I am able to do so upon request.
Now, contrast this to your comment. You make unsubstantiated claims and provide no valid evidence to support these claims, whatsoever.
Given this, I challenge you to provide valid, scientifically acceptable evidence that:
1. “Most dentists indoctrinated with a set of beliefs are clearly trying to preserve their own and their chosen fields”
2. That there is “obviously contradicting evidential science” which is increasing.
3. That “most authorities are of the opinion that topical application derives the primary benefit and systemic ingestion is likely to have no benefit”. Who are these “most authorities” and where do they state that systemic ingestion of fluoride is likely to have no benefit?
The type of unsubstantiated claims you make here are typical of antifluoridationist tactics. If you truly care to contribute intelligently to the discussion, then provide valid evidence as support for your claims, or understand that they are entirely meaningless.
Steven D. Slott, DDS
LikeLike
Myles, you comment really adds nothing and is wrong on several counts. I will correct you one some if these.
1: This is actually a discussion between scientists, chemists, who both have a record of scientific research and are now retired. Neither of us are dentists.
2: Your classifications are mechanical and arbitrary. Maybe yow are unaware but much of the research findings relevant to this discussion occur as reports in dental, journals. As a research chemist interested in the reactions and occurrence of apatites in soils and fertilisers I often made use of the dental literature.
3: Your claims of Indoctrination of dentists are just silly. You yourself display some characteristic symptoms of indoctrination.
4: Your understanding of the various roles, systemic and surface, of fluoride in the body is opportunist. Hopefully you will learn more on this from our exchange.
5: Far from wearing blinkers it was me who bought the relevant CDC quote to Paul’s attention – and to the attention of local anti-fluoridation activists who had purposely omitted the reference to drinking water.
6:This exchange has no moderator – either me or Paul. We agreed in the basic outlines and then set to it. There is no control or censorship of articles at all. You are confusing this with the comment moderation which as the blog owner I control. Both Paul and I agreed that the usual standard of commenting on this issue was shocking and did not want that dragging down the current exchange. If you can point to me using that comment moderation in an unfair way then provide the evidence. But I stress – only the comments discussion is being moderated.
7: Finally. The discussion may not be going the way you would prefer but sneering comments like this won’t change that. As a commenter you should be trying to contribute something of substance – rational argument, evidence, corrections, etc. not simple and naive assertion. You are welcome to do so and I encourage you to do so. But please no more sneering comments.
>
LikeLike
Ken, your attitude of superiority and disdain is irritating and your assumptions and assertions way off base.
1. Your first point of which you explain the obvious does not require a dignified response. Maybe you’re tired or needed some filler to reach your quota of 7 points, I don’t know.
2. Correction, relevant to your position and subject to your interpretation much like the National Institute of Dental Research used the error proned and grossly misleading Brunelle and Carlos official analysis paper of their survey to endorse and promote their dental programs.
3. My claims of indocrination of dentists are silly but yet in the same vein Ken asserts I possess characteristics of being indocrinated. Ken, quite often opponents to water fluoridation start out as indocrinated proponents that is excepting a set of beliefs uncritically . And while I did not endorse water fluoridation, I was of the general opinion that it was good for your teeth. How could I not be with all these claims of fluoridation being one of the top 20 health achievements and more than 90 professional health organizations recognizing fluoridation as being safe. Claims that have no basis, I might add. So I was not impartial, I was partial to fluoridation being a good thing and have come full swing since looking underneath the hood of this klunker of a practice we call fluoridation. I seriously doubt dental school paints anything but a rosy picture of fluoridation.
4. While I don’t believe my understanding of the various roles of fluorides whether they be topical or systemic are opportunistic I do believe them to be inline with the CDC’s. These key sentences from your and Conettes quotes say it all. “The concentration of fluoride in ductal saliva, as it is secreted from salivary glands, is low” “This concentration of fluoride is not likely to affect cariogenic activity.” “however, drinking fluoridated water, brushing with fluoride toothpaste, or using other fluoride dental products can raise the concentration of fluoride in saliva present in the mouth 100-to 1,000-fold.” The CDC disqualifies systemic ingestion of fluoridated water as having any real impact on cavity prevention and then goes on to group fluoridated water with tooth paste and other dental products which are responsible for raising the concentration level of fluoride in saliva topically. Pretty clear cut to me. The CDC spells it out in the quote quoted by Connett. “Fluoride’s caries-preventive properties initially were attributed to changes in enamel during tooth development… However, laboratory and epidemiologic research suggest that fluoride prevents dental caries predominantly after eruption of the tooth into the mouth, and its actions primarily are topical…” (CDC, 1999).
5. I said you were wearing blinders not blinkers. Blinders are worn by horses to narrow their focus to just what’s infront of them so they don’t get distracted and become skitish. I think you made a mistake bringing this quote to Connetts attention as it has backfired on you and you have done yourself a disservice. These quotes support topical use and not systemic usage.
6. I was not confusing moderation of the debate with comment moderation. I should have been more precise when refering to comment moderation. As far as proof of you moderating comments in an unfair way in regards to deleting comments, how am I suppose to do that when I don’t have access to said deleted comments? I have know idea what you are deleting. You’re profluoride and judging by your disdain for opponents, I’m concerned with your allowance of fellow proponents personal attacks and vitriol. You commonly give them a slap on the wrist or a weak rebuke when in contrast with an opponent you delete their comment or use much stronger language. An example would be Gatsby. Many of his comments in my opinion should have been censored but were not. Your blog, your call though Ken. I do think you’re doing a fairly good job in general but do think that an impartial moderator would have removed any question of whether there were any inconsistencies in moderation.
7. How perceptions can be so completely different. I believe the debate to be going well. This debate won’t decide anything but will influence peoples opinions and decisions. While you and Connett have presented your positions, you both have not really engaged one anothers points/arguments consistently. A point by you or Connett is raised but typically left unanswered which is annoying. Maybe a moderator would have been useful in this respect as well to keep both you and Connett on track. Nature of the beast I suppose. I will refrain from making sneering comments in the future as you suggested.
LikeLike
Myles, the hostility io your comment is the very thing we are trying to exclude through moderation. You are welcome to comment here specifically about the issues raised in the articles and I urge you to do so. But future comments will be moderated to exclude the hostility and the attacks.
Even the constructive criticisms in you current comment could have been presented in a useful way
For example, you sole criticism of the exchange seems to be that we”both have not really engaged one anothers points/arguments consistently. A point by you or Connett is raised but typically left unanswered which is annoying.” Well why not press us in your comments? Demand an answers that would be helpful. You can still do so but need to be specific rather than dumping on us.
But be realistic. I myself find Connett appears to have avoided some of my points about the nature of bioapatites and the role of ingested fluoride I have continued to push him but in the end even the independent moderator you want cannot force unwilling people to perform.
Finally I think you are confused on this topical mechanism issue – many anti-fluoridation activists are. Connett has apologised for misrepresenting my position as relying on transfer of ingested F to saliva. He acknowledges I was talking about transfer of F from drinking water in the oral cavity to saliva and biofilms (although he still wants to deny it happens). I do not have the expertise to debate the significance of systemic derived F in saliva and will leave that to others – there still sees to be debate on that issue). My quotes from the CDC seem to have helped get through to Paul. They supported my position. There was no backfiring. Perhaps you should go back and read what I wrote.
These quotes support a surface mechanism for the beneficial role of fluoridated water in countering tooth decay in existing teeth. They are not talking about the beneficial role of ingested F for bone health and for pre-erupted teeth. I have referred to this in my articles but some people seem to have difficulty understanding that because they are so taken up with “topical application.”
So, you are welcome to push us on these issues and demand answers. Just no more put downs please.
>
LikeLike
Myles
One thing Connett has done is to muddy the water in terms of topical versus systemic fluoride, either intentionally in an effort to mislead, or through his lack of understanding of the role of water fluoridation in caries prevention. By attempting to make a major issue out of systemic versus topical effect of fluoridation, he ignores the effective mechanism of action of fluoridation, which lies in keeping consistent exposure of the teeth to low levels of fluoride all during the day. This has been made repeatedly clear to him, yet he still persists in attempts to equate fluoridation to the use of fluoridated toothpaste or fluoride rinses on a daily basis.
The mode of action of water fluoridation is both systemic and topical. The percentage of each is irrelevant as the preventive benefit is derived from the consistent bathing of the teeth with a low concentration of fluoride all during the day. This comes directly from the consumption of fluoridated water, drinks made with fluoridated water, and foods prepared with fluoridated water…..and systemically from incorporation of fluoride into the saliva.
From the CDC:
“Both drinking water and toothpaste provide important and complementary benefits. The drinking water provides long low-level protection, but the fluoride in toothpaste is at a high enough concentration that it has additional properties. Whether in water or toothpaste, fluoride works in two main ways: by slowing the activity of bacteria that cause decay, and by combining with the enamel on the surface of the teeth to make it stronger and more resistant to decay. Fluoride in the water, although at a lower concentration than in toothpaste, maintains a constant low level of fluoride in the dental plaque and saliva all day. Toothpaste provides a high level of fluoride, but only for 1-2 hours after brushing, so the water exposure during the remainder of the day takes over after that.”
——http://www.cdc.gov/fluoridation/fact_sheets/cwf_qa.htm#
From Buzalaf:
“Fluoride concentrations as found in dental plaque have biological activity on critical virulence factors of S. mutans in vitro, such as acid production and glucan synthesis, but the in vivo implications of this are still not clear. Evidence also supports fluoride’s systemic mechanism of caries inhibition in pit and fissure surfaces of permanent first molars when it is incorporated into these teeth pre-eruptively.”
—-Mechanisms of action of fluoride for caries control.
Buzalaf MA, et al.
Monogr Oral Sci. 2011;22:97-114. doi: 10.1159/000325151. Epub 2011 Jun 23.
Affiliation
Department of Biological Sciences, Orthodontics and Public Health, Bauru Dental School, University of São Paulo, Bauru, Brazil. mbuzalaf@fob.sup.br
Paul Connett has no healthcare education, training, or experience. He portrays himself to be an “authority” on fluoridation, yet has not one, single, peer-reviewed piece of scientific research or literature on fluoridation to his name. Those who wish to a accept his opinions as authoritative, for whatever reason, are certainly free to do so. However it must be kept in mind that in accepting his opinions on fluoridation, one is rejecting the overwhelming consensus opinion of the worldwide body of highly respected healthcare organizations, healthcare experts, healthcare providers, U.S. Surgeons General, esteemed healthcare educators, public health experts, and respected regulatory agencies….all of which fully support the public health initiative of water fluoridation.
Steven D. Slott, DDS
LikeLike
Myles. I am a ‘lurker’ Posting a few details as I can, I am not a graduate in anything, but I think Ken is doing a great job of keeping this debate on an even keel. I am quite happy lurking and learning from people who know a lot more than me
LikeLike
Yes, Louise Mantella, I have imposed moderation on Paul Melters because of his personal attacks on other commenters (and now me). That just means they don’t get approved – there is no censorship in the sense of deleting or modifying.
Bill Wilson was told that I do not get into personal email exchanges – he was commenting on a post and his comment logically should have gone there. I have urged him to make his comments in the normal way. This seems to be the only way of trying to encourage stalkers to comment normally.
If, as you assert, Melter’s science is “impeccable” then I suggest you encourage him to comment here in the normal way about the science and stop attacking other commenters. I will happily approve civil comments like that.
LikeLike
Louise
If you will notice, my comments about Connett are not personal attacks. They are statements of fact in regard to his qualifications and the information he provides. When anyone presents themselves as being an authority on anything, as Paul does with fluoride, it is completely fair to raise questions about his qualifications and claims. The fact that he, as he has done in the past and continues to do, gets offended and defensive when questions are raised about his qualifications and the validity of his book is, to me, very telling about the lack of confidence he has in his position and in his book. Others are certainly entitled to their opinion, as well, but any legitimate authority on any subject should be fully prepared to have his qualifications and claims questioned, and have the confidence in himself, his opinions, and his knowledge to withstand these questions and accept the fact that they are not only fair, but necessary.
Steven D. Slott, DDS
LikeLike
An example would be Gatsby. Many of his comments in my opinion should have been censored but were not.
You mean comments from Cedric Katesby?
I totally disagree, his comments are one of the reasons I frequent Ken’s blog.
They cut through shoddy thinking and poor methodology like a knife, and often contain a vein of humour, although I can understand those on the receiving end may feel uncomfortable. One way to avoid any flame is think harder before commenting.
LikeLike
Actually, in regard to Paul Melters, I’ve found him to be very entertaining with the webpage he has devoted to Dr. Johnson and me. It’s flattering that anyone deems our posts to be of that much importance!
Steven D. Slott, DDS
LikeLike
Roger Waters – you are just spamming – repeating the same comment under different articles. Such spamming will not be approved.
LikeLike
Myles6 – – with respect to a toxicologist’s opinion. Here is one from possibly the world’s most prestigious. He was chosen to chair the National Academy of Sciences investigation of the health effects of 4 ppm fluoride (the current maximum allowed buy the EPA).
After egregious distortions of his statements for anti-fluoridation political use he said: “I do not believe there is any valid scientific reason for fearing adverse health conditions from the consumption of water fluoridated at the optimal level.” – John Doull, PhD, Chairman of the 2006 National Research Committee report.
LikeLike