
This is Paul Connett’s response to Ken Perrott’s last article The fluoride debate: Response to Paul’s 6th article.
For Paul Connett’s original article see – Fluoride debate Part 1: Connett.
Here is my response to Ken’s last response to this thread (part 4).
Propaganda from Queensland Health
1) The pictures below appeared on page 2 of a 4-page leaflet from Queensland Health used to promote mandatory fluoridation in 2007. It compares pictures of the teeth of a child who has had its teeth “exposed to fluoridated water” (beautiful) with the teeth of a child “without exposure to fluoridated water” (atrocious).
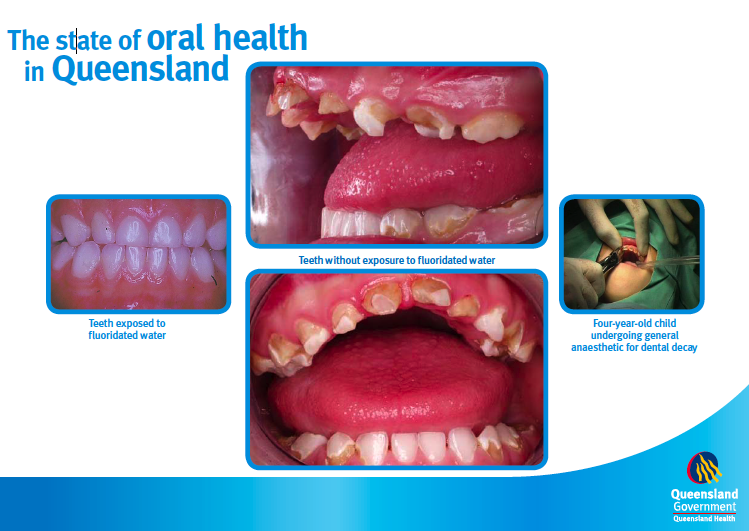
In response to this figure Ken writes:
“It seems to have been taken from a document prepared under the Queensland Health logo. I cannot find a source and no-one seems to be able to give a citation. It is not on the Queensland Health web site.” (my emphasis)
Why does Ken say “seems”? I forwarded a copy of the whole leaflet to Ken. Does he doubt the authenticity of that leaflet? I have no doubt at all about its authenticity. Mind you, I am not surprised – now that citizens in Queensland have pointed out this outrageous piece of state-funded propaganda – that Queensland Health is embarrassed and should want to hide all traces of it.
2) I think it was disingenuous of Ken to try to nullify this outrageous propaganda by providing a link to a leaflet produced by an anti-fluoridation group. The point I was making (in part 3 of this thread – originally part 1A) is that it is one thing for citizens – either promoters or opponents – to use tactics like this (I certainly do not condone or endorse any side using such tactics) but it is quite another when bureaucrats working for the state and paid by taxpayers to protect their health stoop to such tactics. It is unacceptable. Nor should it be necessary if this practice was as “safe and effective” as the promoters claim. Surely the role of civil servants is to provide objective information on a controversial issue not side with one side and then provide outrageous spin in support of that side.
3) Ken did not respond to my other concerns about the propaganda used by Queensland Health. This is less dramatic perhaps but equally deceptive. This was their claim in newspaper ads (see picture below) that there was a 65% difference in tooth decay between fluoridated Townsville and non-fluoridated Brisbane (see picture below).
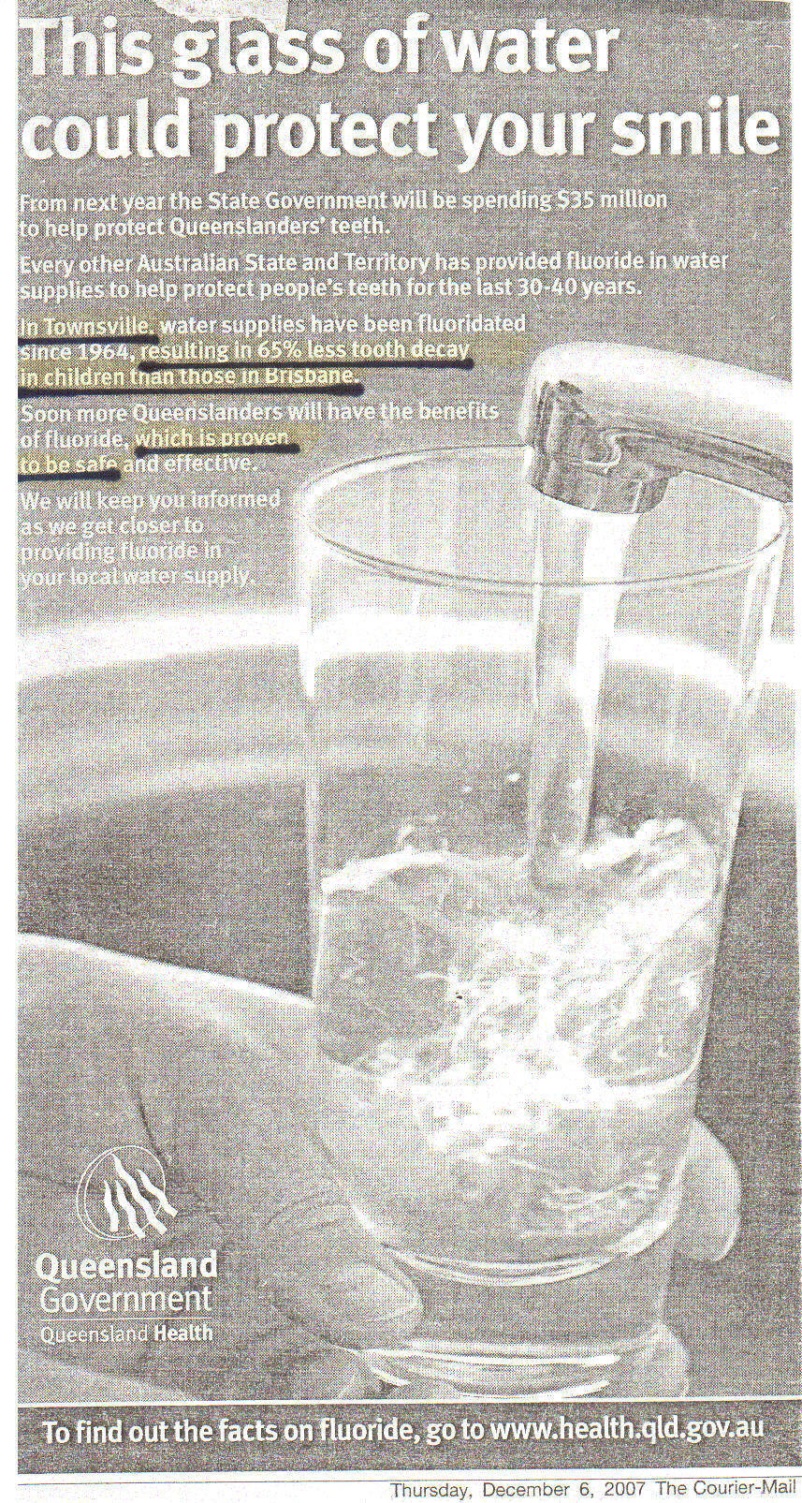
To get this 65% reduction Queensland Health had selected the number for the relative difference for just one age – 7 year olds. In Table 4 – in the paper by Slade et al., (see below) readers will see that this 65% relative reduction amounted to an absolute saving of a measly 0.17 of one tooth surface. Their arithmetic is accurate but a 65% reduction sounds a whole lot more impressive than a saving of 0.17 of one tooth surface. This is a deliberate attempt to mislead the public. In other words, it’s PR spin. I would be interested to hear how Ken would describe it.
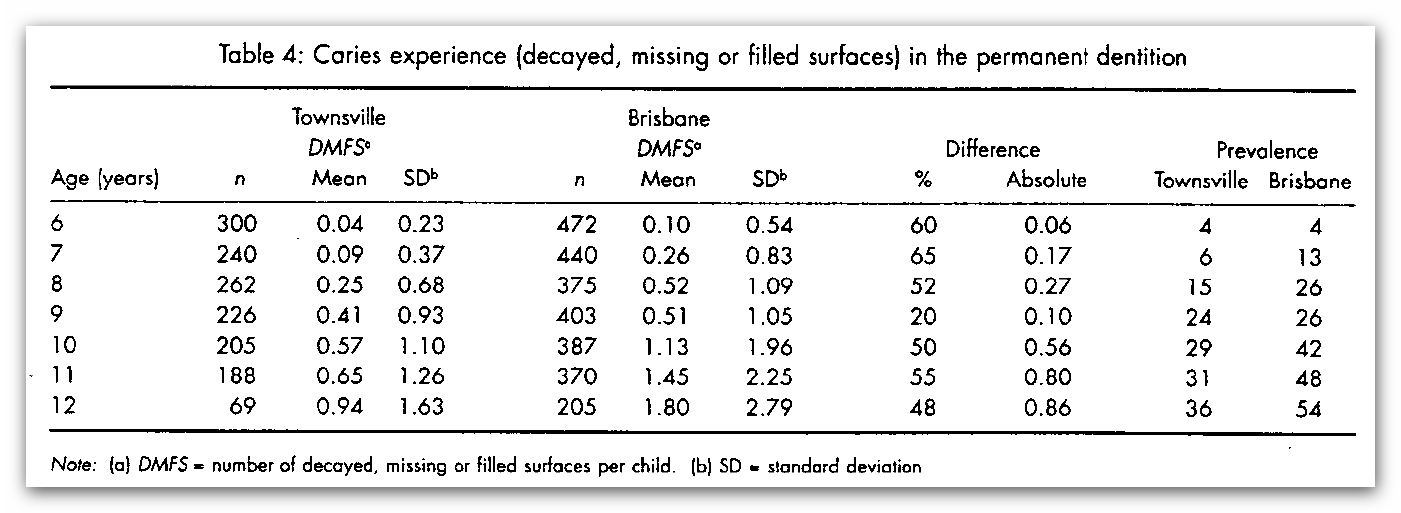
Returning to the photographs in the Queensland Health brochure, does the difference in these two sets of teeth look like a difference of 0.17 of one decayed, missing and filled permanent tooth surfaces (DMFS)?
I wish I could say that this blatant propaganda on behalf of personnel at Queensland Health is an aberration among civil servants in the health agencies of the countries practicing fluoridation. Sadly, from my personal experience, it is not.
I have seen first hand outright propaganda from people at the highest levels of civil service in the health agencies of several fluoridating countries as well as their minions in their bureaucratic chain of command.
The propaganda of these civil servants is shameless but sadly gobbled up by the media and too many local decision makers in their respective countries. One would have hoped that scientists like Ken Perrott with their sensitive antenna to scientific misrepresentation would have helped expose this sad state of affairs. Instead of doing this they fire their rhetorical guns at the citizens who are doing their very best – with limited resources – to bring this state-financed propaganda to the attention of the media, the public and their political representatives – but it is an uphill job.
4) In NZ the manipulation of the science on this practice goes back a long way – in fact to the very first trial of fluoridation in Hastings (with Napier as the control city). This trial was carried out from 1954 to 1964 and has been shown by the late Dr. John Colquhoun and his PhD thesis advisor Dr. Robert Mann and others to have been a scientific fraud (Colquhoun and Mann, 1986; Colquhoun, 1987 and Colquhoun and Wilson, 1996).
5) Ken might wish to comment on the following candid letter sent out by the Director of the Division of Dental Health, Dr. G. H. Leslie, in 1962 – some eight years into this 10-year trial.
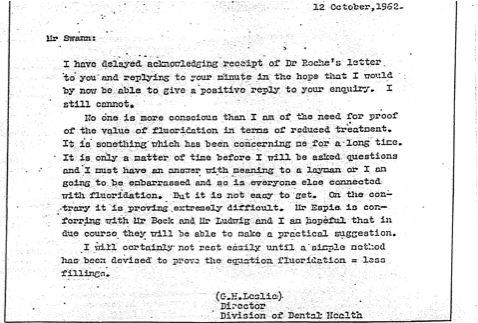
I have typed out this letter to make it easier for people to read, as some of the letters are not clear:
Mr. Swann,
I have delayed acknowledging receipt of Dr. Roche’s letter to you and replying to your minute in the hope that I would by now be able to give a positive reply to your enquiry. I still cannot.
No one is more conscious than I am of the need for proof of the value of fluoridation in terms of reduced treatment. It is something which has been concerning me for a long time. It is only a matter of time before I will be asked questions and I must have an answer with meaning to a layman or I am going to be embarrassed and so is everyone else connected with fluoridation. But it is not easy to get. On the contrary it is proving extremely difficult. Mr. Espia is conferring with Mr. Bock and Mr. Ludwig and I am hopeful that in due course they will be able to make a practical suggestion.
I will certainly not rest easily until a simple method has been devised to prove the equation fluoridation = less fillings
(G.H. Leslie)
Director
Division of Dental Health
6) With this letter we have what amounts to a “smoking gun” as far as the inability of NZ dental officials and researchers to show the effectiveness of fluoridation – some eight years into the ten-year Hastings-Napier fluoridation trial.
7) However, miraculously, two years later this trial was proclaimed as a great success at demonstrating that fluoridation had led to a large reduction in tooth decay (over 60%) and the result was used to push for fluoridation throughout the country.
8) So how in the space of two years was this dramatic turnaround achieved?
9) According to Dr. John Colquhoun’s research it was a complete artifact. The deception was in three parts. First, after about two years the control city of Napier was dropped for bogus reasons. Two, the reduction in tooth decay claimed was based on comparing tooth decay in Hastings at the beginning and the end of the trial (and not a comparison between tooth decay in Hastings and Napier). Three, method of diagnosing tooth decay was changed during the trial. Colquhoun describes this third aspect of the deception:
“The school dentists in the area of the experiment were instructed to change their method of diagnosing tooth decay, so that they recorded much less decay after fluoridation began. Before the experiment they had filled (and classified as “decayed”) teeth with any small catch on the surface, before it had penetrated the outer enamel layer. After the experiment began, they filled (and classified as “decayed”) only teeth with cavities, which penetrated the outer enamel layer. It is easy to see why a sudden drop in the numbers of “decayed and filled” teeth occurred. This change in method of diagnosis was not reported in any of the published accounts of the experiment.”
What qualifies these activities as scientific fraud, in my view, is the last sentence: “This change in method of diagnosis was not reported in any of the published accounts of the experiment.”
10) To the best of my knowledge the evidence that Colquhoun and Mann put forward for this rigged trial has never been refuted. I would be anxious to see if Ken can throw a different light on this matter. If he can’t then I think that he and other NZ citizens should be concerned that the people of NZ were duped in this way.
Ken was unresponsive to many of my other concerns expressed in parts 1 and 1A (or parts 1 and 3 in my thread, The Arguments Against Fluoridation).
11) Ken didn’t address the key issue of the difference between concentration and dose when comparing artificially fluoridated communities and naturally fluoridated study communities when harm has been identified.
12) He didn’t address the need for a margin of safety calculation when determining a safe dose for a community based on a human study that has found harm (see chapter 20 in The Case Against Fluoride…). Nor did he comment on the sample margin of safety analysis that I provided based on the Xiang et al. (2003a,b) study, although he has commented on the Xiang study elsewhere.
13) He didn’t comment on my response to his claim – that there was no need to control the dose as far as efficacy was concerned because it worked over a wide range. I pointed out that there was not a wide range as far as safety was concerned and gave this information:
“I would also remind you that when the US National Research Council reviewed the toxicology of fluoride in water they concluded that several subsets of the US population were exceeding the US EPA’s safe reference dose for fluoride (the so-called IRIS value) of 0.06 mg/kg/day. This included high water consumers and bottle-fed infants. See Figure 2.8 in their report (NRC, 2006).”
14) Ken is ducking a key issue when he writes:
“It is pointless to continue debating definitions of fluoride as a medicine – as I have said the argument is largely semantic. People who wish to pursue the argument should do so in a court of law.”
Is he suggesting that in order to get a rational response from him on this matter I have to take him to court? Joking apart, surely he can concede that the purpose of fluoridation is to treat people as opposed to treating the water to make it safe or palatable to drink? And if he is willing to concede that then doesn’t treating people – at least in some countries – require that those treated have the right to informed consent to that treatment? This is not just about semantics it is about fundamental human rights. See the definition of medicine and medical treatment under EU law which I provided in the other thread (part 6).
15) Instead of providing me with examples of statements from countries in Europe that have rejected fluoridation for reasons other than the two main ones I cited, Ken fobs me off with a statement from the NZ National Fluoride Information Service. In this statement this body gives no specific examples of countries that have not fluoridated for the reasons it – or Ken – states. So I will ask him again.
Ken please provide some evidence that countries have not fluoridated for the reasons you have given as opposed to the reasons I have given, namely: they do not wish to force fluoridation on people who don’t want it and they argue that there are unresolved health concerns about the practice.
16) When Ken restates that:
“For the vast majority of people who have dental fluorosis (recognised by a professional) it is usually classified as “questionable” or “mild.” Real health concerns should only be raised for severe dental fluorosis. Yet anti-fluoride activists lump all those grades together and pretend that dental fluorosis is a much bigger problem than it really is.”
Ken has essentially ignored all the information I provided for him on this issue. I provided the figures cited by the CDC (2010) for dental fluorosis for children aged 12 to 15 in the US. In this report, they indicate that very mild dental fluorosis impacts 28.5% and mild dental fluorosis impacts 8.6% of the population in question. Mild dental fluorosis affects up to 50% of the tooth surface and presents potential psychological problems for young teenagers. Ken may not consider that a “real” problem but many teenagers do. Ken might also be interested to know that Trendley Dean, the so-called father of fluoridation , who developed this first classification of dental fluorosis in the 1930s, in testimony before the US Congress stated that mild dental fluorosis was an unacceptable trade-off for reduction in tooth decay (see chapter 11 in The Case Against Fluoride…).
Moreover 3.6% of US children aged 12-15 have dental fluorosis in either the moderate or severe category. In these categories 100% of the enamel of the impacted teeth is impacted. Neither of these categories is desirable. 3.6% of all the children aged 12-15 in the US is a lot of children!
17) Ken also claimed that there was practically no difference in dental fluorosis prevalence between fluoridated and non-fluoridated communities. He ignored my response. I cited the study by Heller et al (1997), which clearly showed that that was not the case. They found that as the fluoride levels rose from a) less than 0.3 ppm, to b) 0.3 to 0.7 ppm , to c) 0.7 – 1.2 ppm and then d) above 1.2 ppm there was a marked increase in dental fluorosis rates.
18) I offered an animal study (Varner et al, 1998) in which rats were exposed to 1 ppm fluoride (administered either as AlF3 or NaF) for one year and experienced harmful effects. I provided this reference because Ken stated that he paid no attention to animal studies performed at high concentrations and that was all he was offered by opponents of fluoridation. However, I got another brush off from Ken. He claimed that he couldn’t find the whole study by Varner et al – only the abstract – and after a few words on the abstract then stated, “I won’t comment further on this.” First, of all I am surprised that no University in the Hamilton area carries the journal Brain Research where the Varner paper appeared. Also if Ken was having trouble finding this all he had to do was email me and I would have forwarded him a pdf copy of this paper. For future reference I would be happy to do that for all the papers I cite.
19) Nor did Ken respond to the discussion in which I pointed out that the US Food and Drug Administration classifies fluoride for ingestion as an “unapproved drug.” This means that in the U.S. fluoride intended for ingestion has never been subjected to the double blind randomized control trials (RCT) for efficacy that are required of all other drugs. Nor is the FDA tracking side effects from patients or doctors, despite the fact that many individuals claim to be highly sensitive to fluoride’s toxic effects. The same professional and regulatory neglect appears to have occurred in all other fluoridated countries, including New Zealand.
Note: I have raised more specific questions about this professional and regulatory neglect in my latest response (part 6) in the other thread.
20) Ken claimed (in part 2 of this thread) that there was no difference between naturally fluoridated water and artificially fluoridated water and I responded in part 3 that:
“Usually when fluoride occurs naturally in the water it is accompanied by large concentrations of ions like calcium. The presence of the calcium can reduce the uptake of fluoride in the stomach and GI tract. No such protection is offered when the fluoridating chemicals are added to soft water.”
Ken did not acknowledge this important difference.
21) In my response (part 3 of this thread) I wrote:
“In my opening statement I singled out three subsets of the population that shouldn’t be getting fluoridated water: bottle-fed babies, people with poor kidney function and people with outright or borderline iodine deficiency. Ken chose not to comment on the latter two groups. In my view we should be concerned about both groups whether they are drinking naturally occurring fluoride or artificially fluoridated water.”
For the second time Ken chose not to respond to these concerns. Ken is certainly very sensitive to the treatment of low-income families because of his own personal history but he seems not to be as sensitive to the fate of these subsets of the population.
22) Ken chose not to respond to this question:
“Is it not reckless then to knowingly expose the bottle-fed baby to 175-300 times more fluoride than the breast-fed baby? Especially, when we know that fluoride can harm at least one developing tissue in the baby – the growing tooth cells – at very low levels and cause the condition known as dental fluorosis. What makes us believe that while the fluoride is damaging processes in the growing tooth it is not doing the same to the growing bone. After all the teeth grow out of the bone.”
23) Ken chose not to respond to the following information:
“Even when some warning signals emerged during the early trials they were cavalierly ignored by those hell-bent on promoting this practice. For example, when Schlesinger et al., 1956, published the results of the Newburgh-Kingston trial in 1956 they reported that young girls in the fluoridated community were menstruating 5 months earlier on average than the girls in the non-fluoridated community, and that the young boys were experiencing about twice as many cortical bone defects in the fluoridated community compared with the non-fluoridated community. However, no follow-up studies were recommended (see Chapters 9 and 10, The Case Against Fluoride…). These red flags were ignored then just as the studies indicating a lowering of IQ associated with fairly modest levels of fluoride exposure, are being ignored or downplayed by proponents today.”
24) Ken chose not to respond to Dr. Hardy Limeback’s discussion of possible ways that fluoride can interfere with normal bone growth:
“Bone can ACCUMULATE up to 2500 ppm fluoride with fluoridation (we showed that in our Toronto vs Montreal study). The osteoclast cells are exposed to these huge concentrations (because they dissolve bone keeping the dissolved mineral under their dorsal surface through the use of hemidesmosome attachments and then they release that dissolved mineral into the bone extracellular fluid where nearby osteoblasts can also be exposed). In fact one of the theories why there is apoptosis of osteoclasts is the poisonous conditions they have to endure remodeling bone. It is also the reason there is a biologically-supported rationale for the bone cancer inducing effects of fluoride (personal correspondence, Nov 1, 2013).”
Now I will attempt to respond to some of the issues that Ken did comment on.
25) I agree with Ken that I was a little hasty in dismissing the Irish data comparing tooth decay in the Republic of Ireland and Northern Ireland. However, the larger point I was making was this: if indeed it is legitimate to compare these two populations (and there are both cultural and genetic differences) then the more urgent need is to compare the status of various health concerns – which may or may not be caused by or exacerbated by fluoride – between the two countries. However, even though fluoridation has been mandatory in the Republic since 1963, the health authorities there have not attempted a single study comparing the health of communities which are fluoridated and non-fluoridated, either within the Republic itself or between the Republic and the North. Like most fluoridated countries (including NZ) they are flying blind on health concerns.
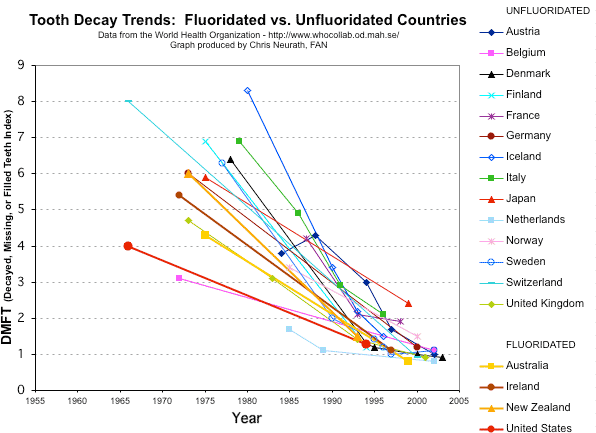
26) I think the value of comparing tooth decay between countries is to note that tooth decay rates have been coming down in both fluoridated and non-fluoridated countries at similar rates. Avid promoters of fluoridation such as the Oral Health Division of the CDC often forget this and try to claim that fluoridation has been coming down in fluoridated countries because of fluoridation when similar declines have occurred in non-fluoridated countries over the same period. See the CDC’s ridiculous Figure 1 in CDC (1999), (see figure below) which purports to show that tooth decay in 12-year olds has come down in the US over the period 1960s to the 1990s because over the same period the percentage of the US population drinking fluoridated water has increased!
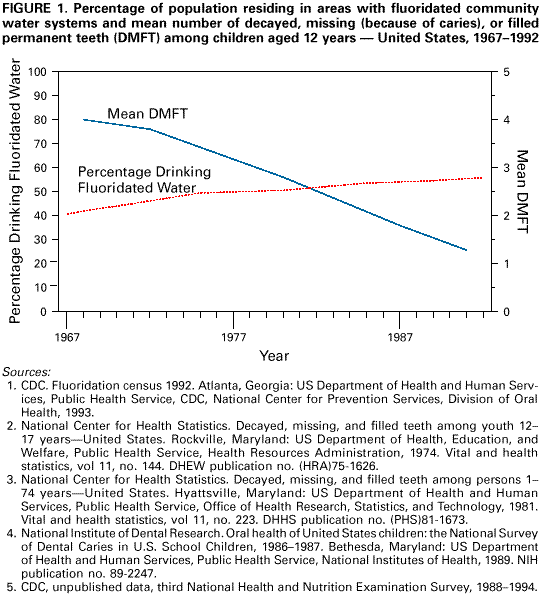 I urge readers to compare this CDC figure with the figure summarizing the decline in tooth decay in many different countries – both fluoridated and non-fluoridated countries – covering the same period (and beyond) cited by the CDC.
I urge readers to compare this CDC figure with the figure summarizing the decline in tooth decay in many different countries – both fluoridated and non-fluoridated countries – covering the same period (and beyond) cited by the CDC.
27) I agree with Ken that whenever we cite the CDC (1999) statement that fluoride’s predominant mode of action is topical not systemic we should not omit the word predominant. I usually do this. He found one example when I didn’t.
28) I have conceded in another post that I was wrong in suggesting that Ken believed that the delivery of fluoride’s topical effect was via the saliva generated in the salivary gland. However, if Ken rules out a significant role for the fluoride delivered by the salivary gland, and instead that the topical action is delivered directly in the mouth, why are we forcing people to swallow fluoridated water at all? Especially adults where no tooth development is involved once their teeth have erupted? Why instead, is he not merely advocating swishing and spitting out fluoridated water, or fluoridated mouthwash or using fluoridated toothpaste.
30) In challenging Ken’s notion that the only animal studies we quoted had very high fluoride levels. I responded that it was well known that you needed to treat rats with 5 to 10 times as much fluoride to reach the same plasma levels as humans. Ken responded by pointing out he could find only one reference to this and cited the NRC (2006) commentary on Dunipace’s work (Dunipace, 1995). The NRC characterized Dunipace’s conclusion as showing that “rats require about five times greater water concentrations than humans to reach the same plasma concentration.” (Appendix D, p. 442). However, there are several other studies that have suggested the same or even a higher ratio than 5 is needed.
Sawan (2010) explains why he used 100 ppm in his animal experiment as follows:
“However, while the fluoride concentration used in the present could be considered relatively high for rodents (100 mg/L or ppm), this concentration was chosen because it produces plasma fluoride levels that are comparable with those commonly found in humans chronically exposed to 8mg/L of fluoride in the drinking water, which is a concentration known to cause severe fluorosis.”
That is a ratio of 12.5.
Also Angmar-Månsson and Whitford (1982) pointed out to produce enamel fluorosis in rats one needed a concentration of 10 to 25 ppm fluoride (compared to the 2 ppm needed in humans). So that means you need a ratio of 5 to 10+ more fluoride to get the same result in rats as humans. Here is the quote:
“It is well known that, in fluoridated drinking water studies with rats, a water fluoride concentration of 10 – 25 ppm is necessary to produce minimal disturbances in enamel mineralization. Because of the higher water concentrations required, the rat has been regarded as more resistant to this adverse effect of fluoride. However, when the associated plasma levels are considered, the rat and the human appear to develop enamel fluorosis at very nearly the same fluoride concentrations.”
I would also point out that, in addition to the extra amount needed to reach the same plasma levels in humans, the NRC pointed out in their 2006 report that rats need at least 10 times more fluoride than humans to reach the same bone fluoride levels. To quote:
” …values support a rat-to-human conversion factor for bone fluoride uptake of at least an order of magnitude.” (Appendix D, p. 445)
Dr. J. William Hirzy.
31) Ken uses dentist Steve Slott to categorize Dr. Hirzy in the following manner, “Hirzy is a long time avowed antifluoridationist and is employed by Connett as the paid lobbyist for Connett’s antifluoridationist group, FAN.”
Clearly this comment from Slott, “an avowed profluoridationist,” is meant to throw doubt on the credentials and integrity of my colleague Bill Hirzy. I have known Bill for over 15 years. I first met him when he was working at the US EPA. At that time he and other professionals at the EPA were very concerned about the way that administrators in this agency felt that it was OK to force professionals to “bend their science and their statements” to fit into their policy judgments.
This concern began in 1985 when a scientist at the EPA admitted that he had been forced to go along with a determination that the safe MCL for fluoride was 4 ppm, when he knew that this level wasn’t safe. This professional and others at the EPA knew that the administrators were bowing to political pressure from politicians (e.g. Strom Thurmond) in certain states with areas of high natural fluoride and who were concerned that if a lower level was set for the MCL it would cost their states a lot of money to remove the fluoride.
As a result of this Dr Robert Carton and others set up a union at the EPA headquarters in an attempt to get a code of scientific integrity adopted at the EPA. This would forbid administrative staff from forcing scientists to make false statements about their scientific findings in order to fit into the “policy” of administrators. This same union after examining the scientific evidence came out in strong opposition to the so-called safety of the MCL and the MCLG for fluoride, both of which had been set at 4 ppm, and also the practice of water fluoridation.
Those who are interested can view Dr. Hirzy’s statement before a Senate subcommittee in the US Congress in 2000 (http://fluoridealert.org/fan-tv/hirzy/ ). Clearly, Bill’s opposition to fluoridation is science-based. Moreover, in a democracy like the US, like any other citizen, including Steve Slott, he is entitled to his opinion on a public policy issue like this, without being treated like some paid hack.
When Bill retired from his teaching position, Fluoride Action Network was only too happy to have such a qualified person work as our point person in Washington, DC. We have paid him a nominal salary to do this. That shouldn’t be used to suggest that he has somehow thrown science and his integrity out of the window, which I think Slott meant to imply when he says Bill is a “paid lobbyist for Connett’s antifluoridationist group, FAN.” Based on the science Bill is opposed to fluoridation. Based on the science FAN is opposed to fluoridation. It is a shame that Slott should think – or intimate – otherwise.
As far as lobbyists are concerned I think Steve would do better to wonder what the ADA is doing with 20 paid staff in DC, all of which are receiving a remuneration, which makes Bill’s nominal salary look like a pittance. One of the things that ADA is doing with its $100 million budget is to try to persuade Congress and state health departments not to allow dental therapists to perform basic dental procedures in low-income areas. Ironically, I believe that Steve is against the ADA’s position on this sensible and cost-effective measure. It has proved most successful in NZ.
In my view Bill Hirzy is an excellent educator on this and other issues. We believe that he can help with a lot of education in Washington, DC, not just with legislators but with the city council and with environmental and other public interest groups. A lot of people in DC respect both his experience and his integrity.
Here is the link to Bill’s correction of the errors in his arsenic paper:
32) Finally, I attach Dr. Hirzy’s response to Ken’s comments on his input in part 3 of this thread:
In a paragraph headed in bold type Perrott cites my activism as reason to question my ability to properly assess risks. I freely admit making an error (soon to be rectified by publication of a corrigendum) in the annual cancer incidences for HFSA and pharmaceutical sodium fluoride. That said, nevertheless EPA did not find fault in my determination that HFSA causes about 100 times more cancer than pharmaceutical sodium fluoride. Neither does Perrott show any fault in that determination.
Perrott comments about my dismissal of NSF’s statement about their testing allegedly proving the amount of arsenic contributed by HFSA is non-detectable and perfectly safe, but he fails to address my observation that NSF in fact reports measurable amounts of arsenic contributed by treatment chemicals, and that those levels lead to 200 times higher cancer risk than USP NaF. In a debate one should address points raised by one’s opponent – if one can…..
After doing some calculations based on the New Zealand Specific Impurity Limit for arsenic, I do admit that the New Zealand standard is superior by a factor of 2.4 to that of NSF. That is, however, faint praise in that it allows about 500 fold higher lung/bladder cancer incidence than pharmaceutical grade sodium fluoride. See below.
Regarding the arsenic levels in HFSA and Mr. Perrott’s being “suspicious” about my results and whether the HFSA samples I reported on were representative, Mr. Perrott cites the Brown et al. 2004 publication in the Journal of the American Water Works Association and kindly provided a link to the article. If he had read that article closely he would have noticed the support for my work on page 118. At page 118 of that piece, Brown et al. report testing 4 samples of HFSA, rejecting one because of excessive free HF, and finding arsenic levels of 9, 20 and 47 mg/kg, in the other three samples, all of which values fall within the range of the 33 samples I cited in my statistical analysis of arsenic levels in HFSA. Further on page 118, Brown et al. cite results from Weng et al. reporting on an unstated number of HFSA samples, finding an average of 28 mg/L and a maximum of 60 mg/L of arsenic – again within the range of my analysis. Finally, also on page 118 is citation of work by Casale, who found a range of 9.4 to 58.5 mg/L of arsenic – within the range of my analysis.
Concerning activism and suspicion, perhaps Perrott is correct in asserting that higher purity HFSA is available in New Zealand, but his activism in promoting fluoridation could raise parallel suspicion about that.
Perrott dismisses as “a silly conspiracy theory” my recitation of data published by the U.S. Geological Survey (USGS) showing that 94% of the byproduct HFSA produced by phosphate manufacturers in 2011 was sold to water fluoridation systems, and coupled with solid data on sales prices, produced about $560,000,000 in revenues for those companies. If only 6% of HFSA found alternative markets, which USGS found to be valued by the producers at nearly double the value for the fluoridation market, where else would HFSA go than down our shower drains and toilets, etc. Pretty good business model for a “silly conspiracy” I’d say.
My citation of the violation in Wellington, Florida was the only one I knew about. How many more there may be/have been, who can tell? And why are HFSA producers not routinely supplying certificates of analysis for every batch sold rather than simply stating “Complies with NSF/ANSI Standard 60.”
What New Zealand Might Otherwise Do (Based in part on Standard for the Supply of Fluoride for Use in Water Treatment – Second Edition. New Zealand Water Supply and Disposal Association. 1997)
Assume density of 20% assay HFSA is 1.2 g/mL (density of 24% assay is 1.24g/mL).
Pure HFSA is 79% w/w fluoride
1 mL of HFSA x 1.2 g/mL x 0.20 x .79 = 0.190 g F/mL HFSA = 190 mg F/mL HFSA
Assume need to add 0.50 mg F/L H2O
0.50 mg F/L H2O ÷ 190 mg F/mL HFSA = 2.6 x 10-3 mL HFSA/L H2O
2.6 x 10-3 mL HFSA/L H2O x 1.2 g HFSA/mL HFSA = 3.2 x 10-3 g HFSA = 3.2 x 10-6 kg HFSA/L H2O
SIL for As = 132 mg As/kg HFSA
1.32 x 102 mg As/kg HFSA x 3.2 x 10-6 kg HFSA/L H2O = 4.2 x 10-4 mg As/L = 0.42 ug As/L
Using the USEPA modified population Unit Risk value of 3.5 x 10-5/(ug As/L), a risk for lung/bladder cancer of 1.5 x 10-5 obtains. This is equivalent to 15 extra cancers per million population exposed for 70 years.
If 4 million people have been exposed at this level for 20 years, one would expect about 17 extra cancers to have developed.\
New Zealand’s SIL for arsenic is about 2.4 times more protective than the U.S. standard.
If pharmaceutical grade NaF had been used for this same period, delivering 0.00084 ug As/L, then New Zealand’s 4 million people exposed for 20 years may have developed about 0.03 such cancers.
If the New Zealand government were to have provided 4 million people with 2 L/day of water containing 0.50 mg added fluoride from pharmaceutical grade NaF for 20 years (and it is very likely that far fewer than 4 million would have opted to drink that water), it would have spend, in constant 2001 U.S. dollars, about $190,000.
If HFSA had been purchased at about half the price charged in the U.S., i.e $800/metric ton over that same period, and assuming New Zealanders use half as much water per capita as U.S. citizens, i.e. 50 U.S. gallons/day, and this practice ran for 20 years, then about $6,000,000 would have gone to phosphate producers.
And assuming it costs half as much in New Zealand to treat the cancers HFSA’s arsenic load produced, then an additional $30,000,000 would be spent on medical costs.\
So, if you are really determined to offer fluoridated drinking water to New Zealanders, you would be well advised to consider the substantial cost savings you would realize by providing free containers of water fluoridated with pharmaceutical grade NaF just to those who want it, while acceding to the demands of your citizens who most vehemently do not want fluoride in their drinking water.\
And, by the way, the New Zealand Lung and Bladder Cancer/Fluoridation Lottery could be cancelled too.
Postscript. This will be my last contribution to this thread. I feel that I have presented my case fully in the book I co-authored (The Case Against Fluoride…). What I am more interested in now – having outlined some basic arguments against fluoridation in this thread (few of which have been satisfactorily rebutted) – is seeing what scientific case Ken can produce for fluoridation. This is meant to be the substance of the other thread and that is where I will now focus my efforts.
In this respect I have been disappointed in Ken’s ability – after four attempts to do so –including the last installment that he published yesterday (Dec 10) – to lay out a scientific case. So far Ken seems more adept at theorizing on why drinking fluoride should work rather than providing the studies that it actually does. In addition, he spends more time demonstrating his disdain for anyone opposed to fluoridation than actually producing the science which shows that fluoridation is “safe and effective” as proponents repeatedly claim. Finding fault with me or other opponents does not establish a case FOR fluoridation. It is a practice forced on millions of people that don’t want it. He defends this practice and as such it his obligation to present a scientific case FOR fluoridation and I am still hoping that he will do that.
Let me be more specific: what I had hoped to see by now is:
a) What primary scientific research Ken has read that gives him the confidence that the epidemiological evidence is overwhelmingly in favor of fluoridation providing a significant benefit over and above the use of fluoridated toothpaste.
b) What his response is to the latest news from Scotland that a simple and cost-effective strategy has been devised that has been found to combat tooth decay in low-income children which does not involve forcing people to swallow fluoride who don’t want to.
c) A presentation of a weight of evidence analysis that would allow him and other promoters to dismiss all the concerns I have raised about fluoride’s impact on the brain and several other tissues. We have presented this case in our book and again in both these threads. Our case is in black and white and documented, where is his response in black and white and documented?
In the process of doing this I would particularly would like to see him identify papers that have been conducted in NZ (or Australia for that matter), which have examined any of the health issues discussed in our book, or that have collected fluoride exposure levels in the urine, blood or bones of NZ citizens to gauge their exposure to fluoride both in the short-term or long-term. In other words I am anxious to find out:
a) the scientific basis for his confidence in the safety of water fluoridation;
b) the argument he would raise to support the notion – despite so many unknowns – that the practice does not violate the Precautionary Principle (see chapter 20 in our book and Tickner and Coffin, 2006), and
c) the basis for his confidence that there is an adequate margin of safety (see chapter 21 in our book) to protect everyone in a large population drinking fluoridated water – especially the most vulnerable – from any harmful effect.
I will continue to pursue his response to these challenges in the other thread: Ken’s Arguments For Fluoridation.
References
Angmar-Månsson B, Whitford GM. (1982). Plasma fluoride levels and enamel fluorosis in the rat. Caries Res. 1982;16(4):334-9.
CDC (1999). Centers for Disease Control and Prevention, “Achievements in Public Health, 1900–1999: Fluoridation of Drinking Water to Prevent Dental Caries,” Mortality and Morbidity Weekly Review 48, no. 41 (October 22, 1999): 933–40, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4841a1.htm
CDC (2010). Beltrán-Aguilar, D et al., Prevalence and Severity of Dental Fluorosis in the United States, 1999-2004. MMWR, 53; November. http://www.cdc.gov/nchs/data/databriefs/db53.htm
Colquhoun J. and R. Mann (1986). “The Hastings Fluoridation Experiment: Science or Swindle?” The Ecologist 16, no. 6: 243–48.
Colquhoun, J (1987). “Education and Fluoridation in New Zealand: An Historical Study,” Ph.D. diss., University of Auckland, New Zealand.
Colquhoun J. and B. Wilson (1999). “The Lost Control and Other Mysteries: Further Revelations on New Zealand’s Fluoridation Trial,” Accountability in Research 6, no. 4:373–94.
Connett, P., Beck, J and Micklem HS. The Case Against Fluoride. Chelsea Green, White River Junction, Vermont, 2010.
Dunipace AJ, et al. (1995). Effect of aging on animal response to chronic fluoride exposure. Journal of Dental Research 74(1):358-68.
Heller KE, et al. (1997).“Dental Caries and Dental Fluorosis at
Varying Water Fluoride Concentrations,” Journal of Public Health Dentistry 57, no. 3: 136–43.
Hirzy (2000). Video. http://fluoridealert.org/fan-tv/hirzy/
NRC (2006). Fluoride in Drinking Water: A Scientific Review of EPA’s Standards (2006) http://www.nap.edu/catalog.php?record_id=11571
Sawan RM, et al. (2010). Fluoride increases lead concentrations in whole blood and in calcified tissues from lead-exposed rats. Toxicology 271(1-2):21-6.
Schlesinger ER, et al. (1956) “Newburgh-Kingston Caries-Fluorine Study XIII. Pediatric Findings After Ten Years,” Journal of the American Dental Association 52, no. 3: 296–306.
Slade, G.D., A.J. Spencer, et al. (1996). “Caries experience among children in fluoridated Townsville and unfluoridated Brisbane.” Aust N Z J Public Health 20(6): 623-9.
Tickner, J and M. Coffin (2006). “What Does the Precautionary Principle Mean for Evidence-Based Dentistry?” Journal of Evidence Based Dental Practice 6, no. 1: 6–15.
Varner et al. (1998).“Chronic Administration of Aluminum-Fluoride or Sodium-Fluoride to Rats in Drinking Water: Alterations in
Neuronal and Cerebrovascular Integrity,” Brain Research 784, no. 1–2: 284–98.
Xiang, Q et al. (2003a) “Effect of Fluoride in Drinking Water on Children’s Intelligence,” Fluoride 36, no. 2 (2003): 84–94, http://www.fluorideresearch.org/362/files/FJ2003_v36_n2_p84-94.pdf
Xiang, Q et al.(2003b), “Blood Lead of Children in Wamiao-Xinhuai Intelligence Study” (letter), Fluoride 36, no. 3 (2003):198–99, http://www.fluorideresearch.org/363/files/FJ2003_v36_n3_p198-199.pdf
Anyone wanting to follow the debate and/or check back over previous articles in the debate can find the list of articles at Fluoride Debate.
See also:
Similar articles on fluoridation
Making sense of fluoride Facebook page








For anyone reading internationally that’s perhaps mildly interested in the Naper – Hastings study that Prof Connett attributed 7 separate points to…
Napier are Hastings are within a short geographical proximity but they have few socio-economic comparisons which makes the idea of setting one as a ‘control’ against the other as practically useless. Using Napier as a control and trialing a public health intervention in Hastings would be similar to using Upstate New York as a control and trialing in Baltimore.
Here’s just come of the confounding factors…
differences in households income
differences in employment levels
differences in population per household
differences in numbers of ethnic minorities (indigenous population)
there’s quite a substantive list of reason why socio economic factors make this comparison useless however i have seen FANNZ use the same shaky statistical nonsense to ‘compare’ Christchurch with Dunedin.
When i’m in New Zealand I leave my chocolate bar OUTSIDE and it stays solid… when i’m in Australia and i leave my chocolate bar INSIDE it still MELTS!!
OBVIOUSLY LEAVING YOUR CHOCOLATE OUTSIDE MAKES NO DIFFERENCE TO WHETHER OR NOT IT WILL MELT!! <— FANNZ logic.
LikeLike
Ken, I wouldn’t bother. Once you start responding to these idiotic exercises in endless sideshows and lolly scrambles you will always look to be in the defensive. “Gish galloping” I believe they call it. Typically the so called “studies” are remote in time and space and involve atypical doses on rodents or comparisons of populations too disparate to be credible. We have enough data within our own country now to make an informed decision. When the aggregate benefits are compared with possible harms given the cultural and economic diversity in our country, fluoridation wins hands down. The science supports it, the epidemiological evidence supports it and so does my personal experience and the experience of most families I am familiar with.
LikeLike
Once again, Paul seeks to flog the same horse…..”fluoride is a drug”. Enough said about that nonsense, Paul. Your opinion is all you have there, and it doesn’t stand up in court or anywhere else except in the minds of antifluoridationists desperate to fine something, anything to hold against this public health initiative. Give it a rest.
The conspiracy nonsense persists. Give that a rest, too, Paul, it’s way past being tiresome and is totally irrelevant.
Your book, “The Case Against Fluoride, which you seem to think is a valid scientific reference, has not been peer-reviewed, and is not a valid reference for anything. You may as well cease trying to pass it off as such. If you want credibility, do as do legitimate scientists, perform some legitimate research, and submit for peer-review and publication is a respected scientific journal……the journal “Fluoride” not qualifying as such.
Your references to disorders……where are these disorders about which you have been fear-mongering for years, Paul? Over 6 decades of water fluoridation has shown none of them.
Hirzy, your FAN paid lobbyist, …….the EPA pretty much put his credibility to rest with their refute and rejection of his petition. That you want to continue to accord him credibility is up to you…..you hang with Mercola, and Alex Jones, so, I suppose it’s no great surprise that you would continue to accord your man Hirzy credibility. What a cast of characters!!
Steven D. Slott, DDS
LikeLike
Ken, I fully agree with Stuart. Connett is simply going around and around in the same circles. You’ve more than adequately answered and refuted all of his “points” and provided more than enough valid information on which NZ can base a proper decision. Continuing to ride Paul’s merry, merry-go-round is pointless.
Steven D. Slott, DDS
LikeLike
I cant understand why Paul keeps quoting the flawed studies from Colquhoun http://www.dentalwatch.org/fl/newbrun.html read for yourself
LikeLike
This will be my last contribution to this thread. I feel that I have presented my case fully in the book I….
Ha ha ha ha ha ha ha.
🙂
“This will be my last contribution to this thread. I feel that I have presented my case fully in the book I co-authored (We Never Went to the Moon: America’s Thirty Billion Dollar Swindle ). What I am more interested in now – having outlined some basic arguments against NASA ever having made it to the moon in this thread (few of which have been satisfactorily rebutted) – is seeing what scientific case Ken can produce for us having made it to the moon.”
“This will be my last contribution to this thread. I feel that I have presented my case fully in the book I co-authored (Callous Disregard: Autism and Vaccines: The Truth Behind a Tragedy ). What I am more interested in now – having outlined some basic arguments against vaccines (few of which have been satisfactorily rebutted) – is seeing what scientific case Ken can produce for vaccines.”
“This will be my last contribution to this thread. I feel that I have presented my case fully in the book I co-authored (Darwin’s Black Box). What I am more interested in now – having outlined some basic arguments against evolution (few of which have been satisfactorily rebutted) – is seeing what scientific case Ken can produce for evolution.”
Nobody but a moron would be interested in your crappy book.
Get thee hence to the scientific arena.
Enter it.
Defend your notions where it counts.
Peer-reviewed science and lots of it.
Any snakeoil merchant can write a vanity press book and appeal to the Dunning-Kruger Effect within addled graduates of the University of Google.
It won’t do.
Less talky-talky and more worky-worky.
Science Works! How the Scientific Peer Review Process works
LikeLike
Paul wants to continue to attempt to make mild dental fluorosis into a major, face deforning, debilitating disorder. It is not. Paul is not a dentist, and hasn’t the education, training, or experience to understand dental fluorosis. After 32 years of practicing dentistry in a fluoridated community surrounded by fluoridated communities, I have as yet to see one single case of mild dental fluorosis, in any manner attributable to fluoridated water, that could even be noticeable outside of close examination in my dental chair. Anecdotal, certainly, but anecdotal from a dental professional who treats thousands individuals from all walks of life, yearly.
Dfrom the American Dental Association:
“Enamel fluorosis is not a disease but rather affects the way that teeth look. In the vast majority of cases, enamel fluorosis appears as barely noticeable faint white lines or streaks on tooth enamel and does not affect the function or health of the teeth. In fact, in many cases, the effect is so subtle that, usually only a dental expert would notice it during an examination. Enamel fluorosis occurs only when baby and permanent teeth are forming under the gums. Once teeth break through the gums, they cannot develop enamel fluorosis.”
——http://www.ada.org/5172.aspx?currentTab=2
Paul has, on his website “fluoridealert.org”, a picture of teeth with large, white spots, brown stains, and pitting. Either he, or some equally unqualified person on his staff, has this photo labeled “mild dental fluoosis”. This is beyond absurdity, yet is a clear example of what Paul considers to be “mild dental fluorosis”. Staining and pitting do not occur with mild dental fluorosis, nor do large, very noticeable white spots, as have occurred on the teeth in his photo. This is photo depicts a classic case of moderate to severe dental fluorosis, effects who do not occur as a result of water fluoridated at the loptimal level.
For any who are interested in seeing an accurate depiction of mild dental fluorosis, the above cited ADA site has several such photos.
Steven D. Slott, DDS
LikeLike
Point 20 ) Classic example of pseudoscience. Let’s assume that Paul is correct in asserting that the presence of Ca2+ ions affects F- uptake in the GI tract.
Municipal water supplies in NZ have a target hardness (combined concentration of Ca2+ and Mg2+ ions) of 200 mg L-1. Most of this is Ca2+ as Lime (CaO) is typically used to increase pH in one of the final stages of water treatment.
If water was fluoridated to 0.8 mg L-1 F- (unreasonably assuming there is 0 mg L-1 F- to start with) using CaF2 as a source, the concentration of Ca2+ would increase by 0.2 % as compared to using HFA or NaF as a source of F-. This 0.2% change in Ca2+ concentration will not have any appreciable effect on F- uptake in the GI tract.
Given Paul has a PhD in chemistry I cannot believe that he is ignorant of such basic chemistry and so I am left with the unfortunate impression that he is being deliberately deceptive in the way that he presents his arguments.
LikeLike
Yep, exactly, Jo
If there is a hypothetical dual-analyte solution of calcium and fluoride, and
the fluoride was less than 1.0 mg/L, it does not much matter much how much calcium is present (natural range of 20 to 200 mg/L), you would be talking parts per billion of mineralized calcium fluoride. Either Paul is a complete incompetent as a chemist, or is intentionally seeking to mislead the public in regard to there being any “difference” between fluoride ions from CaF and those from HFA.
Steven D. Slott, DDS
LikeLike
Paul Connett has a very thorough argument here. The people mocking him, instead of addressing the points he talks about, are making themselves look like fools. Ad hominem much?
LikeLike
The people mocking him, instead of addressing the points he talks about,
Mel, you are either stupid or haven’t read the comments made in this and earlier articles in the series. Connett’s polemic has been thoroughly exposed.
LikeLike
Mel,
You seem to be very general in your comment, can you provide any specifics?
What did you think of Jo’s wonderful exposé?
LikeLike
Mel, the “ad hominem” fallback doesn’t work. Paul’s not done anything in this current comment but repeat the same mantras that have been refuted time and again by Ken and many others. Do yourself a favor, stop the whining about “poor Paul” and pay attention to the facts.
Steven D. Slott, DDS
LikeLike
Mel,
Paul has actually not had convincing arguments and he has been consistently exposed both in the scientific exchange and in the comments section. His feeble attempt to claim a difference between the hydrated fluoride anions from natural and synthetic sources was really unexpected for someone with a PhD in chemistry. Jo exposed him simply and decisively.
So what is this about not addressing his points. They are being addressed and he is being exposed.
You yourself could do nothing to defend him. I take it you also can see the mistakes he is making?
>
LikeLike
Paul says in respect to claiming a difference betwen natural and artifically sourced fluoride in water:
“Usually when fluoride occurs naturally in the water it is accompanied by large concentrations of ions like calcium.”
But that is in direct opposition to what one would expect from basic chemistry and reported relationships between Ca and F in groundwaters. Solubility relationships would cause F concentrations to decrease as Ca increases and vice versa. That also seems to be the common observation with groundwaters.
With treated public drinking water calcium is also present because of the addition of lime.
Pauls should correct this mistake as it is being repeated by some of his supporters.
LikeLike
Mel, speak English.
Find out what “ad hominem’ actually means before you embarrass yourself in public on the internet.
Look it up.
There’s this thing called google.
Just type in “ad hominem” and the definition will pop up. It doesn’t mean what you think it means.
Let me give you an example, ok?
You’re ignorant and you’re an idiot.
See? Yeah, that’s not an ad hominem.
(…Mel starts to type in something…)
No Mel. Stop what you are doing. Just google “ad hominem”.
It’s not that hard.
(…waits patiently…)
LikeLike
Ken Paul
suggested reading copy and paste from
http://www.academia.edu/1360978/Fluoride_in_Groundwater_Causes_Implications_and_Mitigation_Measures
Aquifer material
Most of the fluoride in groundwater is naturally present due to weathering of rocks rich influoride. Water with high concentration of fluoride is mostly found in sediments of marine originand at the foot of mountainous areas (WHO, 2001; Fawell et al., 2006). Known fluoride belts onland include: from Syria through Jordan, Egypt, Libya, Algeria, Sudan and Kenya, from Turkeythrough Iraq, Iran, Afghanistan, India, northern Thailand and China. There are also same kind of belts in the America and Japan (WHO, 2001). Fluorite occurs in igneous and sedimentary rocks.Deer et al., (1983) reported that the occurrence of fluoride in both these rock types is almostsimilar. Fluoride occurs as sellaite [MgF2], fluorite or fluorspar [CaF2], cryolite [Na3AlF6],fluorapatite [3Ca3(PO4)2Ca(F,Cl2)], apatite [CaF2.3Ca3(PO4)], topaz [Al2SiO4(F,OH)2],fluormica (phlogopite) [KMg3(Si3Al)O10(F,OH)2], biotite [K(Mg,Fe)3AlSi3O10(F,OH)2], pidote[Ca2Al2(Fe3+;Al)(SiO4)(Si2O7)O(OH)], amphibole such as tremolite [Ca2Mg5Si8O22(OH)2] and hornblende[Ca2(Mg,Fe,Al)5(Al,Si)8O22(OH)2], mica, clays, villuanite and phosphorite(Matthess, 1982; Pickering, 1985; Hem, 1986; Handa, 1988; Haidouti, 1991; Gaumat et al.,
Apparently these waters are quite alkaline as well
Town water tends to be more acidic
There is no explanation to any differences in absorption
1992; Gaciri and Davies, 1993; Datta et al., 1996; Apambire et al., 1997; Kundu et al., 2001;
Brindha, K. and Elango, L. (2011)
Fluoride in Groundwater: Causes, Implications and Mitigation Measures. In: Monroy, S.D. (Ed.), Fluoride Properties, Applications and Environmental Management, 111-136.
https://www.novapublishers.com/catalog/product_info.php?products_id=15895
Mohapatra et al., 2009). Fluoride minerals such as fluorite and cryolite are not readily soluble inwater under normal pressure and temperature. But under alkaline conditions and range of specific conductivity between 750 and 1750 µS/cm, dissolution rate of fluorite minerals increase(Saxena and Ahmed, 2001). Granitic rocks which are a typical source of fluoride rich rockscontain fluoride ranging between 500 and 1400 mg/kg (Koritnig, 1978; Krauskopf and Bird,1995), which is much higher than any other rock type. The world average content of fluoride ingranitic rocks is 810 mg/kg (Wedepohl, 1969). The weathering of these rocks results in increasedfluoride content in groundwater. Longer residence time in aquifers with fractured fluoride richrocks enhance fluoride levels in the groundwater. Naseem et al. (2010) put forth that graniticrock and clay in Pakistan contained average fluoride of 1939 and 710 mg/kg respectively.Granite and granitic gneisses in Nalgonda, India contain fluoride rich minerals such as fluorite (0to 3.3%), biotite (0.1 to 1.7%) and hornblende (0.1 to 1.1%) (Ramamohana Rao et al., 1993).Mondal et al. (2009) reported from the same area that the rocks contain 460 to 1706 mg/kg of fluoride. Laboratory studies conducted by Chae et al. (2006) showed that leaching of fluoridefrom granitic rocks contributed 6 to 10 mg/l of fluoride to water.
LikeLike
You’re not helping your side look any better, Ian.
Copy-and-pasting is…a bad thing.
Not a good thing.
Bad.
LikeLike
Hi Ian,
What is your point? It’s not difficult. Just preface your copy-and-paste with a few helpful words.
Are you trying to give Ken and Paul a lesson in Geology or Chemistry?
Don’t be an idiot Ian.
LikeLike
no one seems to know what natural fluorides are in the water or how/why “natural” Fluoride might have different rates of absorption in people
This article I believe is helpful
Just trying to help
Cedric contrary to you I’m on the side of science old or new not just old
so take your Christmas holidays early to so you can clear your mind and enjoy yourself
LikeLike
…no one seems to know what natural…
Ian, there is no excuse for copypasta. None.
Stop it.
Bad Ian.
This article I believe is helpful
Just trying to help
No, Ian. It’s not “helpful” at all.
It stubbornly remains copypasta.
Not good.
Bad.
Are we clear?
Cedric contrary to you I’m on the side of science old…
No, Ian. You are a literacy-challenged idiot.
You are only embarrassing yourself in public on the internet.
Seek help.
LikeLike
Thanks for the critique Cedric it takes one to know one and I can see that its OK for you to copypasta…
Show one study that (from Paul/Ken or any one else) has indicated or made any allowances, in the science, for differences in “natural” fluoride
LikeLike
Thanks for the critique Cedric…
It’s more of a simple statement of fact.
The fact you have such immense trouble with basic English grammar is a dead giveaway.
…it takes one to know one.
No it doesn’t. Smart people spot idiots all the time.
It’s really easy.
….and I can see that its OK for you to copypasta…
Then get your eyes checked. I don’t copypasta. I don’t need too.
Neither does Ken or Stuart nor Chrisopher nor Richard etc.
It doesn’t happen.
Take a good hard look at your post dated December 19, 2013 at 9:59 am.
See?
That’s pure copypasta.
Bad.
Nobody does that but an idiot.
There’s no excuse for it.
So…don’t do it.
Otherwise people point at you and laugh.
Christopher’s advice is golden…
What is your point? It’s not difficult. Just preface your copy-and-paste with a few helpful words.
LikeLike
I think maybe Ian should sit back…relax and take a puff…
LikeLike
Show one study that has indicated or made any allowances, “in the science”, for differences in the chemistry “natural” fluorides
LikeLike
“Show one study…”
This whole business of making a point seems to have escaped you.
A few helpful words would be useful.
The idea is to make a claim and then present evidence.
That’s how people on planet Earth do it.
We don’t have to “show” you anything. Especially when you speak in riddles.
Copypasta remains stubbornly copypasta and you still look like an idiot.
The burden of proof does not shift.
If you have a point to make then make it.
Loud and clear.
Stop dancing.
LikeLike
Cedric, you are full of a lot of nonsensical Jibber-Jabber. Maybe one day you could actually make a point. It would be nice to see you over on the “making sense of fluoride” facebook page. They could sure do with some of your wise help. See you soon.
LikeLike
Luke Duaan Oldfield. The results in Hastings were fraudulently manipulated. Please work on your reading comprehension, or are you just wilfully ignorant? You’re an embarrassment to yourself.
LikeLike
The results in Hastings were fraudulently manipulated.
(roll-eyes)
LikeLike