
Hi Jane,
I read your article in the Sonoma County Gazette which was republished at Paul Connett’s Fluoride Alert website – Fluoridation convert. A scientist explains what changed her mind. You briefly described scientific studies which you claim convinced you to take a stance against community water fluoridation. Apparently you found these so convincing you are now a board member and steering committee member of several anti-fluoridation organisations.
My purpose here is to discuss the studies you refer to because I think your interpretation of them is mistaken. I offer my critique of your interpretation in the spirit of normal scientific exchange and discussion and hope you will respond in the same way.
You wrote that you were exasperated with the fluoridation debate so:
“I started researching for myself. This was familiar terrain: I had published many papers, so I know what it takes to prove a point scientifically, and the data required to get a paper published. I had performed analyses, plotted data and defended my research and interpretations in public forums.”
Good on you. I believe experience in scientific research, scientific publication and the use of scientific literature helps cultivate a critical and intelligent approach to the literature. I think this is essential if one seriously wishes to make sense of apparently contradictory evidence and overcome one’s own confirmation bias.
Is fluoridation effective? The WHO data
You say:
“I quickly found World Health Organization data that stunned me:
• Tooth decay has plummeted in developed countries worldwide, regardless of fluoridation.
• Cavity rates are the same—or even lower – in many non-fluoridated countries compared to the U.S.”
Just a minute! Did you look at the WHO data carefully? Did you take into account the well established multiple factors, beside fluoride, influencing dental health? (Things like diet, health services, dental treatments available, other social health services etc.) Did you consider the difficulty of drawing conclusions from data, especially a small amount of data, taken from different cultural, social and political situations? And, importantly, did you check out the WHO data which compared data from fluoridated and non-fluoridated areas in the same country? (Many of the other confounding factors can be eliminated by making comparisons within a country).
The figure on the left below is the one most often used by anti-fluoride activists for obvious reasons – it confirms their bias. But it suffers from all the problems mentioned above (including the fact that the straight lines result from using just 2 data points for each country) and so does not allow a truly objective person to conclude what you have.
Surely with your scientific experience you checked out the detail in the data – such as the WHO data for the Irish Republic which included that for both fluoridated and unflouridated areas? The plot of that data (see figure in the right) suggests your conclusion is unwarranted (the dotted line is the average of fluoridated and unfluoridated and corresponds to the data in the graph on the left.).
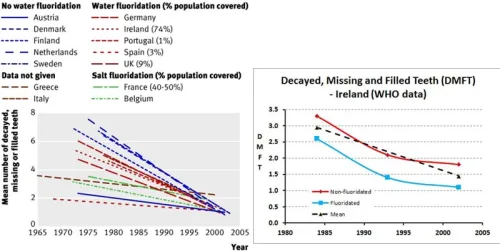
My conclusion from the WHO data is that tooth decay has decreased in all these European countries over the last 30 years. Fluoride is just one factor in this but it is wrong to conclude from the WHO data that fluoride is ineffective (see Fluoride Debate).
Dental fluorosis
This concerns you because:
• The one clear correlation with water fluoridation is disfiguring “dental fluorosis” supposedly only a cosmetic problem.
But, Jane, have you looked at the available data on dental fluorosis carefully? Your conclusion is a misinterpretation which anti-fluoride propagandist love to promote because it confirms their bias – “fluoridation causes a “disfiguring” complaint – dental fluorosis.” But “disfiguring” or serious dental fluorosis is not caused by community water fluoridation. It is caused by excessively high fluoride dietary intake due to high natural levels of fluoride, industrial contamination or obsessive consumption of toothpaste. It is also very rare in the US, Europe, Australia and New Zealand.
Dental specialists identify various levels of fluorosis ranging from not present, through questionable, very mild, mild, moderate to severe – see the figures below (taken from Fluorosis Facts: A Guide for Health Professionals):

Some idea of the appearance of dental fluorosis at these various levels in given by the photos below.

I agree that often (not always) the occurrence of total dental fluorosis may be higher for people in fluoridated areas than in non-fluoridated area – but the “disfiguring” moderate and severe forms are not the result of community water fluoridation. The milder forms which may arise from community water fluoridation tend to be either unnoticeable or so mild as to be of only cosmetic significance.
So Jane, I am surprised that with your scientific experience you came to such an unwarranted conclusion. If you had truly looked at the data intelligently and critically surely you would not have drawn the extreme conclusion you did about community water fluoridation and dental fluorosis.
What about studies showing fluoridation is ineffective?
You refer to studies which show only minimal or no difference in oral health between fluoridated and non-fluoridated areas. I have also seen those studies. But you and I are scientists so know we should always look at the details and not rely on the conclusions drawn by political activists who misinterpret these studies. Hell, as scientists we shouldn’t even rely in the conclusions made by the researchers themselves – we should always look at the details.
Tooth decay for children living in fluoridated and unfluoridated areas has been compared in many studies. It is easy to find results confirming ones bias – pro-fluoridation or anti- fluoridation. So as scientists both you and I should consider all the studies – not just those confirming our particular bias. That should be obvious to us.
I have seen plenty of studies showing a positive effect of community water fluoridation on oral health – so how do I deal with those other studies showing no effect? Well, I certainly don’t ignore them but it helps to look at the details. For example, in my article Fluoridation: what about reports it is ineffective? I discussed a 1985 paper by a New Zealand researcher, John Colquhoun, who found no differences in tooth decay between children in fluoridated and unfluoridated areas.
Colquhoun, who was also an antiifluoridation campaigner, chose to conclude that fluoridation had no effect on oral health. But here is the problem – the children in the non-fluoridated areas he studied all received regular topical dental fluoride application treatments, whereas most of the children in the fluoridated areas did not. So the lack of effect was hardly surprising. In scientific terminology his control group was not a proper control.
What happens when fluoridation is stopped
The studies showing no increase in tooth decay when fluoridation is stopped are continually quoted by anti-fluoridation propagandists – but never the ones that do show such an increase. So your reading of the published studies cannot have been very thorough for you to conclude:
“Tooth decay did not go up when fluoridation was stopped.”
For example, consider just one study in South-west Scotland by Attwood and Blinkhorn (1991) I discussed in article What happens when fluoridation is stopped? The figure below displays some of their data
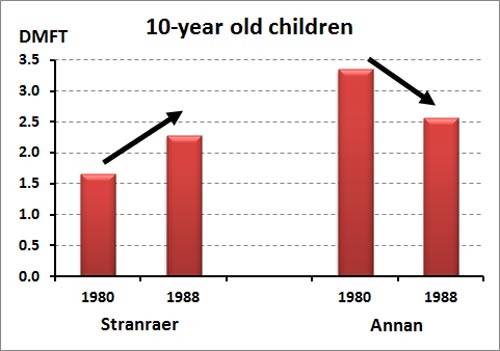
Decayed missing and filled teeth for 10 year olds. Stranraer fluoridated until 1983. Annan not fluoridated.
This study showed tooth decay increased after fluoridation was stopped in one town (Stranraer) even though there was a general decrease in tooth decay (no doubt resulting from things like improvements in diet, tooth brushing, dental treatments, etc.) indicated by the data from the town that had never been fluoridated (Annan).
Still, what about those studies which showed no increase in tooth decay when fluoridation was stopped? Studies in Cuba, the former East Germany and Finland are frequently quoted by anti-fluoridation activists. I discussed these in my article What happens when fluoridation is stopped?
In all the studies referred to the researchers themselves drew attention to the role of other factors which helped maintain oral health. For example, the introduction of a school mouthrinsing programme, which has involved fortnightly mouthrinses with 0.2% NaF solutions” in La Salud, Cuba. Or “improvements in attitudes towards oral health behaviour and, on the other hand, to the broader availability and application of preventive measures (F-salt, F-toothpastes, fissure sealants etc.)” in the former East Germany.
The authors of the Finnish study even warned against drawing the conclusion you have from these studies:
“The main reason for the modest effect of water fluoridation in Finnish circumstances is probably the widespread use of other measures for caries prevention. The children have been exposed to such intense efforts to increase tooth resistance that the effect of water fluoridation does not show up any more. The results must not be extrapolated to countries with less intensive preventive dental care.”
The whole issue of dental health is clearly complex and many factors influence it. As a scientist used to dealing with complex issues you must surely agree the scientific literature should not be cherry-picked. It must be approached critically and intelligently.
Apply It, or Swallow It?
Finally, Jane, we come to the question of the mode of action of fluoride – does it work systemically via ingestion, or topically by a surface reaction on existing teeth? You assert:
In recent years the differentiation between swallowing fluoride and coating teeth with it has become lost in the discussion. But this differentiation is essential. The overwhelming consensus among scientists, including the Centers for Disease Control CDC and the National Research Council, is that fluoride works when it’s applied to the tooth surface, NOT when it’s swallowed.
I know this is the position anti-fluoride propagandists keep promoting but it doesnt actually accord with the evidence. Research shows ingested fluoride plays a beneficial role during tooth development before eruption (see my article Ingested fluoride is beneficial to dental health.
With existing teeth fluoride transferred from water and food during drinking and eating helps maintain a concentration in saliva and tooth biofilms necessary to inhibit tooth decay by a surface reaction. Researchers usually refer to the reaction of fluoride at the tooth surface responsible for inhibiting demineralisation and promoting remineralisation as the “predominate” – not the only – mechanism for the beneficial role of fluoride.
Jane, you should have read the CDC report you refer to more carefully. Far from denying a role for “swallowed” fluoride the CDC report Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States actually says:
“However, drinking fluoridated water, brushing with fluoride toothpaste, or using other fluoride dental products can raise the concentration of fluoride in saliva present in the mouth 100-to 1,000-fold. The concentration returns to previous levels within 1–2 hours but, during this time, saliva serves as an important source of fluoride for concentration in plaque and for tooth remineralization.”
Unfortunately, opponents of CWF claim this surface mechanism means that ingested fluoride plays no role and fluoride is only effective when topically applied – as with toothpaste. This is a gross simplification and distortion. Ingested fluoride is beneficial to teeth duing their development before eruption. And ingested fluoride contributes to the surface reaction protecting existing teeth.
Fluoridated toothpaste (and dental fluoride applications) also contribute to this surface reaction. But the more frequent “top-up” of saliva fluoride concentrations via drinking fluoridated water also make an important contribution.
An invitation
Jane, I don’t claim to have provided the final answer to all criticisms of community water fluoridation here. I have simply responded to your assessments and shown why I think them wrong.
I am open to hearing your responses to my critique and welcome any scientific exchange on this important issue with you.
I look forward to hearing from you.
Ken Perrott.








These conversion stories are unimaginably tiresome. They all think they are Saul on the Road to Damascus. As if changing their minds somehow validates their mistaken “research.”
LikeLiked by 1 person
Ken claims to have had a road to Damascus experience when he found fluoride in apatite’s. Good job he didn’t know about lead, otherwise he would be advocating leaded water! Another question is why give fluoride to people who have fluorosis?
LikeLike
We all look at the world through our own filters and sometime scientists are just as guilty of cognitive biases as the rest of us. For example, there are some scientists who believe in creation rather than evolution. No evidence can persuade them to the contrary.
LikeLike
Agreed, logichick. But the scientific process which checks ideas against reality and is social in nature so opens up ideas to peer critique is a powerful way of overcoming the all too human failing of confirmation bias.
LikeLike
No Shane, my claim to a road to Damascus experience relates to fluorosilicic acid. When I did some research on a local sample the heavy metal analysis (including As and Pb) showed contamination to be extremely low. This convinced me that the anti-fluoridation activists were lying about heavy metal contamination and ever since I have checked any claims they make. I often find they are lying about these a well.
As for fluoride in apatites, the normal and natural presences and it’s role in lowering solubility and increasing hardness has been known and understood for a long time. It wasn’t my discovery.
But, again, your comment does not relate to the article.
LikeLiked by 1 person
Ken: sorry it took me so long to be connected with your message, and then to get around to replying. I certainly have read and assessed much recent research on the effects of fluoride, some of it from U.S. sources, even though I’ve been told that little research on fluoride effects is being done here.
Before sharing my investigations, I will establish my scientific bona fides (see below). I will respond further after you have replied with yours. Jane
CAREER SUMMARY
Jane Nielson holds an A.B., M.S. and Ph.D. degree in multiple geoscience fields. The A.B. in Geology is from The George Washington University, Washington DC (minor in French); the M.S. is in Geochemistry (principally aqueous geochemistry), from The University of Michigan, Ann Arbor, MI; and the Ph.D. in Geology is from Stanford University, Stanford, CA. She also is certified as a licensed Professional Geologist in California (Lic. no. 9011).
She is a Fellow of the Geological Society of America, and formerly maintained memberships with the Geochemical Society of America and Mineralogical Society of America.
From 1974 until her retirement in 1998, Dr. Nielson performed field and laboratory studies as a Research Scientist for the U.S. Geological Survey, in Menlo Park, CA. Her work included mapping and correlating volcanic and sedimentary rock sequences in western Arizona and southeastern California, and characterizing and interpreting their major, minor, and trace element, and isotopic compositions. She also worked on landslide-prone rocks of the California Coast Ranges and the geochemical characteristics (same list as above), of samples from the Earth’s mantle that she and colleagues collected at sites in North Carolina, Arizona, California, Nevada, New Mexico, southern and western Australia, and central and southern France.
Her publications include 42 scientific research papers in refereed journals or USGS publications, plus 32 abstracts, and 8 maps. She has given too many presentations of her work to detail here, both as an applicant and invited participant, and organized numerous scientific symposia and workshops.
She also has taught university courses: prior to and subsequent to her USGS career. Prior to being hired at USGS, Dr. Nielson taught undergraduate and general science and geology lab courses at Northern Arizona University, Flagstaff AZ; and both undergraduate and graduate courses at California State University, Hayward CA (now CSU East Bay). After retirement, she taught undergraduate geology lecture and lab courses at Pomona College, Claremont, CA.
After retirement, she co-authored The American West at Risk: Science Myths, and Politics of Land Abuse and Recovery (Oxford University Press, 2008 — see WordPress site given below), while co-founding water-related organizations in Sonoma County, CA, including the Sebastopol Water Information Group and the Sonoma County Water Coalition.
In 2010, The Sonoma County Conservation Council voted to recognize her contributions with their Environmentalist of the Year award.
LikeLiked by 1 person
Good that you have made contact, Jane, and are willing to discuss this issue. I look forward to a good scientific exchange.
I am not really interested in what we crude Kiwis call a “pissing competition” regarding “scientific bona fides,” especially as such things are easy to check on-line. However, briefly we are probably in similar positions. I am retired after a career in chemical research (my PhD is in chemistry and I did a little university teaching in the early days). I think I have about 70 peer reviewed publications and a number of commercial reports and one patent.
While my first publications were on the reaction of fluoride with soil and soil minerals I have not worked directly on fluoridation itself. I have been aware of the chemical role of F in apatites having researched them a little in studies on soil phosphorus and fertiliser phosphorus. But one “road to Damascus” moment for me was some research I did about 10 years ago on fluorosilicic acid, it’s uses and a possible use in treating biosolids wastes. When I analysed the material we were using for heavy metals I was initially shocked to find the levels were extremely low – this indicated to me that what I had heard from anti-fluoride activists, and initially believed , about contamination was just not true. Since then I have checked out many of their claims and found them to be similarly untrue.
I hope that is sufficient for you to accept the worthiness of me as a partner in a scientific exchange on the fluoridation issue. Hopefully you can respond to my critique above of your original article. If you would like something more extensive perhaps we could discuss the possibility of an an-going exchange similar to the one I has with Paul Connett in the Fluoride Debate.
LikeLike
Hi Ken–
I want to know your employment history. Thanks.
LikeLike
Why, Jane?
Your are not interviewing me for a job, just responding to my invitation for a scientific exchange, or simply to my critique of your article. The science is not dependent on either your or my “employment history.”
But again, briefly, I have worked as a paper boy, milk delivery, office cleaner, etc. Scientifically as a university lecturer during PHD studies and since mainly in NZ research institutes like DSIR, MAF and AgResearch.
Now, please, let’s get into the science.
LikeLike
Jane, are you ready to respond to my open letter yet? Or do you want to give it a miss?
LikeLike
Disappointing that Jane has not replied back after those weird questions. I guess with the silence we concluded Ken wins this one.
LikeLike
Yes, me too Zammbi.
I have submitted a shorter version of this post to the original journal her article was in – maybe she will respond to that.
LikeLike