
I welcome open and transparent discussion here so am thankful to Dr Micklen for his response (see NZ Fluoridation review – HS Micklen responds to critique). Unfortunately he is the only author or “peer-reviewer” of Fluoride Free NZ’s report criticising the NZ Fluoridation review to accept my offer of a right of reply to my critiques. A pity, as if any of them think I have got things wrong, and they can support this with evidence, I certainly want to know about it. There are three aspects to Dr Micklen’s reply – dental fluorsis chronic kidney disease and his critique of my letter in the journal Neurotoxicology and Teratology – Perrott (2015). I will deal with these separately.
Dental fluorosis
I appreciate Dr Micklen is unhappy about my criticisms of his article, and my suggestion his comments of dental fluorosis were muddled. I may have been a bit harsh but he has still not responded to my specific criticism that he:
“unfairly attributes the more severe forms [of dental fluorosis] to community water fluoridation (CWF). Consequently he calculates a cost of dental treatment which is wrong.”
The key problem is that Micklen is assuming that all the medium and severe dental fluorosis can be attributed to CWF, whereas none of it can. Briefly reviewing the argument – the figure below is from the NZ Ministry of Health’s “Our Oral Health“ – the same source Micklen used. 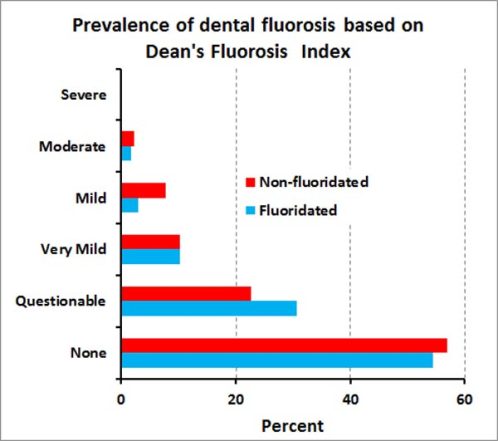 My comment on the relevance of the different grades of dental fluorosis was:
My comment on the relevance of the different grades of dental fluorosis was:
“Moderate and severe grades of dental fluorosis are common in areas where fluorosis is endemic, but relatively rare where CWF is used. Occurrences in the latter case, despite the low concentrations of fluoride in treated drinking water, will have other causes – high natural levels in well water, industrial pollution, excessive consumption of toothpaste, etc.”
The important factor is that severe and moderate forms of dental fluorosis are not caused by CWF. CWF can contribute to mild and very mild forms of dental fluorosis but because these are usually judged positively they certainly don’t need expensive veneers – my dentist colleagues advise simple microabrasion usually works. So Micklen was wrong to suggest the cost of cost of veneers (up to $1750 per tooth) should be attributed to CWF because such costs would be encountered in non-fluoridated areas as well. (In fact, if Micklen had calculated costs for such treatment in non-fluoridated areas using the “Oral Health” data in the literal way he did for the fluoridated areas, he would have found costs to be higher than in non-fluoridated areas! Certainly doesnt’ support his claim but a meaningless result because of the small numbers and large variability).
Chronic kidney disease
Micklen accuses me of using “a piece of grammatical legerdemain to pretend that I [Micklen] called for CKD sufferers to be warned to avoid tap water, which I did not.” Granted he left himself a way out by actually writing:
“I suspect that most opponents of fluoridation would call for CKD sufferers to be warned to avoid tap water. Possibly the NZ health authorities have done so.”
OK, so its not a direct personal recommendation (perhaps he doesn’t belong to the group of “most opponents of fluoridation”) but a reader could be excused for getting that message and in this context it comes across as “dog whistling.” However I will accept his assurance now that:
” In fact, I am inclined to agree with him [me] that that might be extreme in the present state of knowledge.”
As for questions like: “Does further research on the topic receive any funding priority, for example?” – well this is a round about way of giving the message that it doesn’t. Perhaps he should actually check that out and give some evidence instead of making an unwarranted implication. This tactic of posing unfounded questions to convey an unwarranted message is typical of the approach Micklen and Connett take in their book The Case against Fluoride. I criticised this tactic in my exchange with Paul Connett (see Fluoride Debate). I reject Micklen’s suggestion that:
“Perhaps it would be embarrassing, too, for a government to insist on putting fluoride in the water and then advise a substantial number of people not to drink it – or so one might think.”
That is silly – it is like a conspiracy theory. Why would genuine health authorities refuse to give warnings to a small group of people who might be put at risk from a social health policy that is beneficial to the vast majority? Surely they are used to such situations. I also think he is waxing lyrical with the word “substantial!” The numbers involved would be very small, if any, and such a group would already be advised about a number of risks to them because of their condition and treatments. Micklen also lets his ideological position take over by drawing the implication from my article that I am saying CWF is “effective and safe – for some.” Far from it. Surely I am saying it is effective and safe for the vast majority (which is what we can expect from a social health policy) and simply recommending (as in all such policies) that the small group of people, if any, who might be at risk should use alternatives. I am actually saying that CWF is effective and safe for at least the vast majority and that claims to the contrary should be backed up with evidence which should be considered critically
Severe dental fluorosis and cognitive deficits
I thank Dr Micklen for his comments on my letter in the journal Neurotoxicology and Teratology – (Perrott 2015). I am pleased he accepts the hypothesis that severe dental fluorosis could explain observations of cognitive deficits is worth considering and he agreed with the other reviewers the letter was worth publishing. Influence of age I take his point that the poor appearance of teeth may not influence young children (ages 6-8 as in the small the group Choi et al, (2015) studied). However, this is pure speculation on his part and is surely a detail. A detail that should be considered in any planned research incorporating this hypothesis, but not in itself a reason for rejecting the hypothesis out of hand – surely? Unless, of course, he can give evidence to support his suggestion. I notice that he does not support the idea with any citations so suspect the idea is more one of straw-clutching than a serious suggestion. Actually most, but not all, of the citation I used did indeed refer to work with older children. Some were review papers and did not limit their review to any age group. Aguilar-Díaz, et al., (2011) considered children from 8 – 10 years old, Do and Spencer, (2007) studied 8-12 year olds and Abanto et al., (2012) 6-14 year old children. Chikte (2001) studied three groups: 6, 12, 15 year olds. However, I found a quick literature search showed reports of negative effects of oral defects like tooth decay on the child’s quality of life. Kramer et al., (2013) reported this for ages 2 – 5, Scarpelli et al., (2013) for 5 year olds and Cunnion et al., (2010) for 2 – 8 year olds. So, I suggest on the available evidence the negative influence of severe dental fluorosis on quality of life (and possibly cognitive deficits) is likely to occur even in younger children who have not “reached an age to be self-conscious about their appearance.” I don’t think young children are as immune to social attitudes and personal appearance as Dr Micklen suggests. Does effect depend on how common dental fluorosis is? Dr Micklen suggests that:
“Since fluorosis was common in the community [the children studied by Choi el., 2015], having the condition would not appear abnormal.”
Again I think he is indulging in straw-clutching, or special pleading.  Clearly medium and severe dental fluorosis is far more common in this Chinese group than in countries like New Zealand which use CWF. In the graph below I compare their data with that for New Zealand and USA. Incidentally, this figure shows why the data from Choi et al., (2012, 2015) should not be used as an argument against CWF – yet that is what Micklen did in his original article.
Clearly medium and severe dental fluorosis is far more common in this Chinese group than in countries like New Zealand which use CWF. In the graph below I compare their data with that for New Zealand and USA. Incidentally, this figure shows why the data from Choi et al., (2012, 2015) should not be used as an argument against CWF – yet that is what Micklen did in his original article.  But this does not mean that those children with more severe forms will not stand out against the children with less severe forms. There is always a range of appearances of such defects in a group of children. Some will obviously suffer more than others because of their appearance. If Choi et al., do continue to include detailed analysis of dental fluorosis in their future work on this issue then it will be possible to compare cognitive deficit measurements with dental fluorosis indices in a larger group. Such data will be interesting. However, discussion of details like this is premature. My letter simply raised to idea as an alternative worth considering and encouraged the group to continue including detailed dental fluorosis measurements in future work. I was also concerned that they were not being sufficiently open-minded in their choice of a working hypothesis. I concluded my letter with:
But this does not mean that those children with more severe forms will not stand out against the children with less severe forms. There is always a range of appearances of such defects in a group of children. Some will obviously suffer more than others because of their appearance. If Choi et al., do continue to include detailed analysis of dental fluorosis in their future work on this issue then it will be possible to compare cognitive deficit measurements with dental fluorosis indices in a larger group. Such data will be interesting. However, discussion of details like this is premature. My letter simply raised to idea as an alternative worth considering and encouraged the group to continue including detailed dental fluorosis measurements in future work. I was also concerned that they were not being sufficiently open-minded in their choice of a working hypothesis. I concluded my letter with:
Researchers need to be careful not to limit their possible hypotheses or research approaches. Unfortunately Choi et al. (2014) appear to be doing just this with their plans for a larger scale study targeted only at “fluoride’s developmental neurotoxicity.”
Unfortunately none of this group have yet responded to my letter. So, again, I thank Dr Micklen for his feedback on that letter – and his acceptance of the right-of-reply to my article critiquing the FFNZ report. See also:
- Review by Royal Society of NZ and the Office of the Prime Minister’s Chief Science Advisor:
Health Effects of Water Fluoridation: a Review of the Scientific Evidence.
- Critique by Fluoride Free NZ organisation: International Peer Review of the Royal Society/PM Science Advisor Office Fluoridation Review.
- Anti-fluoride activists define kangaroo court as “independent”
- The farce of a “sciency” anti-fluoride report
- Peer review of an anti-fluoride “peer review”
- Cherry-picking and misinformation in Stan Litras’s anti-fluoride article
- Fluoride Free NZ report disingenuous – conclusion
- Did the Royal Society get it wrong about fluoridation?
References
Abanto, J., Carvalho, T. S., Bönecker, M., Ortega, A. O., Ciamponi, A. L., & Raggio, D. P. (2012). Parental reports of the oral health-related quality of life of children with cerebral palsy. BMC Oral Health, 12, 15. doi:10.1186/1472-6831-12-15 Aguilar-Díaz, F. C., Irigoyen-Camacho, M. E., & Borges-Yáñez, S. A. (2011). Oral-health-related quality of life in schoolchildren in an endemic fluorosis area of Mexico. Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 20(10), 1699–706. Chikte, U. M., Louw, A. J., & Stander, I. (2001). Perceptions of fluorosis in northern Cape communities. SADJ : Journal of the South African Dental Association = Tydskrif van Die Suid-Afrikaanse Tandheelkundige Vereniging, 56(11), 528–32. Choi, A. L., Sun, G., Zhang, Y., & Grandjean, P. (2012). Developmental fluoride neurotoxicity: A systematic review and meta-analysis. Environmental Health Perspectives, 120(10), 1362–1368. Choi, A. L., Zhang, Y., Sun, G., Bellinger, D., Wang, K., Yang, X. J., … Grandjean, P. (2015). Association of lifetime exposure to fluoride and cognitive functions in Chinese children: A pilot study. Neurotoxicology and Teratology, 47, 96–101. Cunnion, D. T., Spiro, A., Jones, J. a, Rich, S. E., Papageorgiou, C. P., Tate, A., … Garcia, R. I. (2010). Pediatric oral health-related quality of life improvement after treatment of early childhood caries: a prospective multisite study. Journal of Dentistry for Children, 77, 4–11. Do, L. G., & Spencer, A. (2007). Oral Health-Related Quality of Life of Children by Dental Caries and Fluorosis Experience. Journal of Public Health Dentistry, 67(3), 132–139. Kramer, P. F., Feldens, C. A., Ferreira, S. H., Bervian, J., Rodrigues, P. H., & Peres, M. A. (2013). Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dentistry and Oral Epidemiology, 41(4), 327–35. NZ Ministry of Health. (2010). Our Oral Health Key findings of the 2009 New Zealand Oral Health Survey. Perrott, K. W. (2015). Severe dental fluorosis and cognitive deficits. Neurotoxicology and Teratology. Scarpelli, A. C., Paiva, S. M., Viegas, C. M., Carvalho, A. C., Ferreira, F. M., & Pordeus, I. A. (2013). Oral health-related quality of life among Brazilian preschool children. Community Dentistry and Oral Epidemiology, 41(4), 336–44.








Still don’t get it do you Ken?
What one person regards as mild fluorosis can be quite different for another and since the chances of getting any redress from dental authorities who will keep denying that fluoridated tap water could ever possibly have caused their distress, people should not be left at the mercy of this academic debate – reminds me of arguments of how many angels can dance on the head of a pin.
I see young people in Auckland with dental fluorosis all the time and try not to make them self-conscious by staring at them.
It is time to stop forcing people to imbibe your prejudice and let those that choose to poison their children do so by supplying them with pharmaceutical grade fluoride tablets – or water – where at least they won’t be taking the cadmium, arsenic, lead etc.
You can argue all you like, nit pick and split hairs until the cows come home BUT I reject your assumption that I, and others, need to risk sacrificing our health to that of your mythical ‘greater good’.
It is no different to the Nazis experimenting on children and others and their Aryan assumption of superiority – in fact the studies that show that indeed Pacific Islanders, Negroes and Hispanics are more prone to the adverse effects – so perhaps the Nazis are alive and well protected by the Dental ASSes?
LikeLike
Need to look into various ways used of putting a spin on things.
Our great TeAra is placing a spin by omitting to say Maori did not suffer from tooth decay in pre-European days, and only saying they wore their teeth out chewing fibrous plants.
It also does not say Maori life expectancy had been better than that in Britain before Moehanga of Ngāpuhi was presented to King George III in 1806.
European ways have introduced Maori to many diseases including tooth decay and now want to proclaim how great they are by reducing a proportion of that with fluoride, and getting very annoyed when anyone wants to talk about old ways and better teeth.
LikeLike
So Soundhill. Nothing to say about this post? You don’t want to defend Micklem’s reply?
>
LikeLike
Ken I have to click on a ref to his work but it just gives me more of your selections.
““Since fluorosis was common in the community [the children studied by Choi el., 2015], having the condition would not appear abnormal.””
I would have to add to that that you never replied to my assertion that if comparative appearances meant anything then why would the children who get taunted as “four-eyes” for wearing spectacles actually turn out to be higher in IQ?
And a point of my previous article also includes how did the pre-European Maori have good teeth without fluoridation in NZ then? That seems to add credibility to claims of Micklen and other anti-fluoridationists for rights.
LikeLike
Soundhill – what is the problem with accessing Micklen’s response or his original – all my citations to him are linked?
Could you please report the study you refer to which proves that children taunted with the “four-eyes” chant turn out to have a higher IQ? sounds very interesting and I am surprised you didn’t already provide the citation.
Pre-European Maori had a number of dental problems as indicated from bones and skulls – absesses and wear, for example. I imagine for much of their time in NZ they would have consumed a diet relatively high in fluoride because of high seafood consumption.
However, our social health policies are directed at the current population, not a population which no longer exists.
LikeLike
Ken I cannot see Micklen links to his work. Only leading back to yours.
I don’t know of research between the taunting of children related to their spectacles for shortsightedenss. I just remember it from school. Do you know the same for fluoridosis?
According to Rodney Hide as I posted on msof there were very few signs of abscesses. If you have better figures than “a number of” please give them.
Inland Maori had goitre, need to check their teeth.
LikeLike
The link to Micklen’s reply ( (see NZ Fluoridation review – HS Micklen responds to critique)) links back to the previous post whcih is his reply. If you want to go further they are in the links to the FFNZ report which his article was in.
So you are making a claim about taunting nwhich you have absolutely no information to support? Bit pathetic isn’t it?
Read my letter to the editor – all the citations regarding effects of dental fluorosis and dental decay on quality of life are in that – although I added a couple in this post specifically responding to Micklen’s straw man about age.
There are several papers I read some time ago going into detail (didn’t know Rodney Hide was a reputable person to cite 🙂 ) but no I am not going to search them down for you. I just do not have the time.
It is a pointless discussion because, as I said we don’t determine our social health policies based on situations which not longer exist.
LikeLike
Ken, are milk teeth exempt from fluorosis?
It would seem that Miklen’s argument requires that to be so.
LikeLike
A quick search shows dental fluorosis also occurs with primary teeth.
I think Micklen’s argument is that concern for appearance does not occur until teenage years and therefore younger children would not have their quality of life decreased by dental defects. The references I cited suggests he is wrong.
>
LikeLike
Ken:
******************
I reject Micklen’s suggestion that:
“Perhaps it would be embarrassing, too, for a government to insist on putting fluoride in the water and then advise a substantial number of people not to drink it – or so one might think.”it would be embarrassing . . ” – that is too much like a conspiracy theory.”
******************
You are mixing things up there Ken. I do not see Micklen mentioning conspiracy there.
LikeLike
No, another typo – have corrected a few now.
LikeLike
Ken: “It is a pointless discussion because, as I said we don’t determine our social health policies based on situations which not longer exist.”
It is common to use dietary advice to return health to a better condition. Sometimes the advice is changed as seems to be for fat at the moment. Alternative advice about fat should have been listened to earlier. Same as alternative advice about tooth health.
I presume by the situation which currently exists you mean you do not want to upset a number of large corporates. We can do it, though, as with smoking.
LikeLike
Richard: “Ken, are milk teeth exempt from fluorosis?
It would seem that Miklen’s argument requires that to be so.”
Why do you think that? Those kids were at the age they were starting to lose their first teeth. Though it happens to everyone, having the gaps would surely overshadow fluorosis in terms of appearance for those children, the latter consequently being hard to distinguish in terms of social effect and a chlld’s awareness of its body and differences. Micklen points out it is for older children that Ken is hypothesisng, though Ken says there is some reference for younger ones, but I cannot find it.
LikeLike
You presume wrong – and your putting words in others’ mouths is insulting.
Grow up and discuss things properly.
>
LikeLike
Soundhill, your unwillingness to read things properly and then make assertions based on ignorance is becoming tiresome.
No one pointed “out it is for older children that Ken is hypothesisng” I certainly wasn’t restricting the idea to older children and all Micklen did was argue that my citations related mainly to older children leaving him wiggle room to propose that younger children were not affected because they were not self-conscious. He didn’t support his suggestion with any literature. I pointed out that indeed younger children were part of at least some of the studies cited and then cited three more studies involving younger children Please read things properly before casting aspersion like this.
>
LikeLike
Ken wrote: “No one pointed “out it is for older children that Ken is hypothesisng” I certainly wasn’t restricting the idea to older children and all Micklen did was argue that my citations related mainly to older children”
Micklen wrote: “When he finally presents evidence that moderate-severe fluorosis is aesthetically displeasing and likely to impair quality of life, all of it relates to older children, mainly teenagers,”
Not “mainly,” “all of it.”
I am trying to find your refs.
LikeLike
Yes, Micklen claimed that my citations referred only to older children. I just corrected him to “most.” As some of the studies had younger children. Micklen was incorrect. But, as I said, I took his point and identified studies with younger children and added 3 more citations.
Read the bloody article.
LikeLike
Richard: “Ken, are milk teeth exempt from fluorosis?
It would seem that Miklen’s argument requires that to be so.”
Why do you think that?.
Micklen describing Choi :
Micklen is implying two things
1) that only permanent teeth are under discussion
2) that the period between eruption of permanent teeth and the testing for cognitive ability is two narrow for the subjects to suffer the hypothetical mechanisms that accompany disfigurement and result in impairment.
Consideration of psychological pressures arising from damage to primary teeth as well would extend the window of time that he argues is narrow.
LikeLike
We should also note that Choi et al (2015) found a significant relationship of cognitive defects to severe dental fluorosis. So that is another bit of evidence for considering a mechanism related to effects on quality of life including children with primary teeth.
Correlation is not causation – that argument also applies to F in drinking water – which did not show a relationship to cognitive deficits in their case.
Let us remember this letter to the editor was not claiming a proven mechanism – it was simply a warning that Choi et al should not limit their investigation to one hypothesis. The two referees agreed that point was worth making – and Micklen sort of did to.
>
LikeLike
regarding soundhill’s claim about Maori having good teeth in pre-European times: they didn’t. While they didn’t have a lot in the way of caries, they did suffer badly from worn-down teeth and the concomitant health issues. (You’re right about the high levels of seafood, too, Ken.) And I shall provide a citation for this: https://ourarchive.otago.ac.nz/handle/10523/3865
LikeLike
Intriguingly there does appear to be some evidence of a link between myopia & IQ (http://www.ncbi.nlm.nih.gov/pubmed/19127804 – oooh look, another citation!), though why this is relevant to a discussion of a ‘review’ of a paper on fluoridation is beyond me.
LikeLike
This long pubmedcentral historical pdf article indicates how the Urewera Maori who lived a long way from the coast (50-60km?) had an incidence of goitre of about 18%, indicating low sea food intake, therefore presumably low fluoride.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2167656/pdf/jhyg00280-0084.pdf?origin=publication_detail
But they also had low caries. (I said good teeth once, but meant low decay, as I said the other time) 99% decay free (1928 article):
http://paperspast.natlib.govt.nz/cgi-bin/paperspast?a=d&d=CHP19280301.2.45
I’ve started checking Ken’s refs. The Kramer et al refers to “young children with oral disease and disorders perceived that both the children and other family members had poorer quality of life”. But the troubles discussed are where there are (severe?) eating difficulties: the teeth do not close properly on the food, or are broken or have tooth decay pain. Fluoridosis would tend to be associated with less tooth decay.
Fluoridosis would in many cases be more of an appearance thing rather than causing eating difficulties or pain. I referred to spectacles because I know children wearing them get teased about their appearance. But they tend to have higher IQ if short sighted (more common than long sighted.) So I do not think the appearance to be so important.
I am trying to look up minor physical abnormalities and IQ deficit. I have looked into it before and I would understand it in terms of congenital abnormalities, low set ears with risk of middle ear infection and hearing loss (IQ?) and they may also be associated with kidney disease (Clinical Genetics in Nursing Practice – Felissa L Cohen) One abnormality often associated with another. Goitre can be associated with cretinism and that is not congenital. A lack of iodine has more than one result.
LikeLike
Soundhill – you misrepresent Kramer.
They actually say in their abstract “Negative impacts were more prevalent on items related to pain, difficult drinking and eating some foods.” Other items are not excluded.
They are referring to “items” that are part of the “Early Childhood Oral Health Impact Scale” and its relationship to quality of life. Eating difficulties is only one of the factors relevant.
From my own experience as a child I can assure you that pain and lack of sleep are also an important result of childhood tooth decay which highly impact quality of life and I am sure presents difficulties to learning.
Kramer’s data certainly do not restrict the negative effects simply to eating difficulties.
Cunnion’s results show that negative effects on quality of life were certainly not restricted to eating difficulties. The concluded “Compared with caries-free children, early childhood caries children were more likely to have worse questionnaire response scores and to experience greater negative impacts on physical, mental, and social functioning.”
But what is the point of all your special pleading? All I have done is suggest an hypothesis which is at least as capable of explaining Choi et al (2015)’s results as chemical toxicity – and has more support from the data. I specifically said in the above article:
Now, Soundhill, do you agree with that statement?
Or do you think (contrary to the 2 peer reviewers and Micklen) my letter should not have been published?
LikeLike
Ken
I only had the Kramer abstract, and quoted the three issues in it. You seem to think I did not include pain, but I did.
I think it is always good to question research and hope for better.
I am wondering if Kramer talked of “severe dental fluorosis.”
Here is a study which cites Kramer. It does not name fluorosis but speaks of white spots on teeth.
Click to access 1477-7525-12-55.pdf
In that I need to understand better: “Parents/caregivers’
perception of their child’s oral health was associated with a negative impact on the OHRQoL [Oral Health Related Quality of Life] of both the children and families. Perceptions of parents/caregivers regarding their child’s oral health
plays an important role in the determination of the negative impact on OHRQoL [39], as the health of pre-school children depends on parental/caregiver knowledge regarding health care [40]”
Is it saying parents perceptions are both affecting the variables as well as being the variables?
It is rather complex. IQ measurements seem to be more independent of subjectivity.
You wrote previous article:
“Correlation is not causation – that argument also applies to F in drinking water – which did not show a relationship to cognitive deficits in their case.”
That lends weight to my theory that certain individuals are not so good with fluoride intake. I suggest some do not metabolise it so well. By that I mean they are not able to send the correct amount to the skeleton and teeth and excrete the extra in urine.
I hypothesise that children with severe dental fluorosis have had difficulty excreting fluoride and it is not only causing dental problems.
It would be interesting to get Choi’s figures and do some partial correlations.
LikeLike
Choi et al’s figure are in their paper which has been cited numerous times in my articles. Partial correlate away to your heart’s content.
>
LikeLike
Soundhill – you ignored my question. Could you please answer it.
I said in the above article:
“However, discussion of details like this is premature. My letter simply raised to idea as an alternative worth considering and encouraged the group to continue including detailed dental fluorosis measurements in future work. I was also concerned that they were not being sufficiently open-minded in their choice of a working hypothesis. I concluded my letter with:
Researchers need to be careful not to limit their possible hypotheses or research approaches. Unfortunately Choi et al. (2014) appear to be doing just this with their plans for a larger scale study targeted only at “fluoride’s developmental neurotoxicity.”
LikeLike
Ken I said it is always good to question research.
Of course I believe it good to continue to measure fluorosis as it may indicate the body is not dealing with it.
As for your letter, would you have changed it had Micklen been quicker getting back to you before you sent it? I’ve been wondering about the ref he says is not relevant, and the ages which you have been saying more of.
You will be familiar with catalysts. For other readers a catalytic converter in a car exhaust pipe has a “catalyst” which allows noxious exhaust emissions to combine with oxygen and render them less harmful. However a catalyst may be poisoned so as not to work. The old lead based octane improver would do that, and so may using engine oil that is too thick, I think.
Biochemistry works very much with catalysts.
So I think we need not just to think of fluoride but other factors to go with it.
LikeLike
I got that bit about the danger to a car catalytic converter from thick oil from wiki. But now I am thinking that could be because a car is worn and you are using thick oil, but you are doing that because the thinner oil was getting past the pistons, as may happen with old engines, and getting to the catalyst. In which case thicker oil may get to the catalyst less.
Do you know of a less expensive source for Choi’s figures?
LikeLike
The letter was refereed and published well before Micklen’s article came up. If I had seen his comments before hand I may have included the other 3 citations but that is all. None of the referees raised that issue and I personally see it as special pleading on Micklen’s part. If he had been at all serious he would have done his own literature search – he didn’t.
So I assume you support the publication of the letter? Yes or no?
>
LikeLike
Ken, I think I had a copy of your letter, but now I cannot find it.
Your letter feels rather as if you are trying to make a case for fluoridation, rather than just to advance knowledge. You may be hoping your hypothesis it will get past people not too well versed in biochemistry.
You presented material on oral troubles but did not comment on any scale of social impairment related to various types of oral troubles.
From
http://en.wikipedia.org/wiki/Erikson%27s_stages_of_psychosocial_development
how we appear to others does not concern quite so much till we are getting into adolescence. However the feedback between parent and child which I discussed a little today might translate into negative forces on a younger child. Parent interaction may be very strong. If a parent is positive about a child not being able to bite the upper teeth on the lower ones, then the child may cope more. Maybe fluorosis appearance could elicit a stronger negative emotion from a parent than broken teeth or jaw, overbite and crying from toothache where the parent knows to be more positive. I think you would need to extend your letter to note those parental factors to be controlled for.
I shall need to get Choi’s article before I can answer you.
LikeLike
I will take that as a NO – an ideologically based No, of course.
You have lost your copy of my letter but claim it “feels” as If I am aiming a case for fluoridation – funny as the referees comments said the opposite!
And you admit to not having read the Choi et al (2015) paper!!
Pathetic.
>
LikeLike
Recently on Openparachute I referred to vitamin B3. I have found this article which names the various forms differently to what I said.
“Niacin is the term used to describe two related compounds, nicotinic acid and nicotinamide, both of which have biological activity.”
I think I referred to what I thought is the greater safety of the flushing type of the vitamin, nicotinic acid as opposed to nicotinanide, with time release worse. Now please take into account:
“Severe and potentially life-threatening hepatotoxicity has been associated with treatment of patients with 3-9 g nicotinic acid per day for periods of months or years for the treatment of
hypercholesterolaemia. Severe cases show liver dysfunction and fulminant hepatitis and may even proceed to encephalopathy requiring liver transplantation. Many of
the patients showing hepatotoxicity were taking the slow release
formulation of the compound, so that in contrast
to the flushing discussed above, the development
of hepatic toxicity is a function of long-term
chronic exposure to relatively constant levels rather than the fluctuating levels and rapid rises which produce flushing.”
3g per day is a rather large dose.
Click to access out80j_en.pdf
Next article I want to consider more a possible parallel between slow release niacin and fluoride delivered in water as opposed to food and ask for help with mathematical modelling.
LikeLike
Recently I wrote of poisoning of a catalyst so that the reaction it was helping no longer works.
Some people eat a few stone fruit pips. Stomach acid may release cyanide form the pips. (FSANZ are thinking of banning the sale of apricot pips).
Humans detoxify cyanide by using the catalyst (enzyme is name in biochemistry) rhodanese they have. Some people may make less rhodanese and will get cyanide poisoning sooner.
I do not know the mechanism but as with all biochemical individuality I am presuming people have varying ability to excrete excess fluoride rather than send it to permanent storage somewhere in the body.
I want to develop a mathematical model which has a factor for a beneficial effect of fluoride, but a factor for an adverse effect when the individual has depleted their ability to remove excess for their needs. Effect of slow continuous uptake, approximated by fluoride in drinking water, would be included.
Looks like I may be summing several one-tailed or two-tailed distributions. A distribution will be produced which has varying kurtosis depending on input factors.
LikeLike
Soundhill, you seem to think you are writing a series of articles in the comments section of my blog.
Could you please put these in a more appropriate place – they are a blatant attempt at diversion from proper discussion of my own posts. They are also a cynical use of this blog much in the same way a cuckoo uses the nests of other birds.
I recommend you set up your own blog. That way you can post your articles as the main posts and ensure that there will be discussion around your own articles. It also means that you will be able to give your articles priority instead of burying them, like a cuckoo, in the depths of the discussion in others blogs.
Another plus is that your articles will be indexed by search engines, which will bring interested people to your blog. Certainly a far more preferable solution for you than attempting to take advantage other person’s blogs.
Have a look at wordpress.com. It offers blogs for free with a wide range of themes. The blogs are easily managed as all the work is done for you behind the scenes.
Another advantage of have your own blog is that you can manage the discussion to ensure that diversions are kept to a minimum by placing the “cuckoos” under moderation. Something I am tempted to do at the moment.
>
LikeLike
Pingback: Fluoride and Water Fluoridation - Hillside