Video produced by Calgarians for Kid’s Health which is campaigning for the return of Community water fluoridation to Calgary, Canada. Dr Ghali’s presentation to recent Calgary City Council hearings on fluoridation has been promoted by anti-fluoridation activists.
In my recent article Scientific integrity requires critical investigation – not blind acceptance I expressed some concerns with arguments presented by Dr Ghali in his presentation to the Calgary City Council. The video accompanying the article is one that the Fluoride Action Network and Fluoride Free NZ are using in their campaign against community water fluoridation. A campaign which currently concentrates on misrepresentation of recent fluoride-IQ studies – and resorts to blatant scaremonger.
I offered Dr Ghali a right of reply to my article and he has sent me the following. As it arrived in an email form I have edited it slightly but not changed any of the arguments.
I appreciate your indicating in your email below that you sensed that the recent video posted by the Fluoride Action Network might be presenting just a portion of my comments, without the context of my full presentation (and the presentation of key public health colleagues) at the recent City of Calgary committee meeting on community water fluoridation. That is indeed the case, and I would greatly appreciate your taking a look at the entire presentation if you have time to do so. Also, the presentation should be viewed in relation to the full O’Brien Institute report on CWF (that I attach for your convenience).
The link to the full special council meeting is below. Our O’Brien Institute presentations begin at approximately 17 minutes into the 9 hour meeting, and our main presentations last for 55 minutes followed by some Q&A. We then reappear as a panel (that includes AHS public health leaders) at about 6h40m into the video.
At a high level, we tried in our presentations to shed some light on the controversy, and to show how advocacy positions have focused on attacking both the evidence on benefits of fluoride (e.g., the multi-pronged attacks on Lindsay McLaren’s study on CWF), and the more recent evidence on potential negative cognitive effects in developing brains.
I must say that this journey into the fluoride issue has been quite eye opening, as it exposes the challenge of making sense out of a complicated controversy (– which is, interestingly, the name of your organization…[in my email I had included my position as a scientific advisor for Making Sense of Fluoride]). You will see in the opening part of my presentation to the City of Calgary that there is an interesting and extensive body of literature on the challenge of integrating science and advocacy (and balancing science vs. advocacy). The matter of CWF is a particularly challenging one in that regard, as the strong attacks on, for example, the CWF cessation studies (including Lindsay McLaren’s), are rooted in positional anti-fluoride advocacy, just as the unusually vigourous attacks on the fluoride cognition studies are seemingly rooted in the challenging findings of those studies (– both MIREC and ELEMENT are, after all, both NIH-funded prospective cohort studies unlike any of the prior cognition studies, that despite some limitations are clearly also more notable studies than the cognition studies that preceded them).
The O’Brien Institute was tasked with providing Calgary City Council with a non-positional description of the existing studies and evidence. The new cognition studies (led, interestingly, by two Canadian public health research teams) and the ensuing NTP draft report from the US are now such that it would have been absurd for us to pretend that the new studies do not even exist or that they are fatally flawed with irrelevant results.
Do watch the entirety of the City of Calgary CWF committee meeting, and let me know if you would like to have a chat some time. And thank you again for your email.
I am still concerned about the way Dr Ghali presents this issue but he also raises an important point about advocacy which needs discussion. So I will be responding to this post with a blog article ion a few days.
Ghali still refuses to view the science critically, instead naively continuing to take the studies at face value while implying that those who do critically evaluate them are simply attacking the studies out of biased advocacy. At some point he needs to wake up and understand his own limitations and failures with the O’Brien report. He needs to correct the misconceptions he has irresponsibly disseminated with that report and his subsequent dogged defense of it in the face of legitimate questions put forth by respected reviewers.
There is enough misinformation constantly put forth by antifluoridationists and their little groups, without Ghali adding to it.
Ken,
Integrity? Define: “The quality of being honest and having strong moral principles”
Keep in mind that every individual, fetus, infant, child, adolescent, teen, young, old, healthy, edentulous, dentate, chemically sensitive, are all being supplemented additional fluoride without their consent, without doctor’s prescription, with an unapproved drug, regardless that over half show signs of a toxic overdose of fluoride AND those who want to ingest fluoride can easily get it cheaper and by choice. And you call that public health policy “honest and having strong moral principles.” Don’t feed me your “integrity crap” while removing freedom of choice from millions. You can’t steel the moral high ground with ignorance.
While you keep in mind that too many are ingesting too much fluoride, let me quote Dr. Gahli:
“The new cognition studies (led, interestingly, by two Canadian public health research teams) and the ensuing NTP draft report from the US are now such that it would have been absurd for us to pretend that the new studies do not even exist or that they are fatally flawed with irrelevant results.”
And I would add, the USPHS recommended lowering fluoride concentration in water. . . why? Clearly, too many are ingesting too much fluoride.
And the NRC 2006 report advised the EPA to lower their MCLG which for 13 years the EPA has ignored.
And the EPA DRA, RSC clearly showed even if EPA standard for safety were to permit even more fluoride by 33%, still most of the young would exceed safety exposure levels.
Be careful Ken when you try to take the “moral, ethical integrity” high ground supplementing everyone with even more fluoride without their consent.
Ken, your fatal flaw is you refuse to include dosage in your narrow focus.
Studies of risk will always be weaker because highest quality studies to discover/prove harm are unethical. A different set of assessment skills are necessary. We must not be barbaric and do research like Hitler did.
Ken, I don’t think you appreciate or understand dosage, NOEL or LOEL.
TConsider, the difference between hazard and risk is dosage.
Quoting Stahlmann:
“This article starts with a few comments on the identification and assessment of toxicological risk to show why so many public debates lack the necessary risk competence. . .
“The main focus of pharmacology and toxicology is the desired and undesired or adverse effects of chemical substances on living organisms. One important task in this field is the identification of the basic mechanisms of action that means, the interaction between the chemical substance and the biological structures relevant for the effect at the molecular level. Understanding the toxicological effects of substances thus requires sound knowledge of physiology and biochemistry to answer the question about the mode of action of a poison or drug. . .
“The terms ‘hazard’ and ‘risk’ relate to completely different circumstances. Hazard, which should be understood in a qualitative sense, can be used for substances with a toxic potential. In contrast, risk should be understood in a quantitative sense because this term describes the incidence of an adverse effect at a certain level of exposure, hence a definable quantity. This definition is based on human data; thus, it retrospectively refers to a situation in which the damage to people has already occured. Prevention is not possible this way.
“In toxicology, two different approaches have to be distinguished: medical risk assessment and preventive risk minimisation. Both approaches ultimately help to reduce or prevent risk to human health. In risk assessment, dose-effect-relationships and definite incidence rates may be stated. In prevention, certain thresholds are estimated below which health risks can be excluded or considered ‘acceptable’. Prevention calculations are mostly based on experimental animal data and extrapolated to humans; thus, such calculations often include (un)certainty factors which are based on more or less secured assumptions. …
“Dose-effect-relationships in the low-dose range cannot be distinguished in experiments. For instance, determining an effect incidence of 1/100 or 1/1,000 with the required safety margin would require the examination of an unjustifiably high number of animals. Serious toxic effects affecting one in a hundred or one in a thousand people are not acceptable in most circumstances. For this reason, comparatively high doses are used in animal experiments, and the results have to be extrapolated from high to low exposure and from one species to another. The higher the gap between the experimentally investigated doses and the exposures to be reviewed, the higher is the uncertainty in extrapolation. It should be taken into consideration that high doses are often marked by several – and often interacting – effects, resulting in complex dose-effect-relationships. Because the course of a dose-effect-relationship curve in the low-dose range is unknown, a no observed adverse effect level (NOAEL) is initially determined, hence a dose for which no toxic effect can be found in the experiments. A safe range of exposure (for instance, acceptable daily intake – ADI) is then defined by means of an (un)safety factor. The applied factors are usually round numbers, such as 100, 300 or 1,000, which shows that these factors are not based on science but serve an administrative and political purpose. In the context of health politics, this concept appears rather appropriate because of often missing data on the mode of action of a substance and other knowledge gaps.
“Thresholds defined by different institutions or the legislature have both a regulating and a communicative function to prevent health risks and damage to the ecosystem. Risk analyses are mainly based on toxicological and epidemiological data. Four different phases have to be differentiated: Identification of potential hazard, analysis of the dose-effect relationship, analysis of the exposure and identification of populations at risk (Table 2 (Tab. 2)). Because of the general dose dependency of effects due to xenobiotics, thresholds have to be established for each substance, by which exposure irrelevant to health can be distinguished from exposure relevant to health. Thresholds in the low exposure range are often scientifically disputed. This range is marked by speculations because meaningful prospective studies, such as in drug development, are ethically not justifiable in most cases. However, retrospectively collected data often contain confounding elements, and the significance of such data is often somewhat overrated. Relative risks found in such studies have to be differentiated from risks found in the context of risk assessments that constitute incidences. A relative risk is the ratio of an exposed group and a control group.
Bill where is the integrity in Dr Ghali characterising my position as asking him “to pretend that the new studies do not even exist or that they are fatally flawed with irrelevant results.”
Of course that absurd and it is absurd of you to endorse his silly comment.
Bill, in spite of having had the nonsensical nature of your stale claims explained to you repeatedly, you continue to make them. Develop some integrity, man.
You make ad hominems and make personal attacks rather than attacking the facts. If you had the facts, you would present them.
Too many are ingesting too much fluoride. That is an undisputed fact which both of you would like to ignore, and the foundation for any discussion on fluoride. Any freshman student evaluating substances for benefit and risks, understands the essential foundation of dosage.
Steve, you say my “claims” are nonsensical. Well then, Ken and Steve, I’m listening, show your evidence. Show your facts. What evidence do you have that many are not ingesting too much fluoride? What about the question does not make sense to you?
Dosage. Too many are ingesting too much fluoride and that is undisputed and makes scientific sense. What about that question does not make sense to you?
Ken, I think you would agree there are different levels of confidence with different kinds of studies. For example, prospective studies are better than retrospective studies.
I presume you would agree human studies are better than animal studies (for human evidence.)
I presume you would agree RCT studies are better than ecological studies.
Please provide your RCT prospective human studies on efficacy of fluoride exposure for the mitigation of dental caries and please provide them for safety. There are none. No high quality studies and yet you persist in claiming efficacy at an unknown total fluoride exposure and safety at an unknown dosage is safe and effective. That makes no scientific sense.
Supplementation without consent in the USA of fluoride has been a public health policy for over 70 years with claims of efficacy and safety and yet the high quality studies are still lacking. Fluoridation has been an unapproved experiment without scientific evidence.
Understanding fluoride’s developmental neurotoxicity in the 2006 NRC report was only explored and postulated, they had little evidence. In the last 13 years we have many human and animal studies raising concern with over 80% consistently reporting harm. The quality of the studies are getting better and more consistent. What are the chances of new studies refuting the many studies reporting harm? Not great. Some have, but most raise serious concern. The trend is clear, fluoride is presumed a develoopmental neurotoxic substance according to the NTP.
Ken and Steve, you approach the subject from the position that consumers/patients/public must provide absolute proof of harm. That’s ass backwards.
The FDA is clear, it is the manufacturer who markets the product that must provide the proof of efficacy and safety at a recommended dosage.
Start looking for proof of safety rather than proof of harm, for each of the concerns listed in the NRC 2006 report.
Bill, you’re as predictable as the sun rising and setting each day. Always whining about non-existent “ad-hominems” against poor little you, in transparent attempts to make yourself out as some sort of victim whenever your nonsense is exposed for what it is. Perhaps that worked for you with your parents when growing up, but is unbecoming for adults. Stating obvious facts does not constitute “ad-hominem attacks”. If you wish to be treated as an adult, then act like one.
1. Because you make some unsubstantiated claim about people “ingesting too much fluoride” does not make this an “undisputed fact”. It makes it a
Bill Osmunson personal opinion.
2. Yes, dose and concentration are basic elements in discussing risk and benefit of substances. Unfortunately, you and Connett have never seemed to understand the difference between the two concepts or how they relate to fluoridation.
3. It is neither my, nor anyone else’s, responsibility to disprove your unsubstantiated claim that “many are ingesting too much fluoride”. It is your responsibility to back up such claims with facts and evidence….which you obviously cannot do. That said, the fact that your claims are nonsensical was in regard to the stale, meritless arguments of “consent, doctor’s prescription, unapproved drug, toxic, choice” etc, etc…..none of which have any relevance to fluoridation, all of which are constantly thrown out by antifluoridationists seeking to muddy the water with ridiculous nonsense in lieu of facts and evidence.
4. I do not agree that RCTs are better than observational ones in regard to assessing the effectiveness of a broad public health initiative such as water fluoridation. Just the opposite. RCTs are far too narrow and focused on the individual to make any such assessment. I will gladly, as I have on numerous occasions, provide you with a multitude of high quality observational studies clearly demonstrating the effectiveness of fluoridation in the prevention of significant amounts of very serious dental infection in entire populations.
It is very telling that you defend the agenda-driven Till, et al assembly line of antifluoridation studies, none of which are RCTs. Seems your faulty reliance on RCTs is highly selective.
5. Given the 75 year history of fluoridation, hundreds of millions having chronically ingested optimally fluoridated water during this time, with no proven adverse effects on anyone….given that there is no valid evidence that fluoridation is, in any manner, unsafe…… it is neither my, nor anyone else’s, responsibility to disprove unsubstantiated claims by antifluoridationists that the initiative is unsafe.
6. There is no “unknown dosage” involved with fluoridation. For every one liter of optimally fluoridated water consumed a dose of 0.7 mg fluoride is ingested. Ironically, it is the non-optimally fluoridated water for which you advocate in which the dose is unknown. In the US, this dose can legally be as high as 4.0 mg per every one liter of water consumed…..nearly 6 times the level allowed in optimally fluoridated water.
7. Your personal definition as to what makes “scientific sense” needs a lot of work.
8. The 2006 NRC did not list neurotoxicity as a concern in its final recommendations regarding water with a fluoride concentration of 4.0 mg/liter and below. If it had deemed this to be of concern at this level the committee would have been responsible for so noting and recommending accordingly. It did not.
9. Your uncited “many human and animal studies raising concern” are presumably those presented in the meritless fan petition to the EPA. Citing facts and evidence, EPA reviewers explained the invalidity, irrelevance, and misrepresentation by petitioners of those studies. If you haven’t read that rejection document you should do so.
10. The NTP has not presumed fluoride to be neurotoxic. That which you misrepresent is simply a non-reviewed draft put out for public comment. It does not represent any official NTP determination or policy.
“This DRAFT Monograph is distributed solely for the purpose of pre-dissemination peer review under the applicable information quality guidelines. It has not been formally disseminated by NTP. It does not represent and should not be construed to represent any NTP determination or policy.”
11. Given the 75 year safety record of fluoridation and the void of any valid evidence of “harm” it is indeed the responsibility of those such
as you who wish to discontinue this initiative to provide valid evidence to support your claims, not the other way around
12. The FDA has no jurisdiction over fluoride in drinking water. How it regulates the retail products under its jurisdiction is of no relevance to water fluoridation.
13. For the past 75 years, antifluoridationists have turned over every possible rock they could to find some kind of “harm” they could attach to optimally fluoridated water. They have had zero success.
Thank you Steve for a thoughtful response. I hope my response will stimulate some thoughts. I wish Ken could pull himself together and follow your example.
Each of your items should take many back and forth for clarity and understanding. I am torn between working on one item or doing more. Fluoridation is a huge subject with many streams of evidence.
Item #1. Too much fluoride. Yes, my opinion based on fact. For a start,
a. Do you dispute Millions have dental fluorosis? A biomarker of fluoride exposure.
b. Do you dispute the EPA’s Dose Response Analysis and Relative Dose Contribution of 2010 reporting at least a third or a half of our young are ingesting more fluoride than their suggested “safe” dosage?
c. Do you dispute the HHS lowered the concentration of fluoride in water? Was that enough and has it reduced dental fluorosis rates?
d. Do you dispute that mother’s milk contains much much less fluoride than fluoridated water? An infant on formula made with fluoridated water would far exceed the dosage of fluoride in mother’s milk.
If so, provide your evidence and reasoning.
Item #2. I and Connett keep pounding on those promoting fluoridation, that concentration is not dose. You say we don’t understand, then explain. I’m listening.
You add, “or how they (concentration and dose) relates to fluoridation. My exact thoughts about fluoridationists. The concentration of fluoride in water is not dosage of fluoride from water or total fluoride exposure. So please explain your thoughts.
I had to jump all over a Harvard Professor because he tried to confuse the audience claiming concentration of fluoride in water was a human dose. So it is with pleasure, I can agree with you that dose and concentration are not the same.
Simply put, water fluoridation is not a dose, it is a concentration. The dose would depend on how much water the person drinks. Some non-fluoridated and some (according the the NRC 2006) over 10 liters/day.
Would you agree that fluoridated water is not a controlled individual dose, rather it is a concentration?
Would you agree that water fluoridation represents only about one or two thirds of total exposure?
Item #3. I think we disagree on jurisdiction. I am confident no law or court or agency charged with oversight of any substance used with the intent to prevent disease requires the consumer, user, purchaser, patient to prove with scientific studies, efficacy, dosage and safety.
The FD&C Act places such responsibility on the marketer of the product to achieve FDA approval. Do you disagree?
Item #4. I would question your suggestion that observational studies are better than RCT in public health. Faster, yes. Cheaper, yes. I would suggest both are important but RCT have lower risk of bias. RCT are gold standard for research. Too often observational studies confirm bias or we miss confounders and unknowns.
A couple examples of my concern. The caries rates for 12 year olds in 1921 was about 11.5 per child. When fluoridation started with significance, the dental caries rates had dropped for 12 years old to about 5. A clear observation of prevalence and a significant decrease. However, I have not heard anyone explain what caused the decrease. Clearly, some major confounding factor(s) reduced dental caries. Let’s call it unknown “X”.
Would you agree, the chance that unknown “X” stopped exactly when fluoridation started is beyond reason?
Would you agree that any observational study would not control for unknown “X” and probably would control for in a prospective randomized controlled blinded trial?
There are several factors affecting dental caries, not just fluoride and the unknown “X” is just one problem with observational studies.
Most/many observational fluoridation studies do not include:
Socioeconomic status
adequate size
Difficulty and consistancy in diagnosing decay (today is much different than when I was in school)
Delay in tooth eruption
Diet: Vitamin D, calcium, strontium, sugar, fresh and frozen year round vegetables and fruit consumption not controlled.
Total exposure of Fluoride not determined
Oral hygiene not determined
Not evaluating Life time benefit
Estimating or assuming subject actually drinks the water.
Dental treatment expenses not considered
Mother’s F exposure, Breast feeding and infant formula excluded
Fraud, gross errors, and bias not corrected.
Genetics not considered and maybe a huge factor.
My one office observational opinion was very positive. I was convinced fluoride reduced dental caries. My bias was strong. Careful evaluation of the studies showed me where I was observationally wrong. A real kick in the gut.
I will admit my public health education was long time ago, but no professor suggested observational studies were stronger than RCT.
The second example of my concern over observational studies would be blood letting. The practice persisted because benefit was observed. And I will concede that too often RCT studies are later show to be false.
I think both are important and I defer to the FDA which requires RCT studies to increase their confidence for approval.
Perhaps I have gone on long enough and should address your other points in another post. Intellectual gymnastics is not my sport.
1. You concede that your claim was nothing but personal opinion, not “undisputed fact” as you falsely stated.
2. Yes, millions have dental fluorosis, the overwhelming percentage being mild to very mild, a barely detectable effect which causes no adversity on cosmetics, form, function, or health of teeth. While this is a biomarker of exposure to fluoride, it is not an indicator of overexposure. Peer-reviewed science has clearly demonstrated mildly fluorosed teeth to have increased decay resistance, with there being no valid, peer-reviewed scientific evidence of any adverse health effects from this effect.
—-The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren
Hiroko Iida and Jayanth V. Kumar
J Am Dent Assoc 2009;140;855-862
3. The EPA does not have “a safe dosage” of fluoride. This is a clear example of your lack of understanding of dose vs. concentration. The EPA has set a maximum allowable concentration of 4.0 mg/liter fluoride in water, not a dose.
4. The HHS did not lower the concentration of fluoride in water. HHS has no authority, or ability to do so.
5. By “mothers milk” it is assumed you mean human breast milk, the contents of which have no relevance to water fluoridation. Given that this milk is deficient in iron, vitamin K, and vitamin D to the point of requiring supplements of these substances for breast-fed infants, basing infant dietary needs on such content would mean that infants are meant to be anemic free-bleeders who develop rickets.
6. Your confusion of dose and concentration is clearly evident in my item #3 above.
7. Yes, the concentration of fluoride in water is not dosage of fluoride from water or total fluoride exposure. This elementary concept is self explanatory and requires nothing further in regard to my “thoughts”.
8. Yes, dose and concentration are not the same. Congratulations, you finally seem to be gaining some understanding of this.
9. Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans. The same is true of chlorine, ammonia, and the myriad other substances routinely added to public water supplies.
10. According to the CDC, of the total daily fluoride intake, 75% is from water and other beverages.
11. It is of no consequence whether you disagree with the facts or not. The contents of drinking water supplies are under the jurisdiction of the US EPA, not the FDA.
12. The effectiveness of population-based public health initiatives is not limited to individual effects. It is a measure of the total impact on the entire group. While fluoride does reduce significant amounts of dental decay, other factors may include greater dental awareness within the group due to knowledge of the initiative being in effect, resulting in improved home oral healthcare, more consistent visits to dental providers, dietary improvements, etc. The impact of all of these factors combined are best evaluated by observational studies of the whole population, not by RCTs. In addition, results of RCTs have been shown to have no greater quality than those from high quality observational studies.
“CONCLUSIONS
We found little evidence that estimates of treatment effects in observational studies reported after 1984 are either consistently larger than or qualitatively different from those obtained in randomized, controlled trials.”
—A Comparison of Observational Studies and Randomized, Controlled Trials
Kjell Benson, B.A., and Arthur J. Hartz, M.D., Ph.D.
June 22, 2000
N Engl J Med 2000; 342:1878-1886
DOI: 10.1056/NEJM200006223422506
13. If some “unknown X” is a problem with fluoridation effectiveness studies, it is much moreso with the poor quality observational IQ studies antifluoridationists so ardently defend. Given the highly complex factors involved in human cognitive development, the chance of unknown factors skewing results is far greater in those studies than in effectiveness studies. Again, your reliance on RCTs is highly selective, driven by your own confirmation bias.
I said, “my opinion based on fact.” You responded, “You concede that your claim was nothing but personal opinion, not “undisputed fact” as you falsely stated.” Please read what I say and don’t distort or twist.
Everyone has their opinion which is not always based on fact. And each person puts different weight on different facts.
And second, I don’t know of any science which is not disputed, especially fluoride.
Read what I write and try to understand. I don’t intend to argue.
We agree, dental fluorosis is a biomarker of fluoride intake. The dispute is whether the a biomarker of intake represents an excess of the substance. We agree most have mild/moderate. We agree cosmetic. But a higher intake than if they had no DF.
Historically when fluoridation was started, the public was assured fluoridation would only result in 10% or perhaps 15% DF prevalence. We are now at 40% to 60% depending on the survey and NHANES reports 20% moderate/severe. If 1% have severe DF of the more than 200,000,000 on fluoridation, that means over 2,000,000 have ingested too much fluoride. Would you agree?
Dentists have tried to minimize DF as only a potential “cosmetic” effect. . . as though fluoride only goes to the teeth and not to every cell in the body. We dentists and public health experts have not done safety studies to determine safety, We are marketing blind to our risks. For years we had neither observational or RCT studies on any risks.
However, I would maintain that even mild DF is an indication of possible excess fluoride for soft tissues, especially the developing fetus.
I do not dispute that studies exist which claim those with some DF have fewer caries and those with none or severe DF have more caries. Although the difference is minimal, there is a “sweet” spot of dosage which is probably beneficial in reducing dental caries. Not much reduction, maybe not any reduction, but probably some reduction.
In my presentations I show a graph of the data from Iida, Kumar publication which you reference above. The factual data indeed shows a slight reduction of caries but very hard to detect. And the effect could be one of several research limitations. For factual example, life time benefit is not considered.
Now that you have read those, please consider the EPA’s “RfD” or Reference Dose which is sort of an EPA “safe” dosage to prevent SEVERE DF. RfD is an EPA term.
Note, in the EPA documents they propose raising the RfD. In other words, the NRC 2006 said the EPA’s MCLG was not protective. Instead of determining whether their RfD of 0.06 mg/Kg bw was protective (safe) the EPA proposes 0.08 mg/Kg bw is safe, an increase of 33%. Their graphs then show about a third of children will exceed this new proposed RfD.
Steve, I don’t want you to miss the fact that EPA did the exact opposite of the NCR 2006 report and instead of making their standard more protective, they made their standard LESS protective in order to try and fit policy. And even cooking safety, the EPA shows millions of children will exceed their new proposed RfD.
If you read the EPA literature, you will back out of your statement that EPA does not have a “safe dosage.” That is precisely how the EPA came up with 4 ppm.
#4. You say HHS has no authority over fluoridation. The United States Public Health Service (USPHS) is a division of the Department of Health and Human Services concerned with public health. It contains eight out of the department’s eleven operating divisions. The Assistant Secretary for Health (ASH) oversees the PHS. The Public Health Service Commissioned Corps (PHSCC) is the federal uniformed service of the USPHS, and is one of the seven uniformed services of the United States.
PHS recommends for those who choose, “For these community water systems that add fluoride, PHS now recommends an optimal fluoride concentration of 0.7 milligrams/liter (mg/L).”
0.7 mg/L is a reduction. The reduction is clear admission that some were ingesting too much fluoride.
#5. Geee. You are down on breast milk. Our species would have died out if not for Mother’s milk. OK, APA says mother’s milk is the ideal nutrient for infants which all other substitutes should be compared.
And the Infant Nutrition Council of NZ and AU state:
“Breastmilk is uniquely superior for infant feeding. It is the normal food for infants from birth.
“Breastmilk contains all of the essential nutrients, antibodies and other factors important for growth and development. It cannot be replicated.”
As a Nutritionist, I would maintain that the quality depends in part on the mother’s diet and quantity needs to be adequate. And the infant needs sunshine.
#6. If I am confused on dose and concentration, please explain your understanding. Concentration for fluoride is usually listed as mg/L or ppm. Dose is mg/KgBW.
#7. We agree.
#8. Snarky response is not called for.
#9. Wow, please provide references for, “Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans.”
#10. CDC is correct for some individuals. Read the EPA’s DRA and RSC and NRC 2006 report on total exposure.
#11. According to EPA’s legal counsel, FDA has jurisdiction because Congress has prohibited EPA from adding anything to water for the treatment of humans.
I am an Assistant Professor at the University of Alaska Anchorage Division of Population Health Sciences. In the July 2019 O’Brien Report on community water fluoridation (CWF), your team referenced a paper that I coauthored and conducted in Juneau, Alaska. I studied the health and economic effects of CWF cessation. Fluoridation is a concern in Alaska (as it is in Calgary) because two of Alaska’s largest cities intentionally ceased long-standing CWF programs. The percent of Alaska’s population served by CWF in 2007 was 65% but fell to 49.3% in 2014 and remains so today because of local municipal policy changes fueled by misinformation about fluoridation. CWF misinformation is almost always supported by ‘scholarly’ citations.
As a nurse, mother to three small children, professor, and public health researcher, I read with keen interest the maternal fluoride – IQ study published in JAMA Pediatrics. I agree with the statements you made: that the study was funded by one of the NIH institutes, that it was reported in a well-known US medical journal, and conducted by a primarily Canadian team. However, those descriptive attributes don’t ensure quality or scientific rigor.
It is of concern to me that rather than addressing the modeling and statistical analyses conducted by the authors, you instead discuss the funder, journal, and location of the researchers. I could not find in the O’Brien Report, or by listening to your public testimony, your assessment of the quality of the data presented in the study or your reaction to the post-publication reviews. Isn’t that what the Calgary city council asked you to do – that is, to inform the council members about the quality of the scientific evidence?
You stated at the Calgary City Council meeting that, “The study exists and we can’t make it go away.” But you and your team know as well as I do that the fact that the study ‘exists’ is hardly the point. The point is a shared duty to assess the quality of the research for people who don’t have our scientific training.
Typically, scientists judge a study, or group of studies, not only through the peer review process but also by post-publication reviews. Only through scientific scrutiny and careful study of the methods and statistical analysis can a study’s worth be known. Such work of course takes time. Now that the post-publication reviews of the Jama/Peds F-IQ article are available, it is instructive to read them. Here are some:
The Canadian Agency for Drugs and Technology in Health (CADTH) reviewed the study and stated, the authors’ “conclusions were not supported by the data.” My goodness, isn’t that just about the worst thing that a prestigious agency could say about a paper?
You might also know that I was one of the 30 researchers from 6 different countries who co-wrote and signed a letter to the funders of this research group, the National Institute of Environmental Health Sciences. We sought the data from the study to re-evaluate the analysis and conclusions. This is a reasonable request from scientists who are concerned enough to seek the opportunity to replicate the study. I did not take personal offense when you misrepresented the purpose of the letter to the Calgary City Council and disregarded its details. None of this discussion is ‘personal’ or ‘agenda-driven’, as you claim. It is science-driven. Science does not care about ‘balance’, ‘middle ground’ or ‘both sides of a debate’. It cares about truth, facts, and accuracy.
I didn’t even take personal offense when you called the signers of the letter a bunch of liars at the city council meeting because I know you were simply misinformed. My concerns about the science underpinning fluoridation are professional. The fact that the CADTH has already negatively assessed the study means that the Jama/Ped F-IQ paper is almost certainly fatally flawed and cannot be relied upon. Yet since CADTH released its report, the O’Brien CWF Report has not been updated. I hope that you will revise the O’Brien Report to address the salient points. The public does not need to know who published the paper, funded it or wrote it, but rather whether the paper presents scientifically plausible and reliable evidence. Wouldn’t you agree?
From one health care professional and academic to another, I am asking you to please review the statistical analyses presented in the Jama/Peds F-IQ paper along with the post-publication reviews when you and your team update the O’Brien Report. I have placed below my signature 12 points that specifically concern me about the quality of the study and which I hope you will consider.
I am sure you would also agree that, while it may be uncomfortable for the leader of a public health institute to revise a report already published, your team’s pride can easily be set aside to correct a document when the health of children and community members are at risk.
Thank you very much for reading this post. I believe that you and I entered the health care and health research profession because we want individual’s families and communities to benefit from scientific advancement, all of which must be based on high-quality replicable studies.
Respectfully posted,
Jennifer Meyer Ph.D., MPH, CPH, RN
Assistant Professor
UAA College of Health
Division of Population Health Sciences
ps, I’d be happy to chat with you sometime about the above questions Dr. Ghali. Please don’t hesitate to reach out. Wishing you and your family a peaceful and joyful holiday season.
1. Please comment on the concerns noted by numerous experts about the unacceptably large confidence intervals in this study. As I recall, most (maybe all) bordered or included zero. Does that concern you?
2. The study does not consider whether the effect is nonlinear. As noted by others, multi-level modeling would have allowed for this type of investigation. Why do you think multi-level modeling isn’t being utilized?
3. What about the lack of adjustment for multiple hypothesis testing. Do you wonder why the authors didn’t do that?
4. The unadjusted IQ differences were not significant – does that concern you?
5. None of the exposure measures are validated, and even the authors acknowledge that fact. Can you please help me understand why more caution wasn’t exercised in the interpretation of the results?
6. Do you think it was strange the authors didn’t report the main effect finding for maternal urinary fluoride (MUF) and IQ? This is a violation of STROBE guidelines which I imagine you must certainly familiar with? Guideline 16 to be specific. Why do you think they didn’t include that? Also, does it seem odd that the Jama/Peds editors didn’t require the authors to conform to the guidelines? Does that make you wonder about the quality of the peer review?
7. Did you read the National Toxicology Program draft monograph on fluoride or simply rely on others to tell you what it said? I found it curious they included several studies as ‘low bias’ when the studies all share similar critical flaws, such as the ones identified in the Jama/Peds F-IQ article and other articles affiliated with the Jama/Peds F-IQ authors. These are as described earlier and include no adjustment for multiple testing, no adjustments for cluster sampling, and of course no multilevel modeling. Please be careful to note that this draft monograph has not been validated and on each page, the NTP authors write, “this DRAFT Monograph is distributed solely for the purpose of pre-dissemination peer review and does not represent and should not be construed to represent any NTP determination or policy.”
8. Were you worried about the cluster sampling method not being considered statistically? I found it very unusual the authors included IQ scores within 2.5 standard deviations or 98% of the scores. Including all the scores in a logistic regression means extreme values could have a lot of influence on the model. And look at all the low scores, those in the range of 50-70, they are all boys. Do we know if those boys all came from the same area or cluster? These might have been listed as clusters A, B, C, D, etc. But they were not listed given that there was no accounting or adjustment for cluster sampling.
9. Did it bother you in the FI analysis that they excluded 1 of every 3 mother-child pairs with and IQ test? That seems high? Researchers must work with the data they have of course, but wouldn’t it have been helpful to have a comparison sample note if there were any differences between those included and those excluded?
10. How about the r2 values and the outputs from the regression analysis? Did you find it unusual they were not presented in the supplementary materials? I wonder why they were not presented. Typically, in a paper, we aim to present all the findings.
11. What about the actual sign change noted in the results for MUF and IQ for boys and girls? A small difference between genders might be acceptable, but an actual sign change from – to + seems very unusual.
12. While I am not a physician, experts in nephrology seem very concerned about the inaccurate measures for urinary fluoride. Dr. F. Perry Wilson, a nephrologist at the Yale School of Medicine, criticized the Jama/Peds F-IQ article for relying on urine samples “because urine fluoride is not a perfect proxy for blood fluoride.” What do you think of his concerns?
1. Obviously, you are the one who needs to read your comments and “not distort and twist”.
I draw your attention to your previous comment in which you state:
“Too many are ingesting too much fluoride. That is an undisputed fact which both of you would like to ignore, and the foundation for any discussion on fluoride.”
As you conceded in your second comment, this is not an “undisputed fact” as you falsely claimed. It is simply your unsubstantiated personal opinion.
2. “And second, I don’t know of any science which is not disputed, especially fluoride. Read what I write and try to understand. I don’t intend to argue.”
You’re contradicting yourself. You’re the one who claimed it was “an undisputed fact”. You’re the one who needs to read what you write.
3. In regard to the NHANES data to which you refer, the The National Center for Health Statistics has found this data to be unreliable and not reflective of any real increase in dental fluorosis over time.
“The analysis of the synthetic cohort with adjustment for possible changes in the demographic characteristics of the population over time suggests that the observed increase in fluorosis prevalence does not reflect the genuine amount of change within the U.S. population.” Indeed, the observed increase in the prevalence of dental fluorosis over time suggests that the way the examiners evaluated the level of fluorosis changed over time and the data do not reflect a real increase.”
—-AADR Response to New NCHS Evaluation of Dental Fluorosis Clinical Assessment Data from NHANES Over Time
American Association for Dental Research (AADR)
April 22, 2019
4. There is no valid, peer-reviewed scientific evidence of any risk of adverse effects to any “cell of the body” in association with mild dental fluorosis. The 2006 Committee on Fluoride in Drinking Water which you so frequently misrepresent, was composed of a variety of healthcare personnel and researchers. It, too, found all but the severe level of dental fluorosis to be cosmetic in nature.
5. What you “would maintain” in regard to mild dental fluorosis is groundless, meaningless and irrelevant.
6. Your unsubstantiated, unscientific guesswork in regard to caries reduction in mildly fluorosed teeth is meaningless and irrelevant.
7. Your personal critique of Iida and Kumar is groundless and without merit.
8. The only “safe fluoride exposure” set by the EPA is a maximum of 4.0 mg/liter in water. This takes into account exposure from all other normal sources of fluoride.
The EPA’s Dose Response Analysis identifies 2.0 mg/liter fluoride in drinking as the point of departure for risk of severe dental fluorosis. This is consistent with 2006 NRC finding that severe dental fluorosis does not occur in communities with a water fluoride level below 2.0 mg/liter (pp 114). This POD is 3 times the level of fluoride in optimally fluoridated water.
9. The 2006 NRC found 4.0 mg/liter to not be adequately protective for but 3 stated reasons:
a. risk of severe dental fluorosis
b. risk of bone fracture
c. risk of skeletal fluorosis
As noted by this committee, severe dental fluorosis does not occur with a water fluoride content below 2.0 mg/liter. Water is fluoridated at one third this level.
Bone fracture risk is a U-shaped curve, increased risk occurring with too little or too much fluoride intake. The point of least such risk is at the bottom of the U, in the range of the optimal concentration.
Skeletal fluorosis is so rare in the 74.5% fluoridated US as to be nearly non-existent.
10. There is no valid, peer-reviewed scientific evidence of any adverse effect resultant of “millions of children” exceeding an RfD of fluoride. Mild dental fluorosis is not an adverse effect.
11. “If you read the EPA literature, you will back out of your statement that EPA does not have a “safe dosage.” That is precisely how the EPA came up with 4 ppm.”
I see nothing here that warrants my backing out of anything. You simply exhibit, yet one more time, your lack of understanding of dose versus concentration. 4 ppm is a concentration, not a dose. It can therefore not be an EPA “safe dosage”.
12. In your comment, you asked: “Do you dispute the HHS lowered the concentration of fluoride in water?“.
HHS does not raise or lower the concentration of anything in drinking water. It has neither the authority, nor ability, to do so. To what you are attempting to refer is a recommendation by HHS as to the optimal concentration of fluoride in drinking water. There was no reduction in the 2015 reset of the optimal level recommendation. Due to recent science showing there to no longer be a difference in water consumption due to climate differences, HHS simply eliminated the previous optimal range of 0.7 ppm to 1.2 ppm set in 1962, and replaced it with a single point at the low end of that range, 0.7 ppm. With more sources of fluoride exposure now, than in 1962, HHS determined that the low point of the range would be sufficient to provide the same level of dental decay reduction, with no adverse effects. Thus was entirely in keeping with the original policy of setting the optimal as low as possible to allow for maximum decay reduction with no adverse effects.
13. I see nowhere that I am “down on mother’s milk”. I simply stated facts about human breast milk which you omitted.
“Overall, human breast milk has been found to be low in certain nutrients in developed countries: vitamin D, iodine, iron, and vitamin K.”
—-Med Hypotheses. 2018 Feb;111:82-89. doi: 10.1016/j.mehy.2017.12.020. Epub 2017 Dec 14.
Breast milk is conditionally perfect.
Erick M
Again, if you consider human breast milk to be the sole determinant of dietary requirements of infants, without supplementation, then you believe infants should be anemic free-bleeders who develop rickets.
15. “If I am confused on dose and concentration, please explain your understanding.”
See my item #11 above. It clearly exposes your lack of understanding of dose and concentration.
16. “Wow, please provide references for, ‘Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans.’ “
—-J Clin Pathol. 2003 Oct; 56(10): 803–804.
Fatal water intoxication
D J Farrell1 and L Bower2
17. “CDC is correct for some individuals. Read the EPA’s DRA and RSC and NRC 2006 report on total exposure.”
That you deem the CDC be correct gives me great comfort, as I’m sure it will the CDC.
18. The EPA does not add fluoride to drinking water, nor does it mandate it be done. It simply regulates the concentration level of this and other contents in such water supplies. Fluoridation decisions are made on the state and local level. There is nothing in the law which prohibits this.
Because there can be no federal mandate of addition of substances to water other than for treatment of the water does not magically convey jurisdiction of drinking water supplies from the EPA to the FDA. Your “logic” in making this claim is bizarre even for you.
They mention 0.05 mg/kg/day and I get the impression they think that is safe and effective. EPA uses 0.6 mg/kg/day.
Please go to Table 8-1 of your reference on Dietary Reference for fluoride.
13 studies are listed in Table 8-1. “Non-fluoridated” dose does not exceed 0.04 mgF/Kg body wt/day.
However, 5 studies have “mean” of 0.05 and 8, let me repeat, EIGHT of the 13 studies show excess fluoride dosage for many ranging from 0.7 to 0.13 mgF/kgbw/day
I presume you understand “mean”. 8 studies had many over 0.6 and some more than double EPA’s RfD of 0.6.
In other words, your data confirms my claim that many are ingesting too much fluoride. If you agree with your reference, you would agree, many are ingesting too much fluoride.
My definition of “many” would be more than 0.5%. Half a percent of 1,000,000 would be 5,000 children.
Your data suggests most studies would suggest 50% of more are ingesting too much fluoride, perhaps 500,000 children out of every million. In my book, that is “many.”
1. UL for Infants 0 through 6 months: 0.7 mg/day
UL for Infants 7 through 12 months: 0.9 mg/day
UL for Children 1 through 3 years: 1.3 mg/day
UL for Children 4 through 8 years: 2.2 mg/day
Older Children and Adults Ages > 8 Years: 10 mg/day
Overexposure would be that which is above the threshold of adverse effects. As you can see 10 mg per day is the daily upper limit of fluoride intake before adverse effects for everyone above the age of 8. For those below this age, it is considerably lower, but due only to the risk of mild dental fluorosis in developing teeth, as evidenced by the huge increase in UL after teeth developing years 0-8.
2. Your inability to address my exposure of the fallacies of your other claims is taken as your concession to this.
Steve, you state: “Your inability to address my exposure of the fallacies of your other claims is taken as your concession to this.” Second grader logic. Grow up. Just because I don’t have time to constantly repeat myself because you don’t read, doesn’t mean you can also put words in my mouth.
I don’t have time to do all your research for you.
Yes, DRI lists fluoride as a nutrient and has an UL. However, I have serious reservations on the DRI
First, look at the date of the DRI. 1997. In the last two decades has there been any research on fluoride safety/efficacy published? Hundreds of studies.
Then look at the areas of expertise of Panel members. Nutritionists mainly. Where were the toxicologists and pharmacologists or even dentists? None that I can see. In any panel of members, the conclusion will reflect the training and bias of those members.
DRI defines, “UL = the maximum level of daily nutrient intake that is likely to pose no risk of adverse effects to members of the healthy general population. Unless specified otherwise, the UL represents total intake from food, water, and supplements.”
The term “likely” is used for “healthy general population.” Does not sound either scientific or confident to me. However, nutrition is not a precise discipline and has numerous variables.
Are we only going to protect the “healthy” population? To hell with those having kidney problems, other toxic overdoses with lead, etc. To force everyone to ingest more fluoride when they are not healthy would not be supported by the DRI.
One of my majors in MPH was nutrition.
Nutritionists are frustrated because they can’t prescribe and we all want to “do good” “help people.”
Nutritionists did not consider the toxicity of fluoride, the evidence was and still is incomplete. Fluoride is highly toxic and fits within the definition of poisons, highly toxic substances. As such, it is regulated and permitted under two jurisdictions, pesticides and drugs. No nutrient is so highly toxic as to fit within toxic poison laws.
The absence of fluoride does not cause any disease. A nutrient is required to prevent disease, such as Vitamin C to prevent scurvy. Dental caries is not due to an inadequate intake of fluoride.
Fluoride may mitigate caries but does not prevent caries like Vitamin C prevents scurvy.
What is the UL of fluoride for the fetus? DRI does not include the fetus.
The UL was selected not on research of efficacy and safety but with the intent to protect the policy of fluoridation. Assumption was made.
A six month old infant drinks about 1 liter a day, so the UL was selected as . . . oh, let see, 1 X 0.7 would be 0.7 mg. So they chose that number. Not based on safety or efficacy but on policy and the best evidence they had at the time.
(Correction on my last post. Whitford at the bottom of the list was on the DRI. I wonder if he would stand by his approval two decades later.)
Grandjean is one of the worlds top researchers of toxic substances. A prolific Harvard and Danish University published expert.
Fluoridation’s days are numbered. The question is how many children do we need to harm before we stop the excess.
Grandjean, P. Developmental fluoride neurotoxicity: an updated review. Environ Health 18, 110 (2019) doi:10.1186/s12940-019-0551-x
“Conclusions
Previous assessment of neurotoxicity risks associated with elevated fluoride intake relied on cross-sectional and ecological epidemiology studies and findings from experimental studies of elevated exposures. The evidence base has greatly expanded in recent years, with 14 cross-sectional studies since 2012, and now also three prospective studies of high quality and documentation of individual exposure levels. Thus, there is little doubt that developmental neurotoxicity is a serious risk associated with elevated fluoride exposure, whether due to community water fluoridation, natural fluoride release from soil minerals, or tea consumption, especially when the exposure occurs during early development. Even the most informative epidemiological studies involve some uncertainties, but imprecision of the exposure assessment most likely results in an underestimation of the risk [86]. Thus, the evidence available today may not quite reflect the true extent of the fluoride toxicity. Given that developmental neurotoxicity is considered to cause permanent adverse effects [69], the next generation’s brain health presents a crucial issue in the risk-benefit assessment for fluoride exposure.”
The published review is excellent with over 150 references.
Bill, Grandjean has a bias about water fluoridation – it’s no accident that he is often called on by FAN to make statements. Those statements are well outside any research he has personally done.
The current article is simply a review – all he has contributed is an interpretation driven by his bias.
Nevertheless, I must give him credit for actually including my paper in the section on Mailin & Till (2015) where he says:
“However, the study has been criticized, as the inclusion of mean elevation as a covariate apparently abolishes the significance of fluoridation as a predictor [130].”
Mind you he does not draw the obvious warning that many other studies suffer the same fault of not including important risk-modifying factors.
My paper has studiously been ignored by the Till crowd. They are quite aware of it – I know they have read it – but they dishonesty always refuse to cite it and still present their paper as if it was not flawed.
So good on Grandjean for not behaving the same way. But it is very ironic as he absolutely refused to allow my paper to be considered for the journal he controls -Environmental Health.
Interesting to look at who peer-reviewed Grandjean’s paper though. I suspect if it had been open to a more objective review he would have been told to reduce the basis of his conclusions.
Mind you the manipulation of peer reviewers is, I think, a widespread problem in scientific publication and should really be dealt with (in my time we didn’t get to choose oru reviewers as many journals now allow). But I have never seen anything as blatant as this particular peer review.
Ken,
And we all have some bias based on the science we review and understand. That is one reason we disagree. Another is thick headed stubborn obstinate pride.
You complain about Grandjean, “he absolutely refused to allow my paper to be considered for the journal he controls -Environmental Health.”
Yet you refuse to publish the paper I sent to you and then attack me, calling me a liar.
Well known when the science does not support the bias, the messenger is attacked.
But you don’t publish mine because you can’t refute the facts. Too many are ingesting too much fluoride and you know it.
You can’t refute the fact that we don’t know how much fluoride is needed to prevent or mitigate caries (if any) and we don’t have safety studies.
In the USA no government agency accepts jurisdiction for determining the dosage, efficacy and safety of fluoridation.
Fluoridation’s days are numbered. In the near future we will look back on fluoridation like we do mercury treatments and blood letting.
1. Your continued inability to address my exposure of the fallacies of your claims is so noted. Your concession stands.
2. Yes, you obviously don’t have time to do any research, as evidenced by your comments.
3. Your unsubstantiated personal opinions on National Academy of Medicine DRI are meaningless and irrelevant.
4. There is no valid, peer-reviewed scientific evidence of any adverse effect of optimally fluoridated water on “those having kidney problems, other toxic overdoses with lead, etc.” or anything else.
5. There is no valid, peer-reviewed scientific evidence of any toxicity of fluoride at the optimal level at which water is fluoridated.
6. Fluoride in public water supplies is under the jurisdiction of the EPA, not “pesticides and drugs”.
7. Yes, dental caries is not caused by an inadequate intake of fluoride, any more than is polio caused by an inadequate intake of the Salk vaccine. Dental caries is caused by acid secreted by oral bacteria. Fluoride renders teeth more resistant to this acidic destruction.
8. There is no valid, peer-reviewed scientific evidence of any adverse effect on the fetus from optimally fluoridated water.
9. Your ridiculous claim for the reason of establishment of fluoride UL is meaningless, irrelevant, and an obvious product of your confirmation bias.
10. The lack of usefulness of NAM DRI to you is not surprising. Scientific evidence has never been of much use to antifluoridationists.
You then did not respond to my request of including references and correcting a figure (you obviously had not put together the document properly).
If you had done that small amount of work on your contribution our discussion would have gone ahead.
Surely I dot have to, yet again, provide the email exchange between us exposing your lies?
Surely you are not so inept that you couldn’t have corrected the document. I do not know why you decided to renege and pull out of our discussion but it is simply a repeat of a similar incident when you were director of FAN – see Do we need a new fluoride debate? and New fluoride debate falters
I have no problem discussing the issues raised in your contribution -especially as the work you referred to had been found deficient. I will no doubt deal with the paper you co-authored with Neurath at a later date – but the current propaganda on the IQ-fluoride issue is far more important.
When I do deal with the Neurath et al paper you will be able to comment – but your lies about this attempted exchange and your claim I am funded by “Russia” to ensure that fluoridation continues in the US so that American’s IQ is lowered simply show you are not fit for a proper open good faith scientific exchange. You are simply a buffoon.
Any chance of such an exchange with you here is completely off the table because of your lies and slander.
Ken,
OK, the document I sent you and you have refused to publish.
Because you don’t have the science, the facts, to refute the undisputed fact that too many are ingesting too much fluoride, you attack me and call me a liar.
Name calling is not science.
Every research I’ve heard you talk about is “deficient.”
Maybe you could provide a research paper which meets your standards. Demonstrate quality.
You lie again Bill, I did not refuse to publish at all. Do you want me to post the email chain of our communications at the time yet again?
You cannot find any evidence that I refused to post your article – you were the one who effectively refused to do the formatting, et., required for posting.
I am tempted to post the email chain as an article so that you are more widely exposed. However, I really don’t think anyone cares about this issue – your reputation is really bad.
Ken,
Fact: You asked to debate me on an article, communication, paper or document. You are playing with words in order to slander me. Lets call it a document.
Fact: I said we needed to start at the basics. You at first refused.
Fact: You then agreed and asked me to send you my document.
Fact: You wanted format changed.
Fact: I said it is OK as is and you can change format if you require for posting. Your choice.
Fact: You have not posted it. Refused, delayed, avoided, or what ever term you chose, and then slander me.
Fact: You simply attack the person, name calling, because you do not have the science to back up your bias. You change the subject because you lack science. You evade and avoid the tough questions and streams of evidence which do not confirm your bias.
Fact: you have not disputed that too many are ingesting too much fluoride. Instead you resort to slander and avoid science.
Fact: You have not provided an example of any research on safety/harm on any subject which you find to be ideal, great research, your gold standard without flaws. Show us an example of perfection.
Fact: You do not understand the study of human safety must be ethical and with individual consent. Giving people highly toxic substances to see how and at what dosage they are harmed is problematic, unethical and illegal . . . even with consenting prisoners. It appears, in your world, everything is safe unless you have the highest quality of science finding people are harmed. Those kinds of studies were done historically and are not ethical. A person cannot consent to being harmed.
Fact: you don’t have the science or laws on fluoride exposure to back up your bias.
In other words, Ken, you have not looked at the studies on efficacy. None are of good quality. Yet you expect the highest quality of study on harm/safety. You have a double standard.
You sound like one of Putin’s bullies. Stop your name calling and get back to science.
Too many are ingesting too much fluoride. . . and you have no reasonable science to refute that claim. You are overdosing millions.
Steve,
Instead of providing quality evidence that millions are not ingesting too much fluoride, you attack me.
“An ad hominem argument (or argumentum ad hominem in Latin) is used to counter another argument. … An ad hominem argument is often a personal attack on someone’s character or motive, rather than an attempt to address the actual issue at hand. This type of fallacy is often witnessed in debates in courtrooms and politics.”
At first Ken cautioned against ad hominems. That caution appears to have been removed.
Without the science to support your flawed theory, you guys only have personal attacks left.
My request for the word version was not a whim – as you can see a pdf version simply cannot be posted as text.
I asked for the word version. I also asked you to provide references and links (these are not included in the document). I also asked you to provide proper images – for example, this image is faulty:
Other images are simply copied from a paper – one should at least remove the caption or describe the image in the text. for example your fig 5:
No, you did not hand this problem back to me – “you can change format if you require for posting. Your choice.” You undertook to do what I requested and then did not follow through.
As I said, one cannot post a pdf document (except in the way I have done in this comment). You refused to do the work required to make it available for posting. I suspect because you did not actually have the original word document or images for some reason.
So you simply lied – saying I “refused” to publish it – an outright lie.
I will, of course, cover Neurath’s paper in future – no rush as it has already been dealt with by others who show that the claimed increase of dental fluorosis is biologically impossible. I will cover the paper my way. You are obviously incapable of preparing a proper document for posting.
But because of your persistent lies about this – and your childish slander – claiming I am paid by “Russia” – there is no way I will ever repeat my offer of a scientific exchange with you because you are clearly incapable of such an open good-faith exchange.
Ken,
I simply asked if Russia was behind/supporting your bias for overdosing so many with a highly toxic substance. Just asking.
If not, then perhaps a careful evaluation of dosage and efficacy will provide a background for judgment on safety.
And thank you for linking the document I sent you regarding excess fluoride exposure.
I look forward to your and Steve’s response.
Bias is strong. You suggest a “sensible person is very wary when. . . ”
I would add, a sensible person is very wary with all facts, especially from governments and those with vested interests. It is long past time for you to be wary of claims of “safe and effective” with the addition of fluoride exposure to everyone’s diet.
EPA’s DRA/RSC which I have frequently mentioned here has this graph which I have repeatedly talked about, Fig 8-1 above in your post and link.
As you can see, about a quarter to third of children are ingesting more fluoride than the EPA’s PROPOSED RfD (safe level).
And further, note infants are ignored.
And note this graph is based on a proposed increase of the RfD from 0.06mg/kgbw to 0.08 mg/kgbw. In other words, EPA was evaluating that even if they raised the RfD, many would be harmed. The current RfD would have the black line even lower showing even more harmed.
Those are not “anti-fluoridation” facts, those are EPA facts.
Con off it bIll, it is disgusting to pose such a question and you know it. It is simply slander and complete negation of any good-faith scientific exchange. IUnforutantley this sort of childishness seems to be permitted in the USA – it is being used because people can no longer discuss political issues sensibly.
It linked to your document (notice that you never did – I wonder why) simply to show that is was not in a state for posting here. And you simply refused to put into such a state. You have still not apologised for lying about this whole issue.
You had your chance of a proper discussion of these issues here and you blew it. You will not be given another chance here because you have behaved in an unacceptable way – lying about the issue and slandering me personally.
It is simply not worth entering into any discussion with someone who behaves this way.
Lost my chance to change the document, is it. Science has such tight schedules and deadlines. I never felt you would publish it anyway. You don’t like to publish what doesn’t support your bias. Would be a waste of my time to have changed it and I’m busy. You never planed to publish in the first place. Over exposure doesn’t fit within the belief system of fluoridationists.
Doesn’t sound like you read the document before or recently. For example, you say, “Other images are simply copied from a paper – one should at least remove the caption or describe the image in the text.”
And I did explain it, starting before and after the graph. Yes, a copy and paste from the EPA’s DRA 2010 with reference.
Why do Ken and Steve persist in ignoring all streams of evidence or starting at the fundamentals, dosage?
Why do Ken and Steve persist in supporting overdosing of millions with a highly toxic substance, lacking high quality efficacy or safety studies, against their freedom of choice?
Good scientists, evaluating the same information, should come to a similar conclusion. Clearly, we are not evaluating the same information and you have refused to examine dosage.
Hierarchical evidence is a house of cards. Science fiction is often built on one single unknown, a time many years in the future. The story seems reasonable if we can accept that one unknown.
The same with fluoridation Accept the one simple unknown, dosage, and the story seems reasonable for many.
Too many are ingesting too much fluoride. The concept is undisputed. The only question is how many are being harmed.
You state: “Too many (people) are ingesting too much fluoride.”
So, amongst those millions of people, over more than seven decades of Community Water Fluoridation, according to you there must be at least one person who has been harmed by CWF (apart from the cosmetic harm of tooth fluorosis).
I invite you to provide the evidence that this has actually occurred.
Don’t be silly Bill. I willingly published Paul Connett’s material despite its poor science. It provided an ideal opportunity to discuss the issue.
I would have published yours if it was properly formatted – no problem. Even though you were the Director of FAN at the time you don’t exactly have the abilities or standing Paul has and his articles here did not intimidate me. Why should yours – or do you think you are somehow better than Paul? Is that why you were replaced by Paul again after a short period as FAN director. Your boots (and head) got too big for you?
And I do not recall Paul sinking so low as to pull the McCarthyist “Russia” bogyman on me. That was certainly the pits. What a pathetic mind you have.
Which intimidates any fluoride promoter who seriously looks at the scientific facts.
The Russia financing came from another person here. You failed to answer and I began to wonder what pushes your motivation to force so many into unwanted ill health. So I asked and you failed to respond. A simple “no” would suffice. Instead you tell stories and evade the answer.
Too many are ingesting too much fluoride. You have evaded the concept of dosage. The only reason I can think of is because you don’t have science to back up giving everyone more fluoride.
For about 25 years as a dentist I promoted fluoridation or fluoride supplements. I pushed the drug. Safe and effective, so I never spent the time to look or ask. Why should I look for something that CDC and ADA claim do not exist.
When I started to speak out against over exposure, that is when some came to me and explained their problems with fluoride.
Where endemic fluorosis exists, we know some of the early signs which include arthritic like symptoms, sore joints, enlarged joints. Which people with arthritic like symptoms have fluoride exacerbating or causing the pain? We have failed to diagnose and don’t know.
You ask about individuals. I’m very skeptical when a person says their dermatologist has told them not to use fluoride toothpaste and when they stopped their angular cheilitis cleared up.
Or the mom who took her high school daughter to HS sports competitions in various cities. After the hotel shower, mom sometimes noted a rash on the daughter. The next day she would call the water purveyor and ask if the water was fluoridated. Yes. However, never a rash with just chlorine.
Apparently some individuals are more chemically sensitive than others. Seems to run more often with autistic kids.
Here is a mom’s report of her autistic son. Three parts and I’ve condensed it here.
“I’m the mom of a delightful young man with autism, Kyle, age 30, who is severely hypersensitive to fluoride. Sadly, I didn’t know it for the first 14 years of his life and I didn’t even know of the countless other chemical sensitivities. We’ve traveled a very long and painful road together, his pain physical (and profound), my pain emotional.
“His speech is difficult, but he shows me his love and gratitude daily. He trusts me unconditionally because, in his mind, I fixed him. I got rid of the pain for Kyle, yes, but I could never have done it alone. Kyle doesn’t know of the countless FAN workers and advocates who, through their expertise, helped me to figure out how to protect my son. Most of them have never met me, never talked to me, but their work lives through the fantastic FAN website (www.FluorideACTION.net ), newsletters and videos.
“My eyes get wet and blurry just thinking about 1999, when Kyle was 13-14. He was in pain constantly, all over, but especially the back of his neck and his extremities (hands, feet, lips, tongue). The chronic pain had skyrocketed after what I’ll call a “toxicological event” at age 13 from a horrific reaction to a doctor prescribed “over the counter” (OTC) treatment that is completely benign to most people.
“He cried inconsolably when the pain in his fingers got so bad that he couldn’t play his beloved cello in the orchestra at school. He had to quit playing piano, too, and he could barely hold a fork to eat. There were mysterious pain “peaks”, especially in the middle of the night, but other times, too. He screamed and raced around the house as if pursued by killer bees. His school sent him home repeatedly with horrific headaches. At night the house shook wildly with the leg-pounding on the bed that was more like a 4-hour grand mal seizure than “restless leg”. His screaming was deafening. So little sleep….
“We went to 8 medical specialists and not one of them could diagnose the source of the pain, let alone help relieve it. Tylenol guaranteed a full-blown migraine the next day so was useless, as were other pain-relievers. He was completely intolerant of chemicals in the air and his food, so I changed his entire diet to organic, stopped using any cleaners or scented products and got the school to cooperate with a low-chemical environment. He only drank water—nothing else.
“With all of these changes, he improved, but still had pain every day, with screaming, racing, jumping, sweating, heart racing—gasping from the exertion…and crying, begging me to “Make it go away!”
“A mom from Beaverton, OR with two autistic teenagers was the angel we needed. She was the one who first told me in 2000 about toxic fluoride in tap water and instructed me to switch to reverse osmosis filtered water. There was a profound improvement in 3 days! Our lives changed dramatically for the better.
“No, he was not (is not) completely free of all pain—sadly, unexpected chemicals lurk everywhere. But by providing Kyle with fluoride-free water, chronic pain was no longer the 24/7 “norm”, so detecting the other chemical triggers was finally more achievable and allowed much greater success at avoidance. Fluoride remains the worst, and most difficult, to avoid. It took me many years to understand the many sources of fluoride (I will discuss these in part 2 of my letter tomorrow), and to fully realize the extent of Kyle’s sensitivity to it.
“Thank God for FAN’s information that has been there for me time and time again.
“It’s my hope that other children (and teens, and adults), who suffer as Kyle did, perhaps won’t suffer as long as he did. The problem is much greater for those with autism spectrum disorders. Please help FAN inform mothers across the world of the very real harm that fluoride does to some of our most vulnerable people.
“There is so much more to Kyle’s “Fluoride Story”, but you’re busy and I’m out of time. FAN will be sending out part 2 tomorrow. Meanwhile, Please help FAN put a stop to fluoridation with your generous donation. I’ve already sent mine.”
Stuart, I have spent time quizzing this mom. Why is she sure fluoride is one of the chemicals which cause her son pain. She goes into great detail. Better than most doctors do for their patients.
I’ll post the next two parts of her letter later if you are interested.
When we understand that fluoride is an enzymatic reactor, affects the mitochondria, then our concern turns towards how fluoride affects all tissues.
Start asking your patients. Dental fluorosis is a biomarker of excess fluoride. If just a cosmetic problem, no big deal. But fluoride dose not have a direct pipeline to the teeth avoiding all other tissues.
Don’t lie, Bill. You made the allegation/slander about Russian financing and specifically in relation to fluoride. There is no other person here who has suggested such rubbish – only you. And you know that because you don’t name anyone.
The whole thing is insane – even worse than me suggesting that the Russians are supporting the anti-fluoride movement in order to cause dental health problems in the USA. After all, Abby Martin devoted at least one of her RT programmes to presenting the anti-fluoride arguments and the video of that programme is often used by anti-fluoride activists.
No evasion from me – but a lot from you. You withdrew from the first attempt by me to get an exchange with you – specifically asking me not to publish what you had sent. And then refused to follow through in the second attempt.
The only consistent thing with you is the continual lies.
Perhaps you did not read the post. Within the last six months someone else asked you about your affiliation with Russia. You did not answer.
Ken, you said, “Bill, a sensible person is very wary when anti-fluoridationists use the word “Fact.” We know it means a different thing to them.”
Oh, right. You fluoridationists are so honest. Claiming, “Safe and Effective.” Claiming “Fluoridation prevents dental caries.” Two huge whopper lies. Perhaps, maybe with the stretch of hope the word could be “mitigate,” but to claim prevention is a big fat intentional lie to market a toxic substance to everyone without their consent.
If fluoride actually prevented dental caries, we could measure the difference in treatment and costs. Instead, fluoridationists estimate benefits rather than measure.
Just as many dentists per capita in fluoridation communities as non-fluoridation communities. Dentists make just as much money in both places, dental insurance payments are the same.
Ken, trying to take some sort of moral high ground only shows you’re bias. And who is pushing your bias? ADA, NZDA, who? I think you have simply avoided looking at all streams of evidence and enjoy trying to “outsmart” the experts on specific publications.
If you looked at the evidence from all sources and all streams you would not show your bias.
Too many are ingesting too much fluoride and the fluoride does not prevent dental caries and may not provide a life time of dental caries mitigation.
A couple of years ago a commenter on this blog mentioned her sensitivity to CWF, I think in Auckland, and how she resolved the problem by obtaining her water from Tongariro, with no added fluoride.
I suggested that she should get the water she was drinking independently analysed. After all, Tongariro is the one place in New Zealand where the Ministry for Primary Industries advises farmers to be on the watch for fluoride toxicity in their stock…
Reach your own conclusion.
To allow yourself to be influenced by anecdotes is against all the principles of science.
From your anecdotal reply I am able to conclude that, in the more than seven decades of CWF, amongst the hundreds of millions of people who have benefitted from CWF, apart from mild fluorosis, you are unable to point out anybody who science has demonstrated injury from CWF.
Bill, it is hypocritical for a person resorting to McCarthyist attacks to defend their anti-science position to then talk about the moral high ground. You are an incorrigible lier – morals simply don’t come into it for you.
Bill, you disqualified yourself from a scientific exchange with me. To sink so low as telling outright lies about my offer of a scientific exchange – to blame me for your inability to follow through – is despicable.
To make the McCarthyist smear – money from Russia for me – as a diversion from a proper scientific discussion is even worse.
The article for these comments is on scientific integrity and fluoridation and specifically about the way Dr Ghali attempts to prevent proper scientific peer review. That is a serious subject yet you have refused to contribute to it – you have attempted to hijack the discussion into an irrelevant direction and a cynical diversion. I refuse to divet and that makes you upset.
My advice to you, Bill, is to discuss the article, not attempt these dishonest diversions. There is no value in my allowing a commenter to continually attempt to undermine a proper scientific discussion in this way.
I grew up without fluoridation, but regular dental workups. Result was at least twenty fillings by the age of twenty.
My children grew up with CWF as well as regular dental workups. Result by the age of twenty was four fillings between them. Combined total of fillings less than a fifth of mine. That’s probably a benefit of CWF.
The genetics are (obviously) similar. Toothpastes, upbringing, education to professional level, food, (lack of) sugar ingestion, are all similar, so it’s highly likely that the presence of CWF had some influence on that outcome.
As for the actual science of benefits from CWF – haven’t you been reading this blog? Or read your dental textbooks? I’d just be repeating many papers that have been discussed here previously. Many population studies show benefits from CWF across entire populations. None have shown injury from CWF apart from mild fluorosis. And that science has been derived by collectively following hundreds of millions of people over more than seven decades.
By the way, pointing out that you appear to be allowing yourself to be influenced by anecdote rather than following the science, especially on a science based blog, is hardly jumping your bones. It’s just part of the scientific method and you can expect it if you don’t follow the science.
You say, “highly likely that the presence of CWF had some influence on that outcome.”
Anecdotal faith is not science. Highly likely for two children is not strong evidence.
For the past 90 years each generation has had fewer cavities than the previous, as a whole. (About level for the last decade.) You have no more factual data for benefit of CWF than proof of flying rain deer.
Your evidence is no stronger or weaker than the harm for Kyle from CWF. However, Kyle’s reaction is rapid and consistent. When he has a bath or shower with CWF, he has severe pain for several hours. You really don’t know if your children on a daily basis have fewer cavities.
Did your parents have you clean your teeth and visit the dentist as often as you have for your children? Did the schools teach the same? Many causes of caries and in Kyle’s case, pain. However, cause and effect is easier to monitor and evaluate than caries which takes many months/years.
However, two kids with fewer cavities than parents and grandparents is great news. If CWF actually helped, too bad so many were harmed with excess fluoride.
And you could have given your children fluoride from other sources but avoiding fluoride is much more difficult.
Read my comment. I said I was replying to your anecdote with an anecdote.
Your request for scientific evidence of benefits of CWF was also answered – you can find the evidence in many of the posts and comments on this blog, and even in the textbooks that are required reading to gain a dental qualification.
That evidence was also in the required textbooks on public health when I obtained my own medical qualifications, and still is. I don’t need to waste bandwidth, or time, repeating publically available knowledge.
Despite population scientists following hundreds of millions of people for more than seven decades, there is still no evidence of harm from CWF other than mild fluorosis.
Yes, anecdote for anecdote. However, you ripped me apart for providing what you asked for.
And although each are individual cases, you cannot be as confident fluoride prevented caries because caries takes a long time to develop.
Whereas, an adverse reaction within a few minutes/hours and diagnosis of fluoride sensitivity by the patient’s doctor provides far greater confidence. The fluoride can be tried to see if the patient has an adverse response and avoided to see if not.
Kyle is very autistic and has no clue whether his mom is using fluoridated water or not. He does know when he gets pain.
You don’t want to waste time providing the science on benefit. Really? Is that because the science is incomplete and low to moderate quality?
No. . . you simply do not have the evidence of efficacy.
You say there is no harm from CWF. Perhaps you should look at the science of harm. Many, many studies.
It is true (fact) that since CWF started, dental caries have declined from about 5.5 cavities to about 2.2 cavities.for 12 year olds. At first glance, many give CWF the credit.
However, during the 4 decades prior to CWF starting, cavities fell from about 11.5 to 5.5, an even greater decline..
The critical question is, “what cause caries to decline prior to CWF?”
Seriously, Stuart, there were/are huge monster crushing caries unknowns which caused the decline. They did not stop caries reduction just because CWF started.
Fluoridationists give CWF credit for caries decline, but their research never includes the unknowns.
Just because two events happen does not mean they are related.
Too many are ingesting too much fluoride and the fluoride has risks and expenses with questionable benefit.
Have you noticed Ken does not discuss benefit or dosage of fluoride exposure? The science on benefit and dosage is more incomplete than risk..
Just offhand, I can think of several possible causes of Kyle’s discomfort. He may not have been told whether water is fluoridated or not, but his parents are aware of the situation, and as an intelligent human being Kyle can pick up on his parent’s or caregiver’s expectations, just as much less intelligent non-human animals can pick up on their owner’s expectations. He actually does “have a clue” – or possibly a cue – just as non-human animals do.
And that’s the last I’ll discuss your anecdote. As you said: “just because two events happen does not mean they are related.”
“What cause (sic) caries to decline prior to CWF?” I’ll take a guess. Development and mass marketing of conveniently available toothbrushes and toothpaste/tooth powders?
Hundreds of millions of people have benefitted from CWF for over seven decades. The outcome of this has been followed by population scientists for all of that time. The data is publically available, particularly through the NHS in the UK, concerning health outcomes of matched fluoridated and non-fluoridated populations.
Rather than speculating that CWF may, or may not, cause adverse outcomes, why not look through those seven decades of data, amongst those millions of people, and see if CWF has actually caused adverse outcomes?
Bill, put aside your personal hatred for me – it interferes with your ability to discuss issues. It is very noticeable that you always attempt to divert discussion away from the articles you comment under – in this case, the issue of Dr Ghali’s attempt to close down scientific peer-review and the issue of scientific integrity).
But it is good to hear you say:
“Just because two events happen does not mean they are related.”
Correlation is never evidence for causation – but again and again, anti-fluoridationists act as if it were. Their whole reliance on the IQ issue at the moment (you seem not to have got the message from FAN headquarters of the change in tactics – hell that message couldn’t be made clearer) relies completely on using extremely weak correlations to argue causation. Without proper consideration of confounding factors or investigation of mechanisms
But you are completely wrong to say:
“Fluoridationists give CWF credit for caries decline, but their research never includes the unknowns.”
Other possible risk-modifying factors (or unknowns) are regularly included in investigating relationships with CWF – and some important effects have been demonstrated this way.
But the evidence for the efficacy of CWF rests on multiple sources, including investigation of mechanisms, surface reactions, etc., as well as basic chemistry.
The different approach of the anti-fluoridationists, the straw-clutching using weak relationships and reliance on correlations without other mechanistic support, is simply a result of the ideological and financial motivations of this group. The recent exposure of the role of Merocla in funding FAN and anti-vaccination groups is clear evidecne for that unscientific, ideological driving force (see Major funder of the anti-vaccine movement has made millions selling natural health products).
A huge problem with anecdotal “evidence’; of the sort almost exclusively used by anti-fluoridationists is that it ignores the psychological factors which are often the real causes. In the case of fluoridation this was shown by a Finnish experiment some time ago – see Fluoride sensitivity – all in the mind?)
You said, “Hundreds of millions of people have benefitted from CWF for over seven decades.”
Benefit of CWF is an assumption. I have looked at the science, many studies and reviews of the studies. None of the studies rise to the level acceptable to the US FDA, or I bet for Ken, you or me. Yet the assumption of benefit continues.
Thanks for speculating on the cause of caries decline prior to CWF. I too thought it might be toothpaste. However, fluoridated tooth paste was introduced after CWF, so that is not the reason for the huge decline prior to CWF.
Could it be tooth brushes? Maybe. If so, did the tooth brushing benefit max out right as CWF start? Not likely. Others have speculated increased shipping of fresh produce year round. Again, did the fresh produce max out just as CWF started?
No one knows and that huge confounding factor has not been included, factored in, or controlled, in any caries research.
2. I have repeatedly said raw data from research must be open for all to evaluate. That includes the CDC and HHS. They have pictures of the fluorosis in their survey’s and will not release the photos. Only one reason I can think of. The huge decline in dental fluorosis after 2012 is not physiologically plausible. The diagnosis changed or the data has been cooked. And they have not withdrawn their data or explained or provided the pictures.
3. You disagree that studies have not included confounding factors.
All CWF studies omit one or several of the following:
A. Not one Study corrects for Unknown Confounding Factors (such as the cause for decline prior to CWF)
B. Not one Prospective Randomized Controlled Trial
C. Socioeconomic status usually not controlled
D. Inadequate size
E. Difficulty in diagnosing decay
F. Delay in tooth eruption not controlled
G. Diet: Vitamin D, calcium, strontium, sugar, fresh and frozen year round vegetables and fruit consumption not controlled.
H. Total exposure of Fluoride not determined
I. Oral hygiene not determined
J. Not evaluating Life time benefit
K. Estimating or assuming subject actually drinks the water.
L. Dental treatment expenses not considered
M. Mother’s F exposure, Breast feeding and infant formula excluded
N. Fraud, gross errors, and bias not corrected.
O. Genetics not considered
Ken, you are very demanding of research showing harm, now be consistent and demand the same quality for benefit. In fact, the research on benefit must be strong before CWF is started.
I agree that anecdotal evidence is problematic.
And even a placebo has significant claims of benefit.
What we look for is a significant increase of benefit from a medication greater than the placebo control.
The mind does powerful tricks. And that is a prime reason we need RCT studies for CWF.
The half life of fluoride in humans is about 20 years. A one month study will do little more than consider acute symptoms which may not have been measured adequately.
Increases in fractured teeth or bones, thyroid disorders, cancer, lower IQ, and a host of other symptoms will not show up in one month and not considered.
Ken, use the same critical thinking on dosage and benefit as you do for harm.
I never thought I’d have to be telling a dentist this. Toothpastes and tooth powders have been around for ages. The Romans and Greeks both had tooth powders. Toothpastes are noted in Victorian literature and their containers are found in museums. Tooth brushes have been around almost as long, but were originally made from wood/bone and animal bristle. Their handles can also be found in museums.
If you read my comment accurately, my guess was about mass marketing. Mass marketing of toothbrushes occurred after the development of plastics, and hence the mass market for toothpastes and powders increased at the same time.
If you demonstrably cannot read a brief comment on a blog accurately, how certain are you that you have correctly read the scientific consensus found in dental textbooks? The science that shows the efficacy and safety of CWF as demonstrated in millions of people worldwide over more than seven decades?
My point exactly. I agree with your comment about oral hygiene.
Tooth brushes and tooth powders were used long before the 1920’s. Could the mass marketing cause/contribute to an increase in usage of these and a decline in caries? Yes, indeed, they could be a major cause. We don’t know for sure.
However, Stuart, makes sense to consider tooth brushes and tooth powders caused a huge decline in the 3 to 4 decades prior to CWF. Could also have been increased transportation of fresh produce all year round. Or several other possibilities.
But one thing we know for sure. . . FACT. . . UNDISPUTED FACT. . . A NO BRAINER. . . . CWF did not cause the decline in dental caries prior to CWF starting. That’s my point Stuart. Huge factors more powerful than CWF are unknowns and never controlled for in research of CWF.
AND, If the decline was the tooth brush and powder/paste prior to CWF, did their benefit stop as soon as CWF started? Not likely. Yet you give credit to CWF when the decline after CWF started could still be what was causing the decline before CWF started. My point is, there are huge unknowns not controlled for with CWF research.
Remember, 50% of scientific consensus is wrong, it is our job to correct the wrong.
At one time the consensus was to treat dental caries with mercury fillings.
At one time the consensus was that root canals were 95% successful.
At one time centric relation explained how the mouth opened and closed (function, ROM, etc.)
Etc. Etc. Etc.
Science is not stagnant and is dynamic with discovery and corrections and improvements.
On another note, the FDA has approved fluoride toothpaste because the research is adequate. Fluoride works topically, not systemically.
Bill – McCarthyism is pure hatred and these days it does not have an ideological or political excuse – it is based on racism.
As foir research – I am demanding of all research. That derives from a lifetime of science publication and peer-review.
The example of Malin & Till (2015) is instructive. You would prefer I did not expose the flaws in this study and indeed Till still acts as if Perrott (2018) was never published. But that is how science works – most ideas in science are wrong and that is why critical and intelligent analysis of studies are required. That is how science makes progress and removes old and mistaken ideas.
You say McCarthyism is pure hatred. I would define it as a hatred for Communism, or a campaign or practice that endorses the use of unfair allegations and investigations.
I disagree with Communism but don’t hate it. Are you referring to unfair allegations and investigations? Not sure your intent when you call it based on racism.
None of that has to do with science, so I’m not following you.
I don’t think CWF has anything to do with racism.
However, I’m 100% with you when you say, “most ideas in science are wrong and that is why critical and intelligent analysis of studies are required. That is how science makes progress and removes old and mistaken ideas.”
Therefore, if you thrust is towards unfair investigations of the science of CWF and fluoride exposure, then I agree.
You want to get into the details of specific studies of risk. Fine, we should. However, we first need to consider dosage, or we risk serious bias.
For example, hypothetical. Suppose you looked at the science of fluoride’s benefit and found benefit highly unlikely. And suppose you looked at dosage and realized many are ingesting too much fluoride from many sources. In other words, does little or no good and we are getting too much.
If we think fluoride ingestion has great benefit, then our bias permits some risk.
If we think fluoride ingestion has no/little benefit, then our bias becomes alarmed with any hint of risk.
Therefore, any discussion of risk needs to first start with dosage and benefit.
All drug regulatory agencies require that approach. First, show the research on benefit at a specific dosage. Once benefit has been established at a specific dosage, risk can be evaluated at that dosage.
Ken, unfair investigations of fluoride fail to consider dosage first. An assumption of great benefit results in a bias dismissing risk.
Bill if you don’t think CWF has anything to do with racism why adopt a racist McCarthyyist attitude towards a scientist just because he is discussing the science? The fact is that racism, McCarthyism or accusations of “Russian” payments have absolutely no place in a discussion on this subject and the fact you adopted that approach disqualifies you from any rational discussion of the issue here.
Especially as there has not been any apology for that McCarthyist attack on me if for your lies about the proposed scientific exchange with me.
No apology at all – just more lies.
As for discussing the proven wrong ideas, or suspect ideas, in science – you are the one refusing to discuss the content of this article here – the question of integrity in science and Dr Ghalis attempt to stop peer review of the Green paper. You are doing that by attempting diversion onto irrelevant issues and by hateful attacks on me.
After all the attacks you have done and do to me, looks like you have a very thin soft skin. You persist in calling me a liar and no apology from you.
I’m sorry. Now, would you please stop the attacks on me and go to the science . . . as I have repeatedly requested.
For the fourth or fifth time, I agree with you 100% that science should be open. I have given you at least one example. However, the Green paper went through two peer reviews, as I remember. Does not need another peer review, but I do not know why the data should not be open.
However, your bias and lack of willingness to start at the foundation and look at dosage, makes me doubt your judgment.
You are only looking at one side of the equation or puzzle. Start by backing up and looking at the most basics, i.e. dosage, and then move to the review of risk.
Dosage is where all good scientists reviewing the benefit of a substance start.
We all must start at dosage. Too many are ingesting too much fluoride.
Bill, you are a liar – you lied about the proposed exchange on my blog claiming I had stopped it when it was you that refused to follow through.
that is a despicable lie – nothing to do with my skin – simply an indication you are incapable of a good faith scientific exchange to the extent you will use your laziness to manufacture a lie about me.
Until you ap[oligise for the lie and for the implication I am being paid by “Russia” there is absolutely no hope of a discussion of scientific issue with you here.
Please do not pretend to attempt a discussion of the science – you had your chance and you refused to follow through. You are simply attempting to divert from the content of this article and from the disgusting behaviour attacking me.
Scientific consensus is that CWF is safe and contributes to improved dental health. That has been shown in hundreds of millions of people over more than seventy years. The research is demonstrated in your dental textbooks, in public health textbooks, by Cochrane, and in the many more recent papers cited on this blog.
Against this is your speculation, or belief, voiced amongst that of other anti-fluoridationists. Ken has repeatedly demonstrated that evidence in support of your speculation is lacking.
To support your speculation with evidence, all you need to do is to demonstrate, amongst the well documented data of those hundreds of millions of people, for over those seventy plus years, that CWF does not benefit dental health and/or injures health in other ways.
If your speculation is accurate then the existing data in populations with and without CWF will provide the supporting evidence. There’s no need for you to speculate, if your belief is accurate then the evidence is already in the data.









Ghali still refuses to view the science critically, instead naively continuing to take the studies at face value while implying that those who do critically evaluate them are simply attacking the studies out of biased advocacy. At some point he needs to wake up and understand his own limitations and failures with the O’Brien report. He needs to correct the misconceptions he has irresponsibly disseminated with that report and his subsequent dogged defense of it in the face of legitimate questions put forth by respected reviewers.
There is enough misinformation constantly put forth by antifluoridationists and their little groups, without Ghali adding to it.
Steven D. Slott, DDS
LikeLike
Ken,
Integrity? Define: “The quality of being honest and having strong moral principles”
Keep in mind that every individual, fetus, infant, child, adolescent, teen, young, old, healthy, edentulous, dentate, chemically sensitive, are all being supplemented additional fluoride without their consent, without doctor’s prescription, with an unapproved drug, regardless that over half show signs of a toxic overdose of fluoride AND those who want to ingest fluoride can easily get it cheaper and by choice. And you call that public health policy “honest and having strong moral principles.” Don’t feed me your “integrity crap” while removing freedom of choice from millions. You can’t steel the moral high ground with ignorance.
While you keep in mind that too many are ingesting too much fluoride, let me quote Dr. Gahli:
“The new cognition studies (led, interestingly, by two Canadian public health research teams) and the ensuing NTP draft report from the US are now such that it would have been absurd for us to pretend that the new studies do not even exist or that they are fatally flawed with irrelevant results.”
And I would add, the USPHS recommended lowering fluoride concentration in water. . . why? Clearly, too many are ingesting too much fluoride.
And the NRC 2006 report advised the EPA to lower their MCLG which for 13 years the EPA has ignored.
And the EPA DRA, RSC clearly showed even if EPA standard for safety were to permit even more fluoride by 33%, still most of the young would exceed safety exposure levels.
Be careful Ken when you try to take the “moral, ethical integrity” high ground supplementing everyone with even more fluoride without their consent.
Ken, your fatal flaw is you refuse to include dosage in your narrow focus.
Studies of risk will always be weaker because highest quality studies to discover/prove harm are unethical. A different set of assessment skills are necessary. We must not be barbaric and do research like Hitler did.
Ken, I don’t think you appreciate or understand dosage, NOEL or LOEL.
TConsider, the difference between hazard and risk is dosage.
Quoting Stahlmann:
“This article starts with a few comments on the identification and assessment of toxicological risk to show why so many public debates lack the necessary risk competence. . .
“The main focus of pharmacology and toxicology is the desired and undesired or adverse effects of chemical substances on living organisms. One important task in this field is the identification of the basic mechanisms of action that means, the interaction between the chemical substance and the biological structures relevant for the effect at the molecular level. Understanding the toxicological effects of substances thus requires sound knowledge of physiology and biochemistry to answer the question about the mode of action of a poison or drug. . .
“The terms ‘hazard’ and ‘risk’ relate to completely different circumstances. Hazard, which should be understood in a qualitative sense, can be used for substances with a toxic potential. In contrast, risk should be understood in a quantitative sense because this term describes the incidence of an adverse effect at a certain level of exposure, hence a definable quantity. This definition is based on human data; thus, it retrospectively refers to a situation in which the damage to people has already occured. Prevention is not possible this way.
“In toxicology, two different approaches have to be distinguished: medical risk assessment and preventive risk minimisation. Both approaches ultimately help to reduce or prevent risk to human health. In risk assessment, dose-effect-relationships and definite incidence rates may be stated. In prevention, certain thresholds are estimated below which health risks can be excluded or considered ‘acceptable’. Prevention calculations are mostly based on experimental animal data and extrapolated to humans; thus, such calculations often include (un)certainty factors which are based on more or less secured assumptions. …
“Dose-effect-relationships in the low-dose range cannot be distinguished in experiments. For instance, determining an effect incidence of 1/100 or 1/1,000 with the required safety margin would require the examination of an unjustifiably high number of animals. Serious toxic effects affecting one in a hundred or one in a thousand people are not acceptable in most circumstances. For this reason, comparatively high doses are used in animal experiments, and the results have to be extrapolated from high to low exposure and from one species to another. The higher the gap between the experimentally investigated doses and the exposures to be reviewed, the higher is the uncertainty in extrapolation. It should be taken into consideration that high doses are often marked by several – and often interacting – effects, resulting in complex dose-effect-relationships. Because the course of a dose-effect-relationship curve in the low-dose range is unknown, a no observed adverse effect level (NOAEL) is initially determined, hence a dose for which no toxic effect can be found in the experiments. A safe range of exposure (for instance, acceptable daily intake – ADI) is then defined by means of an (un)safety factor. The applied factors are usually round numbers, such as 100, 300 or 1,000, which shows that these factors are not based on science but serve an administrative and political purpose. In the context of health politics, this concept appears rather appropriate because of often missing data on the mode of action of a substance and other knowledge gaps.
“Thresholds defined by different institutions or the legislature have both a regulating and a communicative function to prevent health risks and damage to the ecosystem. Risk analyses are mainly based on toxicological and epidemiological data. Four different phases have to be differentiated: Identification of potential hazard, analysis of the dose-effect relationship, analysis of the exposure and identification of populations at risk (Table 2 (Tab. 2)). Because of the general dose dependency of effects due to xenobiotics, thresholds have to be established for each substance, by which exposure irrelevant to health can be distinguished from exposure relevant to health. Thresholds in the low exposure range are often scientifically disputed. This range is marked by speculations because meaningful prospective studies, such as in drug development, are ethically not justifiable in most cases. However, retrospectively collected data often contain confounding elements, and the significance of such data is often somewhat overrated. Relative risks found in such studies have to be differentiated from risks found in the context of risk assessments that constitute incidences. A relative risk is the ratio of an exposed group and a control group.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4507061/
Ken, it is frustrating discussing anything with you when you refuse to include the basics of pharmacology and toxicology, i.e. dosage.
Everything is poison, the dosage makes the poison.
We have uncertainty factors in toxicology which must be included with judgment.
Too many are ingesting too much fluoride.
Bill Osmunson DDS MPH
LikeLike
Bill where is the integrity in Dr Ghali characterising my position as asking him “to pretend that the new studies do not even exist or that they are fatally flawed with irrelevant results.”
Of course that absurd and it is absurd of you to endorse his silly comment.
LikeLike
Bill, in spite of having had the nonsensical nature of your stale claims explained to you repeatedly, you continue to make them. Develop some integrity, man.
Steven D. Slott, DDS
LikeLike
Ken and Steve,
You make ad hominems and make personal attacks rather than attacking the facts. If you had the facts, you would present them.
Too many are ingesting too much fluoride. That is an undisputed fact which both of you would like to ignore, and the foundation for any discussion on fluoride. Any freshman student evaluating substances for benefit and risks, understands the essential foundation of dosage.
Steve, you say my “claims” are nonsensical. Well then, Ken and Steve, I’m listening, show your evidence. Show your facts. What evidence do you have that many are not ingesting too much fluoride? What about the question does not make sense to you?
Dosage. Too many are ingesting too much fluoride and that is undisputed and makes scientific sense. What about that question does not make sense to you?
Ken, I think you would agree there are different levels of confidence with different kinds of studies. For example, prospective studies are better than retrospective studies.
I presume you would agree human studies are better than animal studies (for human evidence.)
I presume you would agree RCT studies are better than ecological studies.
Please provide your RCT prospective human studies on efficacy of fluoride exposure for the mitigation of dental caries and please provide them for safety. There are none. No high quality studies and yet you persist in claiming efficacy at an unknown total fluoride exposure and safety at an unknown dosage is safe and effective. That makes no scientific sense.
Supplementation without consent in the USA of fluoride has been a public health policy for over 70 years with claims of efficacy and safety and yet the high quality studies are still lacking. Fluoridation has been an unapproved experiment without scientific evidence.
Understanding fluoride’s developmental neurotoxicity in the 2006 NRC report was only explored and postulated, they had little evidence. In the last 13 years we have many human and animal studies raising concern with over 80% consistently reporting harm. The quality of the studies are getting better and more consistent. What are the chances of new studies refuting the many studies reporting harm? Not great. Some have, but most raise serious concern. The trend is clear, fluoride is presumed a develoopmental neurotoxic substance according to the NTP.
Ken and Steve, you approach the subject from the position that consumers/patients/public must provide absolute proof of harm. That’s ass backwards.
The FDA is clear, it is the manufacturer who markets the product that must provide the proof of efficacy and safety at a recommended dosage.
Start looking for proof of safety rather than proof of harm, for each of the concerns listed in the NRC 2006 report.
LikeLike
Bill, you’re as predictable as the sun rising and setting each day. Always whining about non-existent “ad-hominems” against poor little you, in transparent attempts to make yourself out as some sort of victim whenever your nonsense is exposed for what it is. Perhaps that worked for you with your parents when growing up, but is unbecoming for adults. Stating obvious facts does not constitute “ad-hominem attacks”. If you wish to be treated as an adult, then act like one.
1. Because you make some unsubstantiated claim about people “ingesting too much fluoride” does not make this an “undisputed fact”. It makes it a
Bill Osmunson personal opinion.
2. Yes, dose and concentration are basic elements in discussing risk and benefit of substances. Unfortunately, you and Connett have never seemed to understand the difference between the two concepts or how they relate to fluoridation.
3. It is neither my, nor anyone else’s, responsibility to disprove your unsubstantiated claim that “many are ingesting too much fluoride”. It is your responsibility to back up such claims with facts and evidence….which you obviously cannot do. That said, the fact that your claims are nonsensical was in regard to the stale, meritless arguments of “consent, doctor’s prescription, unapproved drug, toxic, choice” etc, etc…..none of which have any relevance to fluoridation, all of which are constantly thrown out by antifluoridationists seeking to muddy the water with ridiculous nonsense in lieu of facts and evidence.
4. I do not agree that RCTs are better than observational ones in regard to assessing the effectiveness of a broad public health initiative such as water fluoridation. Just the opposite. RCTs are far too narrow and focused on the individual to make any such assessment. I will gladly, as I have on numerous occasions, provide you with a multitude of high quality observational studies clearly demonstrating the effectiveness of fluoridation in the prevention of significant amounts of very serious dental infection in entire populations.
It is very telling that you defend the agenda-driven Till, et al assembly line of antifluoridation studies, none of which are RCTs. Seems your faulty reliance on RCTs is highly selective.
5. Given the 75 year history of fluoridation, hundreds of millions having chronically ingested optimally fluoridated water during this time, with no proven adverse effects on anyone….given that there is no valid evidence that fluoridation is, in any manner, unsafe…… it is neither my, nor anyone else’s, responsibility to disprove unsubstantiated claims by antifluoridationists that the initiative is unsafe.
6. There is no “unknown dosage” involved with fluoridation. For every one liter of optimally fluoridated water consumed a dose of 0.7 mg fluoride is ingested. Ironically, it is the non-optimally fluoridated water for which you advocate in which the dose is unknown. In the US, this dose can legally be as high as 4.0 mg per every one liter of water consumed…..nearly 6 times the level allowed in optimally fluoridated water.
7. Your personal definition as to what makes “scientific sense” needs a lot of work.
8. The 2006 NRC did not list neurotoxicity as a concern in its final recommendations regarding water with a fluoride concentration of 4.0 mg/liter and below. If it had deemed this to be of concern at this level the committee would have been responsible for so noting and recommending accordingly. It did not.
9. Your uncited “many human and animal studies raising concern” are presumably those presented in the meritless fan petition to the EPA. Citing facts and evidence, EPA reviewers explained the invalidity, irrelevance, and misrepresentation by petitioners of those studies. If you haven’t read that rejection document you should do so.
10. The NTP has not presumed fluoride to be neurotoxic. That which you misrepresent is simply a non-reviewed draft put out for public comment. It does not represent any official NTP determination or policy.
“This DRAFT Monograph is distributed solely for the purpose of pre-dissemination peer review under the applicable information quality guidelines. It has not been formally disseminated by NTP. It does not represent and should not be construed to represent any NTP determination or policy.”
11. Given the 75 year safety record of fluoridation and the void of any valid evidence of “harm” it is indeed the responsibility of those such
as you who wish to discontinue this initiative to provide valid evidence to support your claims, not the other way around
12. The FDA has no jurisdiction over fluoride in drinking water. How it regulates the retail products under its jurisdiction is of no relevance to water fluoridation.
13. For the past 75 years, antifluoridationists have turned over every possible rock they could to find some kind of “harm” they could attach to optimally fluoridated water. They have had zero success.
Steven D. Slott, DDS
LikeLike
Thank you Steve for a thoughtful response. I hope my response will stimulate some thoughts. I wish Ken could pull himself together and follow your example.
Each of your items should take many back and forth for clarity and understanding. I am torn between working on one item or doing more. Fluoridation is a huge subject with many streams of evidence.
Item #1. Too much fluoride. Yes, my opinion based on fact. For a start,
a. Do you dispute Millions have dental fluorosis? A biomarker of fluoride exposure.
b. Do you dispute the EPA’s Dose Response Analysis and Relative Dose Contribution of 2010 reporting at least a third or a half of our young are ingesting more fluoride than their suggested “safe” dosage?
c. Do you dispute the HHS lowered the concentration of fluoride in water? Was that enough and has it reduced dental fluorosis rates?
d. Do you dispute that mother’s milk contains much much less fluoride than fluoridated water? An infant on formula made with fluoridated water would far exceed the dosage of fluoride in mother’s milk.
If so, provide your evidence and reasoning.
Item #2. I and Connett keep pounding on those promoting fluoridation, that concentration is not dose. You say we don’t understand, then explain. I’m listening.
You add, “or how they (concentration and dose) relates to fluoridation. My exact thoughts about fluoridationists. The concentration of fluoride in water is not dosage of fluoride from water or total fluoride exposure. So please explain your thoughts.
I had to jump all over a Harvard Professor because he tried to confuse the audience claiming concentration of fluoride in water was a human dose. So it is with pleasure, I can agree with you that dose and concentration are not the same.
Simply put, water fluoridation is not a dose, it is a concentration. The dose would depend on how much water the person drinks. Some non-fluoridated and some (according the the NRC 2006) over 10 liters/day.
Would you agree that fluoridated water is not a controlled individual dose, rather it is a concentration?
Would you agree that water fluoridation represents only about one or two thirds of total exposure?
Item #3. I think we disagree on jurisdiction. I am confident no law or court or agency charged with oversight of any substance used with the intent to prevent disease requires the consumer, user, purchaser, patient to prove with scientific studies, efficacy, dosage and safety.
The FD&C Act places such responsibility on the marketer of the product to achieve FDA approval. Do you disagree?
Item #4. I would question your suggestion that observational studies are better than RCT in public health. Faster, yes. Cheaper, yes. I would suggest both are important but RCT have lower risk of bias. RCT are gold standard for research. Too often observational studies confirm bias or we miss confounders and unknowns.
A couple examples of my concern. The caries rates for 12 year olds in 1921 was about 11.5 per child. When fluoridation started with significance, the dental caries rates had dropped for 12 years old to about 5. A clear observation of prevalence and a significant decrease. However, I have not heard anyone explain what caused the decrease. Clearly, some major confounding factor(s) reduced dental caries. Let’s call it unknown “X”.
Would you agree, the chance that unknown “X” stopped exactly when fluoridation started is beyond reason?
Would you agree that any observational study would not control for unknown “X” and probably would control for in a prospective randomized controlled blinded trial?
There are several factors affecting dental caries, not just fluoride and the unknown “X” is just one problem with observational studies.
Most/many observational fluoridation studies do not include:
Socioeconomic status
adequate size
Difficulty and consistancy in diagnosing decay (today is much different than when I was in school)
Delay in tooth eruption
Diet: Vitamin D, calcium, strontium, sugar, fresh and frozen year round vegetables and fruit consumption not controlled.
Total exposure of Fluoride not determined
Oral hygiene not determined
Not evaluating Life time benefit
Estimating or assuming subject actually drinks the water.
Dental treatment expenses not considered
Mother’s F exposure, Breast feeding and infant formula excluded
Fraud, gross errors, and bias not corrected.
Genetics not considered and maybe a huge factor.
My one office observational opinion was very positive. I was convinced fluoride reduced dental caries. My bias was strong. Careful evaluation of the studies showed me where I was observationally wrong. A real kick in the gut.
I will admit my public health education was long time ago, but no professor suggested observational studies were stronger than RCT.
The second example of my concern over observational studies would be blood letting. The practice persisted because benefit was observed. And I will concede that too often RCT studies are later show to be false.
I think both are important and I defer to the FDA which requires RCT studies to increase their confidence for approval.
Perhaps I have gone on long enough and should address your other points in another post. Intellectual gymnastics is not my sport.
LikeLike
Bill:
1. You concede that your claim was nothing but personal opinion, not “undisputed fact” as you falsely stated.
2. Yes, millions have dental fluorosis, the overwhelming percentage being mild to very mild, a barely detectable effect which causes no adversity on cosmetics, form, function, or health of teeth. While this is a biomarker of exposure to fluoride, it is not an indicator of overexposure. Peer-reviewed science has clearly demonstrated mildly fluorosed teeth to have increased decay resistance, with there being no valid, peer-reviewed scientific evidence of any adverse health effects from this effect.
—-The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren
Hiroko Iida and Jayanth V. Kumar
J Am Dent Assoc 2009;140;855-862
3. The EPA does not have “a safe dosage” of fluoride. This is a clear example of your lack of understanding of dose vs. concentration. The EPA has set a maximum allowable concentration of 4.0 mg/liter fluoride in water, not a dose.
4. The HHS did not lower the concentration of fluoride in water. HHS has no authority, or ability to do so.
5. By “mothers milk” it is assumed you mean human breast milk, the contents of which have no relevance to water fluoridation. Given that this milk is deficient in iron, vitamin K, and vitamin D to the point of requiring supplements of these substances for breast-fed infants, basing infant dietary needs on such content would mean that infants are meant to be anemic free-bleeders who develop rickets.
6. Your confusion of dose and concentration is clearly evident in my item #3 above.
7. Yes, the concentration of fluoride in water is not dosage of fluoride from water or total fluoride exposure. This elementary concept is self explanatory and requires nothing further in regard to my “thoughts”.
8. Yes, dose and concentration are not the same. Congratulations, you finally seem to be gaining some understanding of this.
9. Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans. The same is true of chlorine, ammonia, and the myriad other substances routinely added to public water supplies.
10. According to the CDC, of the total daily fluoride intake, 75% is from water and other beverages.
11. It is of no consequence whether you disagree with the facts or not. The contents of drinking water supplies are under the jurisdiction of the US EPA, not the FDA.
12. The effectiveness of population-based public health initiatives is not limited to individual effects. It is a measure of the total impact on the entire group. While fluoride does reduce significant amounts of dental decay, other factors may include greater dental awareness within the group due to knowledge of the initiative being in effect, resulting in improved home oral healthcare, more consistent visits to dental providers, dietary improvements, etc. The impact of all of these factors combined are best evaluated by observational studies of the whole population, not by RCTs. In addition, results of RCTs have been shown to have no greater quality than those from high quality observational studies.
“CONCLUSIONS
We found little evidence that estimates of treatment effects in observational studies reported after 1984 are either consistently larger than or qualitatively different from those obtained in randomized, controlled trials.”
—A Comparison of Observational Studies and Randomized, Controlled Trials
Kjell Benson, B.A., and Arthur J. Hartz, M.D., Ph.D.
June 22, 2000
N Engl J Med 2000; 342:1878-1886
DOI: 10.1056/NEJM200006223422506
13. If some “unknown X” is a problem with fluoridation effectiveness studies, it is much moreso with the poor quality observational IQ studies antifluoridationists so ardently defend. Given the highly complex factors involved in human cognitive development, the chance of unknown factors skewing results is far greater in those studies than in effectiveness studies. Again, your reliance on RCTs is highly selective, driven by your own confirmation bias.
Steven D. Slott, DDS
LikeLike
Steve,
That’s not what I said. . . .
I said, “my opinion based on fact.” You responded, “You concede that your claim was nothing but personal opinion, not “undisputed fact” as you falsely stated.” Please read what I say and don’t distort or twist.
Everyone has their opinion which is not always based on fact. And each person puts different weight on different facts.
And second, I don’t know of any science which is not disputed, especially fluoride.
Read what I write and try to understand. I don’t intend to argue.
We agree, dental fluorosis is a biomarker of fluoride intake. The dispute is whether the a biomarker of intake represents an excess of the substance. We agree most have mild/moderate. We agree cosmetic. But a higher intake than if they had no DF.
Historically when fluoridation was started, the public was assured fluoridation would only result in 10% or perhaps 15% DF prevalence. We are now at 40% to 60% depending on the survey and NHANES reports 20% moderate/severe. If 1% have severe DF of the more than 200,000,000 on fluoridation, that means over 2,000,000 have ingested too much fluoride. Would you agree?
Dentists have tried to minimize DF as only a potential “cosmetic” effect. . . as though fluoride only goes to the teeth and not to every cell in the body. We dentists and public health experts have not done safety studies to determine safety, We are marketing blind to our risks. For years we had neither observational or RCT studies on any risks.
However, I would maintain that even mild DF is an indication of possible excess fluoride for soft tissues, especially the developing fetus.
I do not dispute that studies exist which claim those with some DF have fewer caries and those with none or severe DF have more caries. Although the difference is minimal, there is a “sweet” spot of dosage which is probably beneficial in reducing dental caries. Not much reduction, maybe not any reduction, but probably some reduction.
In my presentations I show a graph of the data from Iida, Kumar publication which you reference above. The factual data indeed shows a slight reduction of caries but very hard to detect. And the effect could be one of several research limitations. For factual example, life time benefit is not considered.
#3. I agree EPA has 4 ppm MCLG. However, if you read the EPA’s 2010 Relative Source Contribution and Dose Response Analysis, you will understand a great deal more about EPA and “safe” fluoride exposure. See the DRA report for non cancer effects:
https://nepis.epa.gov/Exe/ZyNET.exe/P100N4S8.TXT?ZyActionD=ZyDocument&Client=EPA&Index=2006+Thru+2010&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5Czyfiles%5CIndex%20Data%5C06thru10%5CTxt%5C00000036%5CP100N4S8.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=1&ZyEntry=1&SeekPage=x&ZyPURL
And please read the EPA’s Dose Response Analysis. https://nepis.epa.gov/Exe/ZyNET.exe/P100N4S8.TXT?ZyActionD=ZyDocument&Client=EPA&Index=2006+Thru+2010&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5Czyfiles%5CIndex%20Data%5C06thru10%5CTxt%5C00000036%5CP100N4S8.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=1&ZyEntry=1&SeekPage=x&ZyPURL
Now that you have read those, please consider the EPA’s “RfD” or Reference Dose which is sort of an EPA “safe” dosage to prevent SEVERE DF. RfD is an EPA term.
Note, in the EPA documents they propose raising the RfD. In other words, the NRC 2006 said the EPA’s MCLG was not protective. Instead of determining whether their RfD of 0.06 mg/Kg bw was protective (safe) the EPA proposes 0.08 mg/Kg bw is safe, an increase of 33%. Their graphs then show about a third of children will exceed this new proposed RfD.
Steve, I don’t want you to miss the fact that EPA did the exact opposite of the NCR 2006 report and instead of making their standard more protective, they made their standard LESS protective in order to try and fit policy. And even cooking safety, the EPA shows millions of children will exceed their new proposed RfD.
If you read the EPA literature, you will back out of your statement that EPA does not have a “safe dosage.” That is precisely how the EPA came up with 4 ppm.
#4. You say HHS has no authority over fluoridation. The United States Public Health Service (USPHS) is a division of the Department of Health and Human Services concerned with public health. It contains eight out of the department’s eleven operating divisions. The Assistant Secretary for Health (ASH) oversees the PHS. The Public Health Service Commissioned Corps (PHSCC) is the federal uniformed service of the USPHS, and is one of the seven uniformed services of the United States.
See PHS recommendation to lower fluoridation in public water. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4547570/
PHS recommends for those who choose, “For these community water systems that add fluoride, PHS now recommends an optimal fluoride concentration of 0.7 milligrams/liter (mg/L).”
0.7 mg/L is a reduction. The reduction is clear admission that some were ingesting too much fluoride.
#5. Geee. You are down on breast milk. Our species would have died out if not for Mother’s milk. OK, APA says mother’s milk is the ideal nutrient for infants which all other substitutes should be compared.
And the Infant Nutrition Council of NZ and AU state:
“Breastmilk is uniquely superior for infant feeding. It is the normal food for infants from birth.
“Breastmilk contains all of the essential nutrients, antibodies and other factors important for growth and development. It cannot be replicated.”
As a Nutritionist, I would maintain that the quality depends in part on the mother’s diet and quantity needs to be adequate. And the infant needs sunshine.
#6. If I am confused on dose and concentration, please explain your understanding. Concentration for fluoride is usually listed as mg/L or ppm. Dose is mg/KgBW.
#7. We agree.
#8. Snarky response is not called for.
#9. Wow, please provide references for, “Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans.”
#10. CDC is correct for some individuals. Read the EPA’s DRA and RSC and NRC 2006 report on total exposure.
#11. According to EPA’s legal counsel, FDA has jurisdiction because Congress has prohibited EPA from adding anything to water for the treatment of humans.
LikeLike
Hello Dr. Ghali,
I am an Assistant Professor at the University of Alaska Anchorage Division of Population Health Sciences. In the July 2019 O’Brien Report on community water fluoridation (CWF), your team referenced a paper that I coauthored and conducted in Juneau, Alaska. I studied the health and economic effects of CWF cessation. Fluoridation is a concern in Alaska (as it is in Calgary) because two of Alaska’s largest cities intentionally ceased long-standing CWF programs. The percent of Alaska’s population served by CWF in 2007 was 65% but fell to 49.3% in 2014 and remains so today because of local municipal policy changes fueled by misinformation about fluoridation. CWF misinformation is almost always supported by ‘scholarly’ citations.
As a nurse, mother to three small children, professor, and public health researcher, I read with keen interest the maternal fluoride – IQ study published in JAMA Pediatrics. I agree with the statements you made: that the study was funded by one of the NIH institutes, that it was reported in a well-known US medical journal, and conducted by a primarily Canadian team. However, those descriptive attributes don’t ensure quality or scientific rigor.
It is of concern to me that rather than addressing the modeling and statistical analyses conducted by the authors, you instead discuss the funder, journal, and location of the researchers. I could not find in the O’Brien Report, or by listening to your public testimony, your assessment of the quality of the data presented in the study or your reaction to the post-publication reviews. Isn’t that what the Calgary city council asked you to do – that is, to inform the council members about the quality of the scientific evidence?
You stated at the Calgary City Council meeting that, “The study exists and we can’t make it go away.” But you and your team know as well as I do that the fact that the study ‘exists’ is hardly the point. The point is a shared duty to assess the quality of the research for people who don’t have our scientific training.
Typically, scientists judge a study, or group of studies, not only through the peer review process but also by post-publication reviews. Only through scientific scrutiny and careful study of the methods and statistical analysis can a study’s worth be known. Such work of course takes time. Now that the post-publication reviews of the Jama/Peds F-IQ article are available, it is instructive to read them. Here are some:
1. Canadian Agency for Drugs and Technology in Health, “Community Water Fluoridation Exposure: A Review of Neurological and Cognitive Effects” https://www.cadth.ca/community-water-fluoridation-exposure-review-neurological-and-cognitive-effects-0
2. Science Media Centre: Expert reaction to study looking at maternal exposure to fluoride and IQ in children https://www.sciencemediacentre.org/expert-reaction-to-study-looking-at-maternal-exposure-to-fluoride-and-iq-in-children/
3. 3. Science-Based Medicine: “New study purporting to show a correlation between fluoride and IQ comes under heavy criticism.” https://sciencebasedmedicine.org/maternal-fluoride-and-iq/
The Canadian Agency for Drugs and Technology in Health (CADTH) reviewed the study and stated, the authors’ “conclusions were not supported by the data.” My goodness, isn’t that just about the worst thing that a prestigious agency could say about a paper?
You might also know that I was one of the 30 researchers from 6 different countries who co-wrote and signed a letter to the funders of this research group, the National Institute of Environmental Health Sciences. We sought the data from the study to re-evaluate the analysis and conclusions. This is a reasonable request from scientists who are concerned enough to seek the opportunity to replicate the study. I did not take personal offense when you misrepresented the purpose of the letter to the Calgary City Council and disregarded its details. None of this discussion is ‘personal’ or ‘agenda-driven’, as you claim. It is science-driven. Science does not care about ‘balance’, ‘middle ground’ or ‘both sides of a debate’. It cares about truth, facts, and accuracy.
I didn’t even take personal offense when you called the signers of the letter a bunch of liars at the city council meeting because I know you were simply misinformed. My concerns about the science underpinning fluoridation are professional. The fact that the CADTH has already negatively assessed the study means that the Jama/Ped F-IQ paper is almost certainly fatally flawed and cannot be relied upon. Yet since CADTH released its report, the O’Brien CWF Report has not been updated. I hope that you will revise the O’Brien Report to address the salient points. The public does not need to know who published the paper, funded it or wrote it, but rather whether the paper presents scientifically plausible and reliable evidence. Wouldn’t you agree?
From one health care professional and academic to another, I am asking you to please review the statistical analyses presented in the Jama/Peds F-IQ paper along with the post-publication reviews when you and your team update the O’Brien Report. I have placed below my signature 12 points that specifically concern me about the quality of the study and which I hope you will consider.
I am sure you would also agree that, while it may be uncomfortable for the leader of a public health institute to revise a report already published, your team’s pride can easily be set aside to correct a document when the health of children and community members are at risk.
Thank you very much for reading this post. I believe that you and I entered the health care and health research profession because we want individual’s families and communities to benefit from scientific advancement, all of which must be based on high-quality replicable studies.
Respectfully posted,
Jennifer Meyer Ph.D., MPH, CPH, RN
Assistant Professor
UAA College of Health
Division of Population Health Sciences
ps, I’d be happy to chat with you sometime about the above questions Dr. Ghali. Please don’t hesitate to reach out. Wishing you and your family a peaceful and joyful holiday season.
To readers: As a courtesy, I emailed this note to Dr. Ghali before posting. I hope he shares it with his team at the O’Brien Institute https://obrieniph.ucalgary.ca/about-institute/our-team
1. Please comment on the concerns noted by numerous experts about the unacceptably large confidence intervals in this study. As I recall, most (maybe all) bordered or included zero. Does that concern you?
2. The study does not consider whether the effect is nonlinear. As noted by others, multi-level modeling would have allowed for this type of investigation. Why do you think multi-level modeling isn’t being utilized?
3. What about the lack of adjustment for multiple hypothesis testing. Do you wonder why the authors didn’t do that?
4. The unadjusted IQ differences were not significant – does that concern you?
5. None of the exposure measures are validated, and even the authors acknowledge that fact. Can you please help me understand why more caution wasn’t exercised in the interpretation of the results?
6. Do you think it was strange the authors didn’t report the main effect finding for maternal urinary fluoride (MUF) and IQ? This is a violation of STROBE guidelines which I imagine you must certainly familiar with? Guideline 16 to be specific. Why do you think they didn’t include that? Also, does it seem odd that the Jama/Peds editors didn’t require the authors to conform to the guidelines? Does that make you wonder about the quality of the peer review?
7. Did you read the National Toxicology Program draft monograph on fluoride or simply rely on others to tell you what it said? I found it curious they included several studies as ‘low bias’ when the studies all share similar critical flaws, such as the ones identified in the Jama/Peds F-IQ article and other articles affiliated with the Jama/Peds F-IQ authors. These are as described earlier and include no adjustment for multiple testing, no adjustments for cluster sampling, and of course no multilevel modeling. Please be careful to note that this draft monograph has not been validated and on each page, the NTP authors write, “this DRAFT Monograph is distributed solely for the purpose of pre-dissemination peer review and does not represent and should not be construed to represent any NTP determination or policy.”
8. Were you worried about the cluster sampling method not being considered statistically? I found it very unusual the authors included IQ scores within 2.5 standard deviations or 98% of the scores. Including all the scores in a logistic regression means extreme values could have a lot of influence on the model. And look at all the low scores, those in the range of 50-70, they are all boys. Do we know if those boys all came from the same area or cluster? These might have been listed as clusters A, B, C, D, etc. But they were not listed given that there was no accounting or adjustment for cluster sampling.
9. Did it bother you in the FI analysis that they excluded 1 of every 3 mother-child pairs with and IQ test? That seems high? Researchers must work with the data they have of course, but wouldn’t it have been helpful to have a comparison sample note if there were any differences between those included and those excluded?
10. How about the r2 values and the outputs from the regression analysis? Did you find it unusual they were not presented in the supplementary materials? I wonder why they were not presented. Typically, in a paper, we aim to present all the findings.
11. What about the actual sign change noted in the results for MUF and IQ for boys and girls? A small difference between genders might be acceptable, but an actual sign change from – to + seems very unusual.
12. While I am not a physician, experts in nephrology seem very concerned about the inaccurate measures for urinary fluoride. Dr. F. Perry Wilson, a nephrologist at the Yale School of Medicine, criticized the Jama/Peds F-IQ article for relying on urine samples “because urine fluoride is not a perfect proxy for blood fluoride.” What do you think of his concerns?
LikeLike
Bill:
1. Obviously, you are the one who needs to read your comments and “not distort and twist”.
I draw your attention to your previous comment in which you state:
“Too many are ingesting too much fluoride. That is an undisputed fact which both of you would like to ignore, and the foundation for any discussion on fluoride.”
As you conceded in your second comment, this is not an “undisputed fact” as you falsely claimed. It is simply your unsubstantiated personal opinion.
2. “And second, I don’t know of any science which is not disputed, especially fluoride. Read what I write and try to understand. I don’t intend to argue.”
You’re contradicting yourself. You’re the one who claimed it was “an undisputed fact”. You’re the one who needs to read what you write.
3. In regard to the NHANES data to which you refer, the The National Center for Health Statistics has found this data to be unreliable and not reflective of any real increase in dental fluorosis over time.
“The analysis of the synthetic cohort with adjustment for possible changes in the demographic characteristics of the population over time suggests that the observed increase in fluorosis prevalence does not reflect the genuine amount of change within the U.S. population.” Indeed, the observed increase in the prevalence of dental fluorosis over time suggests that the way the examiners evaluated the level of fluorosis changed over time and the data do not reflect a real increase.”
—-AADR Response to New NCHS Evaluation of Dental Fluorosis Clinical Assessment Data from NHANES Over Time
American Association for Dental Research (AADR)
April 22, 2019
4. There is no valid, peer-reviewed scientific evidence of any risk of adverse effects to any “cell of the body” in association with mild dental fluorosis. The 2006 Committee on Fluoride in Drinking Water which you so frequently misrepresent, was composed of a variety of healthcare personnel and researchers. It, too, found all but the severe level of dental fluorosis to be cosmetic in nature.
5. What you “would maintain” in regard to mild dental fluorosis is groundless, meaningless and irrelevant.
6. Your unsubstantiated, unscientific guesswork in regard to caries reduction in mildly fluorosed teeth is meaningless and irrelevant.
7. Your personal critique of Iida and Kumar is groundless and without merit.
8. The only “safe fluoride exposure” set by the EPA is a maximum of 4.0 mg/liter in water. This takes into account exposure from all other normal sources of fluoride.
The EPA’s Dose Response Analysis identifies 2.0 mg/liter fluoride in drinking as the point of departure for risk of severe dental fluorosis. This is consistent with 2006 NRC finding that severe dental fluorosis does not occur in communities with a water fluoride level below 2.0 mg/liter (pp 114). This POD is 3 times the level of fluoride in optimally fluoridated water.
9. The 2006 NRC found 4.0 mg/liter to not be adequately protective for but 3 stated reasons:
a. risk of severe dental fluorosis
b. risk of bone fracture
c. risk of skeletal fluorosis
As noted by this committee, severe dental fluorosis does not occur with a water fluoride content below 2.0 mg/liter. Water is fluoridated at one third this level.
Bone fracture risk is a U-shaped curve, increased risk occurring with too little or too much fluoride intake. The point of least such risk is at the bottom of the U, in the range of the optimal concentration.
Skeletal fluorosis is so rare in the 74.5% fluoridated US as to be nearly non-existent.
10. There is no valid, peer-reviewed scientific evidence of any adverse effect resultant of “millions of children” exceeding an RfD of fluoride. Mild dental fluorosis is not an adverse effect.
11. “If you read the EPA literature, you will back out of your statement that EPA does not have a “safe dosage.” That is precisely how the EPA came up with 4 ppm.”
I see nothing here that warrants my backing out of anything. You simply exhibit, yet one more time, your lack of understanding of dose versus concentration. 4 ppm is a concentration, not a dose. It can therefore not be an EPA “safe dosage”.
12. In your comment, you asked: “Do you dispute the HHS lowered the concentration of fluoride in water?“.
HHS does not raise or lower the concentration of anything in drinking water. It has neither the authority, nor ability, to do so. To what you are attempting to refer is a recommendation by HHS as to the optimal concentration of fluoride in drinking water. There was no reduction in the 2015 reset of the optimal level recommendation. Due to recent science showing there to no longer be a difference in water consumption due to climate differences, HHS simply eliminated the previous optimal range of 0.7 ppm to 1.2 ppm set in 1962, and replaced it with a single point at the low end of that range, 0.7 ppm. With more sources of fluoride exposure now, than in 1962, HHS determined that the low point of the range would be sufficient to provide the same level of dental decay reduction, with no adverse effects. Thus was entirely in keeping with the original policy of setting the optimal as low as possible to allow for maximum decay reduction with no adverse effects.
13. I see nowhere that I am “down on mother’s milk”. I simply stated facts about human breast milk which you omitted.
“Overall, human breast milk has been found to be low in certain nutrients in developed countries: vitamin D, iodine, iron, and vitamin K.”
—-Med Hypotheses. 2018 Feb;111:82-89. doi: 10.1016/j.mehy.2017.12.020. Epub 2017 Dec 14.
Breast milk is conditionally perfect.
Erick M
Again, if you consider human breast milk to be the sole determinant of dietary requirements of infants, without supplementation, then you believe infants should be anemic free-bleeders who develop rickets.
15. “If I am confused on dose and concentration, please explain your understanding.”
See my item #11 above. It clearly exposes your lack of understanding of dose and concentration.
16. “Wow, please provide references for, ‘Yes, optimally fluoridated water is a concentration of fluoride in water at which the threshold of adverse effects of fluoride will not be exceeded through the consumption of this water in combination with fluoride intake from all other normal sources of fluoride intake. This is due to the limiting factor of water toxicity in humans.’ “
—-Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride.
https://www.ncbi.nlm.nih.gov/books/NBK109832/
—-J Clin Pathol. 2003 Oct; 56(10): 803–804.
Fatal water intoxication
D J Farrell1 and L Bower2
17. “CDC is correct for some individuals. Read the EPA’s DRA and RSC and NRC 2006 report on total exposure.”
That you deem the CDC be correct gives me great comfort, as I’m sure it will the CDC.
18. The EPA does not add fluoride to drinking water, nor does it mandate it be done. It simply regulates the concentration level of this and other contents in such water supplies. Fluoridation decisions are made on the state and local level. There is nothing in the law which prohibits this.
Because there can be no federal mandate of addition of substances to water other than for treatment of the water does not magically convey jurisdiction of drinking water supplies from the EPA to the FDA. Your “logic” in making this claim is bizarre even for you.
Steven D. Slott, DDS
LikeLike
Steve,
I wrote a long response and just lost it. So I’ll get to the main point.
You provided a reference. —-Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride.
https://www.ncbi.nlm.nih.gov/books/NBK109832/
They mention 0.05 mg/kg/day and I get the impression they think that is safe and effective. EPA uses 0.6 mg/kg/day.
Please go to Table 8-1 of your reference on Dietary Reference for fluoride.
13 studies are listed in Table 8-1. “Non-fluoridated” dose does not exceed 0.04 mgF/Kg body wt/day.
However, 5 studies have “mean” of 0.05 and 8, let me repeat, EIGHT of the 13 studies show excess fluoride dosage for many ranging from 0.7 to 0.13 mgF/kgbw/day
I presume you understand “mean”. 8 studies had many over 0.6 and some more than double EPA’s RfD of 0.6.
In other words, your data confirms my claim that many are ingesting too much fluoride. If you agree with your reference, you would agree, many are ingesting too much fluoride.
My definition of “many” would be more than 0.5%. Half a percent of 1,000,000 would be 5,000 children.
Your data suggests most studies would suggest 50% of more are ingesting too much fluoride, perhaps 500,000 children out of every million. In my book, that is “many.”
LikeLike
Bill:
1. UL for Infants 0 through 6 months: 0.7 mg/day
UL for Infants 7 through 12 months: 0.9 mg/day
UL for Children 1 through 3 years: 1.3 mg/day
UL for Children 4 through 8 years: 2.2 mg/day
Older Children and Adults Ages > 8 Years: 10 mg/day
— Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride.
https://www.ncbi.nlm.nih.gov/books/NBK109832/
Overexposure would be that which is above the threshold of adverse effects. As you can see 10 mg per day is the daily upper limit of fluoride intake before adverse effects for everyone above the age of 8. For those below this age, it is considerably lower, but due only to the risk of mild dental fluorosis in developing teeth, as evidenced by the huge increase in UL after teeth developing years 0-8.
2. Your inability to address my exposure of the fallacies of your other claims is taken as your concession to this.
Steven D. Slott, DDS
LikeLike
Steve, you state: “Your inability to address my exposure of the fallacies of your other claims is taken as your concession to this.” Second grader logic. Grow up. Just because I don’t have time to constantly repeat myself because you don’t read, doesn’t mean you can also put words in my mouth.
I don’t have time to do all your research for you.
Yes, DRI lists fluoride as a nutrient and has an UL. However, I have serious reservations on the DRI
First, look at the date of the DRI. 1997. In the last two decades has there been any research on fluoride safety/efficacy published? Hundreds of studies.
Then look at the areas of expertise of Panel members. Nutritionists mainly. Where were the toxicologists and pharmacologists or even dentists? None that I can see. In any panel of members, the conclusion will reflect the training and bias of those members.
DRI defines, “UL = the maximum level of daily nutrient intake that is likely to pose no risk of adverse effects to members of the healthy general population. Unless specified otherwise, the UL represents total intake from food, water, and supplements.”
The term “likely” is used for “healthy general population.” Does not sound either scientific or confident to me. However, nutrition is not a precise discipline and has numerous variables.
Are we only going to protect the “healthy” population? To hell with those having kidney problems, other toxic overdoses with lead, etc. To force everyone to ingest more fluoride when they are not healthy would not be supported by the DRI.
One of my majors in MPH was nutrition.
Nutritionists are frustrated because they can’t prescribe and we all want to “do good” “help people.”
Nutritionists did not consider the toxicity of fluoride, the evidence was and still is incomplete. Fluoride is highly toxic and fits within the definition of poisons, highly toxic substances. As such, it is regulated and permitted under two jurisdictions, pesticides and drugs. No nutrient is so highly toxic as to fit within toxic poison laws.
The absence of fluoride does not cause any disease. A nutrient is required to prevent disease, such as Vitamin C to prevent scurvy. Dental caries is not due to an inadequate intake of fluoride.
Fluoride may mitigate caries but does not prevent caries like Vitamin C prevents scurvy.
What is the UL of fluoride for the fetus? DRI does not include the fetus.
The UL was selected not on research of efficacy and safety but with the intent to protect the policy of fluoridation. Assumption was made.
A six month old infant drinks about 1 liter a day, so the UL was selected as . . . oh, let see, 1 X 0.7 would be 0.7 mg. So they chose that number. Not based on safety or efficacy but on policy and the best evidence they had at the time.
For today, the DRI has limited usefulness.
LikeLike
Ken and Steve,
(Correction on my last post. Whitford at the bottom of the list was on the DRI. I wonder if he would stand by his approval two decades later.)
Grandjean is one of the worlds top researchers of toxic substances. A prolific Harvard and Danish University published expert.
Fluoridation’s days are numbered. The question is how many children do we need to harm before we stop the excess.
Grandjean, P. Developmental fluoride neurotoxicity: an updated review. Environ Health 18, 110 (2019) doi:10.1186/s12940-019-0551-x
“Conclusions
Previous assessment of neurotoxicity risks associated with elevated fluoride intake relied on cross-sectional and ecological epidemiology studies and findings from experimental studies of elevated exposures. The evidence base has greatly expanded in recent years, with 14 cross-sectional studies since 2012, and now also three prospective studies of high quality and documentation of individual exposure levels. Thus, there is little doubt that developmental neurotoxicity is a serious risk associated with elevated fluoride exposure, whether due to community water fluoridation, natural fluoride release from soil minerals, or tea consumption, especially when the exposure occurs during early development. Even the most informative epidemiological studies involve some uncertainties, but imprecision of the exposure assessment most likely results in an underestimation of the risk [86]. Thus, the evidence available today may not quite reflect the true extent of the fluoride toxicity. Given that developmental neurotoxicity is considered to cause permanent adverse effects [69], the next generation’s brain health presents a crucial issue in the risk-benefit assessment for fluoride exposure.”
The published review is excellent with over 150 references.
LikeLike
Bill, Grandjean has a bias about water fluoridation – it’s no accident that he is often called on by FAN to make statements. Those statements are well outside any research he has personally done.
The current article is simply a review – all he has contributed is an interpretation driven by his bias.
Nevertheless, I must give him credit for actually including my paper in the section on Mailin & Till (2015) where he says:
Mind you he does not draw the obvious warning that many other studies suffer the same fault of not including important risk-modifying factors.
My paper has studiously been ignored by the Till crowd. They are quite aware of it – I know they have read it – but they dishonesty always refuse to cite it and still present their paper as if it was not flawed.
So good on Grandjean for not behaving the same way. But it is very ironic as he absolutely refused to allow my paper to be considered for the journal he controls -Environmental Health.
Interesting to look at who peer-reviewed Grandjean’s paper though. I suspect if it had been open to a more objective review he would have been told to reduce the basis of his conclusions.
Mind you the manipulation of peer reviewers is, I think, a widespread problem in scientific publication and should really be dealt with (in my time we didn’t get to choose oru reviewers as many journals now allow). But I have never seen anything as blatant as this particular peer review.
LikeLike
Ken,
And we all have some bias based on the science we review and understand. That is one reason we disagree. Another is thick headed stubborn obstinate pride.
You complain about Grandjean, “he absolutely refused to allow my paper to be considered for the journal he controls -Environmental Health.”
Yet you refuse to publish the paper I sent to you and then attack me, calling me a liar.
Well known when the science does not support the bias, the messenger is attacked.
But you don’t publish mine because you can’t refute the facts. Too many are ingesting too much fluoride and you know it.
You can’t refute the fact that we don’t know how much fluoride is needed to prevent or mitigate caries (if any) and we don’t have safety studies.
In the USA no government agency accepts jurisdiction for determining the dosage, efficacy and safety of fluoridation.
Fluoridation’s days are numbered. In the near future we will look back on fluoridation like we do mercury treatments and blood letting.
LikeLike
Bill:
1. Your continued inability to address my exposure of the fallacies of your claims is so noted. Your concession stands.
2. Yes, you obviously don’t have time to do any research, as evidenced by your comments.
3. Your unsubstantiated personal opinions on National Academy of Medicine DRI are meaningless and irrelevant.
4. There is no valid, peer-reviewed scientific evidence of any adverse effect of optimally fluoridated water on “those having kidney problems, other toxic overdoses with lead, etc.” or anything else.
5. There is no valid, peer-reviewed scientific evidence of any toxicity of fluoride at the optimal level at which water is fluoridated.
6. Fluoride in public water supplies is under the jurisdiction of the EPA, not “pesticides and drugs”.
7. Yes, dental caries is not caused by an inadequate intake of fluoride, any more than is polio caused by an inadequate intake of the Salk vaccine. Dental caries is caused by acid secreted by oral bacteria. Fluoride renders teeth more resistant to this acidic destruction.
8. There is no valid, peer-reviewed scientific evidence of any adverse effect on the fetus from optimally fluoridated water.
9. Your ridiculous claim for the reason of establishment of fluoride UL is meaningless, irrelevant, and an obvious product of your confirmation bias.
10. The lack of usefulness of NAM DRI to you is not surprising. Scientific evidence has never been of much use to antifluoridationists.
Steven D. Slott, DDS
LikeLike
Bill – you are an incorrigible liar.
You have never sent me a “paper” – and, come off it, I am not in the business of publishing scientific papers.
You sent me a document to be included in an open good-faith scientific exchange of the sort I had with Paul Connett – see <a href="https://www.researchgate.net/publication/298124881_The_fluoride_debate"The Fluoride Debate.
You then did not respond to my request of including references and correcting a figure (you obviously had not put together the document properly).
If you had done that small amount of work on your contribution our discussion would have gone ahead.
Surely I dot have to, yet again, provide the email exchange between us exposing your lies?
Surely you are not so inept that you couldn’t have corrected the document. I do not know why you decided to renege and pull out of our discussion but it is simply a repeat of a similar incident when you were director of FAN – see Do we need a new fluoride debate? and New fluoride debate falters
I have no problem discussing the issues raised in your contribution -especially as the work you referred to had been found deficient. I will no doubt deal with the paper you co-authored with Neurath at a later date – but the current propaganda on the IQ-fluoride issue is far more important.
When I do deal with the Neurath et al paper you will be able to comment – but your lies about this attempted exchange and your claim I am funded by “Russia” to ensure that fluoridation continues in the US so that American’s IQ is lowered simply show you are not fit for a proper open good faith scientific exchange. You are simply a buffoon.
Any chance of such an exchange with you here is completely off the table because of your lies and slander.
LikeLike
Ken,
OK, the document I sent you and you have refused to publish.
Because you don’t have the science, the facts, to refute the undisputed fact that too many are ingesting too much fluoride, you attack me and call me a liar.
Name calling is not science.
Every research I’ve heard you talk about is “deficient.”
Maybe you could provide a research paper which meets your standards. Demonstrate quality.
LikeLike
You lie again Bill, I did not refuse to publish at all. Do you want me to post the email chain of our communications at the time yet again?
You cannot find any evidence that I refused to post your article – you were the one who effectively refused to do the formatting, et., required for posting.
I am tempted to post the email chain as an article so that you are more widely exposed. However, I really don’t think anyone cares about this issue – your reputation is really bad.
LikeLike
Oops, Bill……looks like Ken’s exposed your “alternative facts” yet once again.
Steven D. Slott, DDS
LikeLike
Ken,
Fact: You asked to debate me on an article, communication, paper or document. You are playing with words in order to slander me. Lets call it a document.
Fact: I said we needed to start at the basics. You at first refused.
Fact: You then agreed and asked me to send you my document.
Fact: You wanted format changed.
Fact: I said it is OK as is and you can change format if you require for posting. Your choice.
Fact: You have not posted it. Refused, delayed, avoided, or what ever term you chose, and then slander me.
Fact: You simply attack the person, name calling, because you do not have the science to back up your bias. You change the subject because you lack science. You evade and avoid the tough questions and streams of evidence which do not confirm your bias.
Fact: you have not disputed that too many are ingesting too much fluoride. Instead you resort to slander and avoid science.
Fact: You have not provided an example of any research on safety/harm on any subject which you find to be ideal, great research, your gold standard without flaws. Show us an example of perfection.
Fact: You do not understand the study of human safety must be ethical and with individual consent. Giving people highly toxic substances to see how and at what dosage they are harmed is problematic, unethical and illegal . . . even with consenting prisoners. It appears, in your world, everything is safe unless you have the highest quality of science finding people are harmed. Those kinds of studies were done historically and are not ethical. A person cannot consent to being harmed.
Fact: you don’t have the science or laws on fluoride exposure to back up your bias.
In other words, Ken, you have not looked at the studies on efficacy. None are of good quality. Yet you expect the highest quality of study on harm/safety. You have a double standard.
You sound like one of Putin’s bullies. Stop your name calling and get back to science.
Too many are ingesting too much fluoride. . . and you have no reasonable science to refute that claim. You are overdosing millions.
LikeLike
Steve,
Instead of providing quality evidence that millions are not ingesting too much fluoride, you attack me.
“An ad hominem argument (or argumentum ad hominem in Latin) is used to counter another argument. … An ad hominem argument is often a personal attack on someone’s character or motive, rather than an attempt to address the actual issue at hand. This type of fallacy is often witnessed in debates in courtrooms and politics.”
At first Ken cautioned against ad hominems. That caution appears to have been removed.
Without the science to support your flawed theory, you guys only have personal attacks left.
LikeLike
Bill, a sensible person is very wary when anti-fluoridationists use the word “Fact.” We know it means a different thing to them.
But you are backing away from your claim I “refused” to publish your contribution.
This is the contribtion you sent – a pdf document.
My request for the word version was not a whim – as you can see a pdf version simply cannot be posted as text.
I asked for the word version. I also asked you to provide references and links (these are not included in the document). I also asked you to provide proper images – for example, this image is faulty:
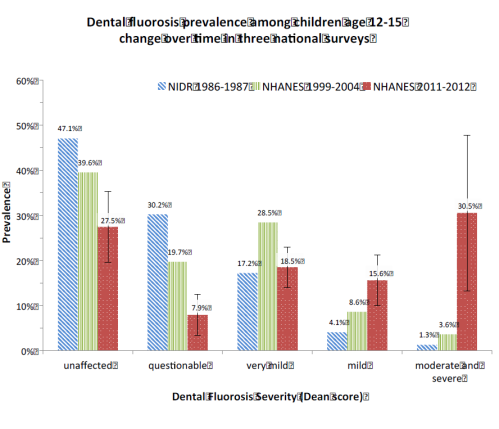
Other images are simply copied from a paper – one should at least remove the caption or describe the image in the text. for example your fig 5:

No, you did not hand this problem back to me – “you can change format if you require for posting. Your choice.” You undertook to do what I requested and then did not follow through.
As I said, one cannot post a pdf document (except in the way I have done in this comment). You refused to do the work required to make it available for posting. I suspect because you did not actually have the original word document or images for some reason.
So you simply lied – saying I “refused” to publish it – an outright lie.
I will, of course, cover Neurath’s paper in future – no rush as it has already been dealt with by others who show that the claimed increase of dental fluorosis is biologically impossible. I will cover the paper my way. You are obviously incapable of preparing a proper document for posting.
But because of your persistent lies about this – and your childish slander – claiming I am paid by “Russia” – there is no way I will ever repeat my offer of a scientific exchange with you because you are clearly incapable of such an open good-faith exchange.
LikeLike
Bill, yet you think it is ok to post the slander that I am paid by “Russia.”
You are simply a hypocrite suffering from the Trump Derangement Syndrome – you cannot deal with facts so use the Russia slander instead.

LikeLike
Ken,
I simply asked if Russia was behind/supporting your bias for overdosing so many with a highly toxic substance. Just asking.
If not, then perhaps a careful evaluation of dosage and efficacy will provide a background for judgment on safety.
And thank you for linking the document I sent you regarding excess fluoride exposure.
I look forward to your and Steve’s response.
Bias is strong. You suggest a “sensible person is very wary when. . . ”
I would add, a sensible person is very wary with all facts, especially from governments and those with vested interests. It is long past time for you to be wary of claims of “safe and effective” with the addition of fluoride exposure to everyone’s diet.
EPA’s DRA/RSC which I have frequently mentioned here has this graph which I have repeatedly talked about, Fig 8-1 above in your post and link.
As you can see, about a quarter to third of children are ingesting more fluoride than the EPA’s PROPOSED RfD (safe level).
And further, note infants are ignored.
And note this graph is based on a proposed increase of the RfD from 0.06mg/kgbw to 0.08 mg/kgbw. In other words, EPA was evaluating that even if they raised the RfD, many would be harmed. The current RfD would have the black line even lower showing even more harmed.
Those are not “anti-fluoridation” facts, those are EPA facts.
LikeLike
Con off it bIll, it is disgusting to pose such a question and you know it. It is simply slander and complete negation of any good-faith scientific exchange. IUnforutantley this sort of childishness seems to be permitted in the USA – it is being used because people can no longer discuss political issues sensibly.
It linked to your document (notice that you never did – I wonder why) simply to show that is was not in a state for posting here. And you simply refused to put into such a state. You have still not apologised for lying about this whole issue.
You had your chance of a proper discussion of these issues here and you blew it. You will not be given another chance here because you have behaved in an unacceptable way – lying about the issue and slandering me personally.
It is simply not worth entering into any discussion with someone who behaves this way.
LikeLike
Seasons greetings, Ken and Steve,
Lost my chance to change the document, is it. Science has such tight schedules and deadlines. I never felt you would publish it anyway. You don’t like to publish what doesn’t support your bias. Would be a waste of my time to have changed it and I’m busy. You never planed to publish in the first place. Over exposure doesn’t fit within the belief system of fluoridationists.
Doesn’t sound like you read the document before or recently. For example, you say, “Other images are simply copied from a paper – one should at least remove the caption or describe the image in the text.”
And I did explain it, starting before and after the graph. Yes, a copy and paste from the EPA’s DRA 2010 with reference.
Why do Ken and Steve persist in ignoring all streams of evidence or starting at the fundamentals, dosage?
Why do Ken and Steve persist in supporting overdosing of millions with a highly toxic substance, lacking high quality efficacy or safety studies, against their freedom of choice?
Good scientists, evaluating the same information, should come to a similar conclusion. Clearly, we are not evaluating the same information and you have refused to examine dosage.
Hierarchical evidence is a house of cards. Science fiction is often built on one single unknown, a time many years in the future. The story seems reasonable if we can accept that one unknown.
The same with fluoridation Accept the one simple unknown, dosage, and the story seems reasonable for many.
Too many are ingesting too much fluoride. The concept is undisputed. The only question is how many are being harmed.
LikeLike
Bill,
You state: “Too many (people) are ingesting too much fluoride.”
So, amongst those millions of people, over more than seven decades of Community Water Fluoridation, according to you there must be at least one person who has been harmed by CWF (apart from the cosmetic harm of tooth fluorosis).
I invite you to provide the evidence that this has actually occurred.
LikeLike
Don’t be silly Bill. I willingly published Paul Connett’s material despite its poor science. It provided an ideal opportunity to discuss the issue.
I would have published yours if it was properly formatted – no problem. Even though you were the Director of FAN at the time you don’t exactly have the abilities or standing Paul has and his articles here did not intimidate me. Why should yours – or do you think you are somehow better than Paul? Is that why you were replaced by Paul again after a short period as FAN director. Your boots (and head) got too big for you?
And I do not recall Paul sinking so low as to pull the McCarthyist “Russia” bogyman on me. That was certainly the pits. What a pathetic mind you have.
LikeLike
Too many are ingesting too much fluoride.
Which intimidates any fluoride promoter who seriously looks at the scientific facts.
The Russia financing came from another person here. You failed to answer and I began to wonder what pushes your motivation to force so many into unwanted ill health. So I asked and you failed to respond. A simple “no” would suffice. Instead you tell stories and evade the answer.
Too many are ingesting too much fluoride. You have evaded the concept of dosage. The only reason I can think of is because you don’t have science to back up giving everyone more fluoride.
LikeLike
Thanks for asking Stuart.
For about 25 years as a dentist I promoted fluoridation or fluoride supplements. I pushed the drug. Safe and effective, so I never spent the time to look or ask. Why should I look for something that CDC and ADA claim do not exist.
When I started to speak out against over exposure, that is when some came to me and explained their problems with fluoride.
Where endemic fluorosis exists, we know some of the early signs which include arthritic like symptoms, sore joints, enlarged joints. Which people with arthritic like symptoms have fluoride exacerbating or causing the pain? We have failed to diagnose and don’t know.
You ask about individuals. I’m very skeptical when a person says their dermatologist has told them not to use fluoride toothpaste and when they stopped their angular cheilitis cleared up.
Or the mom who took her high school daughter to HS sports competitions in various cities. After the hotel shower, mom sometimes noted a rash on the daughter. The next day she would call the water purveyor and ask if the water was fluoridated. Yes. However, never a rash with just chlorine.
Apparently some individuals are more chemically sensitive than others. Seems to run more often with autistic kids.
Here is a mom’s report of her autistic son. Three parts and I’ve condensed it here.
“I’m the mom of a delightful young man with autism, Kyle, age 30, who is severely hypersensitive to fluoride. Sadly, I didn’t know it for the first 14 years of his life and I didn’t even know of the countless other chemical sensitivities. We’ve traveled a very long and painful road together, his pain physical (and profound), my pain emotional.
“His speech is difficult, but he shows me his love and gratitude daily. He trusts me unconditionally because, in his mind, I fixed him. I got rid of the pain for Kyle, yes, but I could never have done it alone. Kyle doesn’t know of the countless FAN workers and advocates who, through their expertise, helped me to figure out how to protect my son. Most of them have never met me, never talked to me, but their work lives through the fantastic FAN website (www.FluorideACTION.net ), newsletters and videos.
“My eyes get wet and blurry just thinking about 1999, when Kyle was 13-14. He was in pain constantly, all over, but especially the back of his neck and his extremities (hands, feet, lips, tongue). The chronic pain had skyrocketed after what I’ll call a “toxicological event” at age 13 from a horrific reaction to a doctor prescribed “over the counter” (OTC) treatment that is completely benign to most people.
“He cried inconsolably when the pain in his fingers got so bad that he couldn’t play his beloved cello in the orchestra at school. He had to quit playing piano, too, and he could barely hold a fork to eat. There were mysterious pain “peaks”, especially in the middle of the night, but other times, too. He screamed and raced around the house as if pursued by killer bees. His school sent him home repeatedly with horrific headaches. At night the house shook wildly with the leg-pounding on the bed that was more like a 4-hour grand mal seizure than “restless leg”. His screaming was deafening. So little sleep….
“We went to 8 medical specialists and not one of them could diagnose the source of the pain, let alone help relieve it. Tylenol guaranteed a full-blown migraine the next day so was useless, as were other pain-relievers. He was completely intolerant of chemicals in the air and his food, so I changed his entire diet to organic, stopped using any cleaners or scented products and got the school to cooperate with a low-chemical environment. He only drank water—nothing else.
“With all of these changes, he improved, but still had pain every day, with screaming, racing, jumping, sweating, heart racing—gasping from the exertion…and crying, begging me to “Make it go away!”
“A mom from Beaverton, OR with two autistic teenagers was the angel we needed. She was the one who first told me in 2000 about toxic fluoride in tap water and instructed me to switch to reverse osmosis filtered water. There was a profound improvement in 3 days! Our lives changed dramatically for the better.
“No, he was not (is not) completely free of all pain—sadly, unexpected chemicals lurk everywhere. But by providing Kyle with fluoride-free water, chronic pain was no longer the 24/7 “norm”, so detecting the other chemical triggers was finally more achievable and allowed much greater success at avoidance. Fluoride remains the worst, and most difficult, to avoid. It took me many years to understand the many sources of fluoride (I will discuss these in part 2 of my letter tomorrow), and to fully realize the extent of Kyle’s sensitivity to it.
“Thank God for FAN’s information that has been there for me time and time again.
“It’s my hope that other children (and teens, and adults), who suffer as Kyle did, perhaps won’t suffer as long as he did. The problem is much greater for those with autism spectrum disorders. Please help FAN inform mothers across the world of the very real harm that fluoride does to some of our most vulnerable people.
“There is so much more to Kyle’s “Fluoride Story”, but you’re busy and I’m out of time. FAN will be sending out part 2 tomorrow. Meanwhile, Please help FAN put a stop to fluoridation with your generous donation. I’ve already sent mine.”
Stuart, I have spent time quizzing this mom. Why is she sure fluoride is one of the chemicals which cause her son pain. She goes into great detail. Better than most doctors do for their patients.
I’ll post the next two parts of her letter later if you are interested.
When we understand that fluoride is an enzymatic reactor, affects the mitochondria, then our concern turns towards how fluoride affects all tissues.
Start asking your patients. Dental fluorosis is a biomarker of excess fluoride. If just a cosmetic problem, no big deal. But fluoride dose not have a direct pipeline to the teeth avoiding all other tissues.
Too many are ingesting too much fluoride.
LikeLike
Don’t lie, Bill. You made the allegation/slander about Russian financing and specifically in relation to fluoride. There is no other person here who has suggested such rubbish – only you. And you know that because you don’t name anyone.
The whole thing is insane – even worse than me suggesting that the Russians are supporting the anti-fluoride movement in order to cause dental health problems in the USA. After all, Abby Martin devoted at least one of her RT programmes to presenting the anti-fluoride arguments and the video of that programme is often used by anti-fluoride activists.
No evasion from me – but a lot from you. You withdrew from the first attempt by me to get an exchange with you – specifically asking me not to publish what you had sent. And then refused to follow through in the second attempt.
The only consistent thing with you is the continual lies.
LikeLike
Perhaps you did not read the post. Within the last six months someone else asked you about your affiliation with Russia. You did not answer.
Ken, you said, “Bill, a sensible person is very wary when anti-fluoridationists use the word “Fact.” We know it means a different thing to them.”
Oh, right. You fluoridationists are so honest. Claiming, “Safe and Effective.” Claiming “Fluoridation prevents dental caries.” Two huge whopper lies. Perhaps, maybe with the stretch of hope the word could be “mitigate,” but to claim prevention is a big fat intentional lie to market a toxic substance to everyone without their consent.
If fluoride actually prevented dental caries, we could measure the difference in treatment and costs. Instead, fluoridationists estimate benefits rather than measure.
Just as many dentists per capita in fluoridation communities as non-fluoridation communities. Dentists make just as much money in both places, dental insurance payments are the same.
Ken, trying to take some sort of moral high ground only shows you’re bias. And who is pushing your bias? ADA, NZDA, who? I think you have simply avoided looking at all streams of evidence and enjoy trying to “outsmart” the experts on specific publications.
If you looked at the evidence from all sources and all streams you would not show your bias.
Too many are ingesting too much fluoride and the fluoride does not prevent dental caries and may not provide a life time of dental caries mitigation.
LikeLike
Bill,
I’ll counter your anecdote with one of my own.
A couple of years ago a commenter on this blog mentioned her sensitivity to CWF, I think in Auckland, and how she resolved the problem by obtaining her water from Tongariro, with no added fluoride.
I suggested that she should get the water she was drinking independently analysed. After all, Tongariro is the one place in New Zealand where the Ministry for Primary Industries advises farmers to be on the watch for fluoride toxicity in their stock…
Reach your own conclusion.
To allow yourself to be influenced by anecdotes is against all the principles of science.
From your anecdotal reply I am able to conclude that, in the more than seven decades of CWF, amongst the hundreds of millions of people who have benefitted from CWF, apart from mild fluorosis, you are unable to point out anybody who science has demonstrated injury from CWF.
LikeLike
Bill, it is hypocritical for a person resorting to McCarthyist attacks to defend their anti-science position to then talk about the moral high ground. You are an incorrigible lier – morals simply don’t come into it for you.
LikeLike
Stuart,
Catch 22.
You asked for “one person” who had been harmed from fluoride. I was reluctant because a case study has limited value.
When I answered your question, then you jump my bones.
I should never have responded to you.
However, now it is your turn to name one person who has benefited from CWF
Come on, I was reasonable with you, now you name one person who has benefited from CWF and give some good scientific evidence that person benefited.
And also, show some quality studies on benefit to the population as a whole from CWF. Quality studies of benefit don’t exist.
At least present your science “one person” has benefited from CWF.
LikeLike
Ken,
When are you going to attack the facts and science instead of the messenger?
Too many are ingesting too much fluoride.
You can’t dispute excess fluoride and it appears to rub you the wrong way.
LikeLike
Bill, you disqualified yourself from a scientific exchange with me. To sink so low as telling outright lies about my offer of a scientific exchange – to blame me for your inability to follow through – is despicable.
To make the McCarthyist smear – money from Russia for me – as a diversion from a proper scientific discussion is even worse.
The article for these comments is on scientific integrity and fluoridation and specifically about the way Dr Ghali attempts to prevent proper scientific peer review. That is a serious subject yet you have refused to contribute to it – you have attempted to hijack the discussion into an irrelevant direction and a cynical diversion. I refuse to divet and that makes you upset.
My advice to you, Bill, is to discuss the article, not attempt these dishonest diversions. There is no value in my allowing a commenter to continually attempt to undermine a proper scientific discussion in this way.
LikeLike
Bill,
Warning, anecdote: two people – my own children.
I grew up without fluoridation, but regular dental workups. Result was at least twenty fillings by the age of twenty.
My children grew up with CWF as well as regular dental workups. Result by the age of twenty was four fillings between them. Combined total of fillings less than a fifth of mine. That’s probably a benefit of CWF.
The genetics are (obviously) similar. Toothpastes, upbringing, education to professional level, food, (lack of) sugar ingestion, are all similar, so it’s highly likely that the presence of CWF had some influence on that outcome.
As for the actual science of benefits from CWF – haven’t you been reading this blog? Or read your dental textbooks? I’d just be repeating many papers that have been discussed here previously. Many population studies show benefits from CWF across entire populations. None have shown injury from CWF apart from mild fluorosis. And that science has been derived by collectively following hundreds of millions of people over more than seven decades.
By the way, pointing out that you appear to be allowing yourself to be influenced by anecdote rather than following the science, especially on a science based blog, is hardly jumping your bones. It’s just part of the scientific method and you can expect it if you don’t follow the science.
LikeLike
Stuart,
You say, “highly likely that the presence of CWF had some influence on that outcome.”
Anecdotal faith is not science. Highly likely for two children is not strong evidence.
For the past 90 years each generation has had fewer cavities than the previous, as a whole. (About level for the last decade.) You have no more factual data for benefit of CWF than proof of flying rain deer.
Your evidence is no stronger or weaker than the harm for Kyle from CWF. However, Kyle’s reaction is rapid and consistent. When he has a bath or shower with CWF, he has severe pain for several hours. You really don’t know if your children on a daily basis have fewer cavities.
Did your parents have you clean your teeth and visit the dentist as often as you have for your children? Did the schools teach the same? Many causes of caries and in Kyle’s case, pain. However, cause and effect is easier to monitor and evaluate than caries which takes many months/years.
However, two kids with fewer cavities than parents and grandparents is great news. If CWF actually helped, too bad so many were harmed with excess fluoride.
And you could have given your children fluoride from other sources but avoiding fluoride is much more difficult.
LikeLike
Bill,
Read my comment. I said I was replying to your anecdote with an anecdote.
Your request for scientific evidence of benefits of CWF was also answered – you can find the evidence in many of the posts and comments on this blog, and even in the textbooks that are required reading to gain a dental qualification.
That evidence was also in the required textbooks on public health when I obtained my own medical qualifications, and still is. I don’t need to waste bandwidth, or time, repeating publically available knowledge.
Despite population scientists following hundreds of millions of people for more than seven decades, there is still no evidence of harm from CWF other than mild fluorosis.
LikeLike
Stuart,
Yes, anecdote for anecdote. However, you ripped me apart for providing what you asked for.
And although each are individual cases, you cannot be as confident fluoride prevented caries because caries takes a long time to develop.
Whereas, an adverse reaction within a few minutes/hours and diagnosis of fluoride sensitivity by the patient’s doctor provides far greater confidence. The fluoride can be tried to see if the patient has an adverse response and avoided to see if not.
Kyle is very autistic and has no clue whether his mom is using fluoridated water or not. He does know when he gets pain.
You don’t want to waste time providing the science on benefit. Really? Is that because the science is incomplete and low to moderate quality?
No. . . you simply do not have the evidence of efficacy.
You say there is no harm from CWF. Perhaps you should look at the science of harm. Many, many studies.
LikeLike
Stuart,
It is true (fact) that since CWF started, dental caries have declined from about 5.5 cavities to about 2.2 cavities.for 12 year olds. At first glance, many give CWF the credit.
However, during the 4 decades prior to CWF starting, cavities fell from about 11.5 to 5.5, an even greater decline..
The critical question is, “what cause caries to decline prior to CWF?”
Seriously, Stuart, there were/are huge monster crushing caries unknowns which caused the decline. They did not stop caries reduction just because CWF started.
Fluoridationists give CWF credit for caries decline, but their research never includes the unknowns.
Just because two events happen does not mean they are related.
Too many are ingesting too much fluoride and the fluoride has risks and expenses with questionable benefit.
Have you noticed Ken does not discuss benefit or dosage of fluoride exposure? The science on benefit and dosage is more incomplete than risk..
LikeLike
Bill,
Just offhand, I can think of several possible causes of Kyle’s discomfort. He may not have been told whether water is fluoridated or not, but his parents are aware of the situation, and as an intelligent human being Kyle can pick up on his parent’s or caregiver’s expectations, just as much less intelligent non-human animals can pick up on their owner’s expectations. He actually does “have a clue” – or possibly a cue – just as non-human animals do.
And that’s the last I’ll discuss your anecdote. As you said: “just because two events happen does not mean they are related.”
“What cause (sic) caries to decline prior to CWF?” I’ll take a guess. Development and mass marketing of conveniently available toothbrushes and toothpaste/tooth powders?
Hundreds of millions of people have benefitted from CWF for over seven decades. The outcome of this has been followed by population scientists for all of that time. The data is publically available, particularly through the NHS in the UK, concerning health outcomes of matched fluoridated and non-fluoridated populations.
Rather than speculating that CWF may, or may not, cause adverse outcomes, why not look through those seven decades of data, amongst those millions of people, and see if CWF has actually caused adverse outcomes?
LikeLike
Bill, put aside your personal hatred for me – it interferes with your ability to discuss issues. It is very noticeable that you always attempt to divert discussion away from the articles you comment under – in this case, the issue of Dr Ghali’s attempt to close down scientific peer-review and the issue of scientific integrity).
But it is good to hear you say:
Correlation is never evidence for causation – but again and again, anti-fluoridationists act as if it were. Their whole reliance on the IQ issue at the moment (you seem not to have got the message from FAN headquarters of the change in tactics – hell that message couldn’t be made clearer) relies completely on using extremely weak correlations to argue causation. Without proper consideration of confounding factors or investigation of mechanisms
But you are completely wrong to say:
Other possible risk-modifying factors (or unknowns) are regularly included in investigating relationships with CWF – and some important effects have been demonstrated this way.
But the evidence for the efficacy of CWF rests on multiple sources, including investigation of mechanisms, surface reactions, etc., as well as basic chemistry.
The different approach of the anti-fluoridationists, the straw-clutching using weak relationships and reliance on correlations without other mechanistic support, is simply a result of the ideological and financial motivations of this group. The recent exposure of the role of Merocla in funding FAN and anti-vaccination groups is clear evidecne for that unscientific, ideological driving force (see Major funder of the anti-vaccine movement has made millions selling natural health products).
LikeLike
A huge problem with anecdotal “evidence’; of the sort almost exclusively used by anti-fluoridationists is that it ignores the psychological factors which are often the real causes. In the case of fluoridation this was shown by a Finnish experiment some time ago – see Fluoride sensitivity – all in the mind?)
LikeLike
Stuart,
You said, “Hundreds of millions of people have benefitted from CWF for over seven decades.”
Benefit of CWF is an assumption. I have looked at the science, many studies and reviews of the studies. None of the studies rise to the level acceptable to the US FDA, or I bet for Ken, you or me. Yet the assumption of benefit continues.
Thanks for speculating on the cause of caries decline prior to CWF. I too thought it might be toothpaste. However, fluoridated tooth paste was introduced after CWF, so that is not the reason for the huge decline prior to CWF.
Could it be tooth brushes? Maybe. If so, did the tooth brushing benefit max out right as CWF start? Not likely. Others have speculated increased shipping of fresh produce year round. Again, did the fresh produce max out just as CWF started?
No one knows and that huge confounding factor has not been included, factored in, or controlled, in any caries research.
LikeLike
Ken,
Three items to your post above.
1. I have no hatred for you or anyone.
2. I have repeatedly said raw data from research must be open for all to evaluate. That includes the CDC and HHS. They have pictures of the fluorosis in their survey’s and will not release the photos. Only one reason I can think of. The huge decline in dental fluorosis after 2012 is not physiologically plausible. The diagnosis changed or the data has been cooked. And they have not withdrawn their data or explained or provided the pictures.
3. You disagree that studies have not included confounding factors.
All CWF studies omit one or several of the following:
A. Not one Study corrects for Unknown Confounding Factors (such as the cause for decline prior to CWF)
B. Not one Prospective Randomized Controlled Trial
C. Socioeconomic status usually not controlled
D. Inadequate size
E. Difficulty in diagnosing decay
F. Delay in tooth eruption not controlled
G. Diet: Vitamin D, calcium, strontium, sugar, fresh and frozen year round vegetables and fruit consumption not controlled.
H. Total exposure of Fluoride not determined
I. Oral hygiene not determined
J. Not evaluating Life time benefit
K. Estimating or assuming subject actually drinks the water.
L. Dental treatment expenses not considered
M. Mother’s F exposure, Breast feeding and infant formula excluded
N. Fraud, gross errors, and bias not corrected.
O. Genetics not considered
Ken, you are very demanding of research showing harm, now be consistent and demand the same quality for benefit. In fact, the research on benefit must be strong before CWF is started.
LikeLike
Ken,
I agree that anecdotal evidence is problematic.
And even a placebo has significant claims of benefit.
What we look for is a significant increase of benefit from a medication greater than the placebo control.
The mind does powerful tricks. And that is a prime reason we need RCT studies for CWF.
The half life of fluoride in humans is about 20 years. A one month study will do little more than consider acute symptoms which may not have been measured adequately.
Increases in fractured teeth or bones, thyroid disorders, cancer, lower IQ, and a host of other symptoms will not show up in one month and not considered.
Ken, use the same critical thinking on dosage and benefit as you do for harm.
LikeLike
Bill,
You really do need to read things properly.
I never thought I’d have to be telling a dentist this. Toothpastes and tooth powders have been around for ages. The Romans and Greeks both had tooth powders. Toothpastes are noted in Victorian literature and their containers are found in museums. Tooth brushes have been around almost as long, but were originally made from wood/bone and animal bristle. Their handles can also be found in museums.
If you read my comment accurately, my guess was about mass marketing. Mass marketing of toothbrushes occurred after the development of plastics, and hence the mass market for toothpastes and powders increased at the same time.
If you demonstrably cannot read a brief comment on a blog accurately, how certain are you that you have correctly read the scientific consensus found in dental textbooks? The science that shows the efficacy and safety of CWF as demonstrated in millions of people worldwide over more than seven decades?
LikeLike
Stuart,
My point exactly. I agree with your comment about oral hygiene.
Tooth brushes and tooth powders were used long before the 1920’s. Could the mass marketing cause/contribute to an increase in usage of these and a decline in caries? Yes, indeed, they could be a major cause. We don’t know for sure.
However, Stuart, makes sense to consider tooth brushes and tooth powders caused a huge decline in the 3 to 4 decades prior to CWF. Could also have been increased transportation of fresh produce all year round. Or several other possibilities.
But one thing we know for sure. . . FACT. . . UNDISPUTED FACT. . . A NO BRAINER. . . . CWF did not cause the decline in dental caries prior to CWF starting. That’s my point Stuart. Huge factors more powerful than CWF are unknowns and never controlled for in research of CWF.
AND, If the decline was the tooth brush and powder/paste prior to CWF, did their benefit stop as soon as CWF started? Not likely. Yet you give credit to CWF when the decline after CWF started could still be what was causing the decline before CWF started. My point is, there are huge unknowns not controlled for with CWF research.
Remember, 50% of scientific consensus is wrong, it is our job to correct the wrong.
At one time the consensus was to treat dental caries with mercury fillings.
At one time the consensus was that root canals were 95% successful.
At one time centric relation explained how the mouth opened and closed (function, ROM, etc.)
Etc. Etc. Etc.
Science is not stagnant and is dynamic with discovery and corrections and improvements.
On another note, the FDA has approved fluoride toothpaste because the research is adequate. Fluoride works topically, not systemically.
Science is not a blind faith belief system.
LikeLike
Bill – McCarthyism is pure hatred and these days it does not have an ideological or political excuse – it is based on racism.
As foir research – I am demanding of all research. That derives from a lifetime of science publication and peer-review.
The example of Malin & Till (2015) is instructive. You would prefer I did not expose the flaws in this study and indeed Till still acts as if Perrott (2018) was never published. But that is how science works – most ideas in science are wrong and that is why critical and intelligent analysis of studies are required. That is how science makes progress and removes old and mistaken ideas.
LikeLike
Ken,
Let me try to understand you.
You say McCarthyism is pure hatred. I would define it as a hatred for Communism, or a campaign or practice that endorses the use of unfair allegations and investigations.
I disagree with Communism but don’t hate it. Are you referring to unfair allegations and investigations? Not sure your intent when you call it based on racism.
None of that has to do with science, so I’m not following you.
I don’t think CWF has anything to do with racism.
However, I’m 100% with you when you say, “most ideas in science are wrong and that is why critical and intelligent analysis of studies are required. That is how science makes progress and removes old and mistaken ideas.”
Therefore, if you thrust is towards unfair investigations of the science of CWF and fluoride exposure, then I agree.
You want to get into the details of specific studies of risk. Fine, we should. However, we first need to consider dosage, or we risk serious bias.
For example, hypothetical. Suppose you looked at the science of fluoride’s benefit and found benefit highly unlikely. And suppose you looked at dosage and realized many are ingesting too much fluoride from many sources. In other words, does little or no good and we are getting too much.
If we think fluoride ingestion has great benefit, then our bias permits some risk.
If we think fluoride ingestion has no/little benefit, then our bias becomes alarmed with any hint of risk.
Therefore, any discussion of risk needs to first start with dosage and benefit.
All drug regulatory agencies require that approach. First, show the research on benefit at a specific dosage. Once benefit has been established at a specific dosage, risk can be evaluated at that dosage.
Ken, unfair investigations of fluoride fail to consider dosage first. An assumption of great benefit results in a bias dismissing risk.
Happy New Year
LikeLike
Bill if you don’t think CWF has anything to do with racism why adopt a racist McCarthyyist attitude towards a scientist just because he is discussing the science? The fact is that racism, McCarthyism or accusations of “Russian” payments have absolutely no place in a discussion on this subject and the fact you adopted that approach disqualifies you from any rational discussion of the issue here.
Especially as there has not been any apology for that McCarthyist attack on me if for your lies about the proposed scientific exchange with me.
No apology at all – just more lies.
As for discussing the proven wrong ideas, or suspect ideas, in science – you are the one refusing to discuss the content of this article here – the question of integrity in science and Dr Ghalis attempt to stop peer review of the Green paper. You are doing that by attempting diversion onto irrelevant issues and by hateful attacks on me.
LikeLike
Ken,
After all the attacks you have done and do to me, looks like you have a very thin soft skin. You persist in calling me a liar and no apology from you.
I’m sorry. Now, would you please stop the attacks on me and go to the science . . . as I have repeatedly requested.
For the fourth or fifth time, I agree with you 100% that science should be open. I have given you at least one example. However, the Green paper went through two peer reviews, as I remember. Does not need another peer review, but I do not know why the data should not be open.
However, your bias and lack of willingness to start at the foundation and look at dosage, makes me doubt your judgment.
You are only looking at one side of the equation or puzzle. Start by backing up and looking at the most basics, i.e. dosage, and then move to the review of risk.
Dosage is where all good scientists reviewing the benefit of a substance start.
We all must start at dosage. Too many are ingesting too much fluoride.
Happy New Year
LikeLike
Bill, you are a liar – you lied about the proposed exchange on my blog claiming I had stopped it when it was you that refused to follow through.
that is a despicable lie – nothing to do with my skin – simply an indication you are incapable of a good faith scientific exchange to the extent you will use your laziness to manufacture a lie about me.
Until you ap[oligise for the lie and for the implication I am being paid by “Russia” there is absolutely no hope of a discussion of scientific issue with you here.
Please do not pretend to attempt a discussion of the science – you had your chance and you refused to follow through. You are simply attempting to divert from the content of this article and from the disgusting behaviour attacking me.
LikeLike
Bill,
Scientific consensus is that CWF is safe and contributes to improved dental health. That has been shown in hundreds of millions of people over more than seventy years. The research is demonstrated in your dental textbooks, in public health textbooks, by Cochrane, and in the many more recent papers cited on this blog.
Against this is your speculation, or belief, voiced amongst that of other anti-fluoridationists. Ken has repeatedly demonstrated that evidence in support of your speculation is lacking.
To support your speculation with evidence, all you need to do is to demonstrate, amongst the well documented data of those hundreds of millions of people, for over those seventy plus years, that CWF does not benefit dental health and/or injures health in other ways.
If your speculation is accurate then the existing data in populations with and without CWF will provide the supporting evidence. There’s no need for you to speculate, if your belief is accurate then the evidence is already in the data.
LikeLike