This is Ken Perrott’s response to Paul Connett’s second criticism of Ken’s article Fluoride Debate: Why I support fluoridation – 2nd response from Connett.
For Ken Perrott’s original article see – Fluoride debate: Why I support fluoridation.
It is a pity that Paul Connett chose to ignore the ethical question of balancing personal choice and social good because he took my comments on this as a personal criticism of him. They were not meant to be. I am happy to discuss the science but, in the end, science cannot make ethical and values decisions for us. Yes, it can, and should, inform those decisions – but pretending they are only about science does a disservice to science and to ethics.
Unfortunately science is often used in these sort of debates as a proxy for values issues. Professor Gluckman pointed that out in his statement What is in the water? An excellent article by Tania Ritchie in Science and Society outlines the dangers of this approach (see The fluoridation debate: why we all lose when we pretend it’s just about science). She shows how using science as a proxy backs people into pseudoscientific corners (and that is certainly an issue for these opposing fluoridation). It also places an impossible demand of certainty on science (“prove to me beyond doubt that fluoride at optimal concentrations is completely safe – if in doubt leave it out”). And concentration on the science often disguises poor ethical positions. She concludes:
“Using good science to counter bad science is productive. Using good science to tell us what will happen if we make a certain decision is also, of course, vital. But pretending science can tell us what decision we should make, or trying to counter ethical concerns with science, will never be helpful.”
Well, for the moment I guess I am opting for “using good science to counter bad science” but I hope we can return to these ethical issues at some stage.
Nature of bioapatites and systemic role for fluoride
Paul seems not to have taken on board my description of the structural role of fluoride in apatites and the recognised beneficial role of ingested fluoride. (Perhaps he considered that section was somehow a personal criticism and should be ignored.)
Mind you, I keep coming across that problem with other anti-fluoride activists. They wish to talk only about topical application of fluoride, and ignore completely the beneficial effects of ingested fluoride. This seems to create reading, hearing and comprehension problems for them. So I get accused of advocating that suntan lotion should be drunk or similar attempts at humour!
However, it is a critical feature of this debate so I will just start this response by briefly repeating a few things.

- Fluoride is a normal, natural component of bioapatites. In the real world these don’t exist as end-member compounds such as hydroxylapatite or fluoroapatite. They are more correctly described as hydroxyl-fluoro-carbonate-apatites.
- Accumulation of fluoride, together with calcium and phosphate, in our bioapatites is a normal part of development. This is beneficial because it helps strength our bones and teeth, and lowers their solubility.
- Both insufficient fluoride, or excess fluoride in our bioapatites can cause problems.
- Excessive dietary intake can result in excessive fluoride in our bones and teeth. Insufficient intake may also cause our bioapatites to be weaker and more prone to dissolve. When dietary intake of fluoride is reduced fluoride can be lost from bones and calcified tissues.
- The scientific literature reports that fluoride has a systemic role benefitting bones and pre-erupted teeth
Surface mechanisms for reducing tooth decay
We seem to be making a little progress here with the so-called “topical” mechanism – but only a little and very grudgingly. Paul has apologised for misrepresenting my explanation of the surface mechanism for the action of fluoridated water in countering tooth decay in existing teeth. He acknowledges that I was discussing the transfer of fluoride to saliva from water during drinking water, and not the smaller concentrations coming from the salivary glands after ingestion.
In this I was simply reporting what I have read in the scientific literature. But Paul will still have none of that. He concedes that fluoride in saliva “may or may not do something” and presents his own “simple personal observations” to claim that there is little chance of drinking water mixing with saliva. Not the first time I have heard this argument – and it always brings a picture to mind of a committed anti-fluoride activist drinking their water through a tube down the throat. I leave it to readers to observe their own drinking behaviour and decide if drinking water has little chance of mixing with saliva – or transferring ions to saliva.
So it is one step forward and another step back. Made worse by his assertion (from personal experience) “that the fluoride ions have little opportunity to form a biofilm on any teeth other than the back of the front teeth.” Of course the fluoride does not form a biofilm. It and other ions in the water and saliva do, however, transfer to, and diffuse through, existing biofilms (plaque) on the teeth.
There are quite a few reports of the effect of regular consumption of fluoridated water increasing the F concentrations in saliva and plaque both after ingestion (eg Cury & Tenuta 2008, Martínez-Mier 2012) and directly Featherston 2000, Bruun & Thylstrup 1984). (Yes, I realise that the CDC sates that the ingested fluoride delivered to saliva “is not likely to affect cariogenic activity” and this is echoed by other writers. However, there still seem to be workers who argue this does contribute and I am aware of laboratory experiments showing the mechanism can work at very low fluoride concentrations. But this is a detail I will leave to the experts – it doesn’t affect the current exchange).
Loaded language and scientific knowledge
Paul again refers to advances of scientific knowledge in a sneering way. He claims that the CDC “admitted” that research indicated the prevention of dental caries by fluoride occurs by a topical mechanism in existing teeth. He also speculates that the CDC “was scrambling to salvage some kind of role for fluoridated water . . . Despite its admission of the predominance of the topical effect.” Can somebody with research experience in chemistry really see scientific progress as some sort of winning-out over a conspiracy to ignore the “truth?”
Mary Byrne, a local anti-fluoridation spokesperson, shows a similar apparent misunderstanding of the nature of scientific knowledge when she describes, disparagingly, this progress in understanding as scientists being “wrong for fifty years.” She keeps repeating this even though her error has been explained to her.
These characterisations are like saying Newton was wrong with his laws of motion or that he was somehow hiding the truth and Einsteinian relativity is simply a case of scientists being forced to “admit”, or “concede” they were wrong – as if they had hidden something!
Use of loaded language like this has a political purpose which interferes with proper understanding of the science.
The journal Fluoride
Paul describes my comments about the journal Fluoride, and its editors, as “derogatory,” and accuses me of “double standards.” I think that shows a sensitivity and inability to consider my comments objectively. Not surprising, as Paul has some “irons in the fire” on this issue.
I said that “if I had some credible findings in fluoride chemistry and wished to present a paper to the scientific community for their consideration Fluoride is the last journal I would choose.” This isn’t completely hypothetical because I have published a few papers on fluoride chemistry. So how do I decide where to publish my work?
Firstly, my fluoride work was relevant to pedology and soil chemistry so it was natural to consider soil science journals. This was the audience to aim for and our work was of direct relevance to readers of those journals. I doubt that many of our intended audience or their institutes subscribed to, or read, Fluoride.
But, today if I were considering a general journal and had a look at Fluoride what would I find. First of all the website (where I would go to judge the journal’s scope, requirements and refereeing policy) – seriously, does this show a credible scientific society or editorial office?
That extremely amateurish web page puts me off – perhaps there are other general journals dealing with fluoride (contrary to Paul’s claim). Let us see if Journal of Fluoride Chemistry is better? See the difference?

Home page for the Journal of Fluorine Chemistry
Secondly, a quick skim of accepted papers in Fluoride indicates many are related to areas where fluoride toxicity is a problem because natural levels are high or excessive. The quality of many of these papers appears poor, a common problem where there are many authors whose main language is not English. It has a predominantly “third World” appearance. This would also raise a flag about possibly low standards of editorial review. Have a look at the list of contents for one of the 2007 issues.
None of these factors would attract me as a working and publishing scientist concerned at establishing a publication record in high quality and credible journals.
However, if I was a non-English speaker with routine work which I might find difficulty publishing elsewhere, and especially if that work was related to areas where natural fluoride levels were high, I would probably consider the journal. With the realisation in the back of my mind that I would probably have no luck with submission to a more reputable journal.
Now, I am not being “personal” or “derogatory” in making that realistic evaluation. Nor do I think there are “double standards’ in choosing a good journal for publication. Good work deserves a good journal for publication.
Paul effectively concedes this in referring to attempts by Xiang et al to get their work published in a more reputable journal. He laments the fact that this journal would not include material already published in Fluoride (standard procedure in the publishing world) as amounting to Xiang’s material being “withheld from the mainstream scientific community.” (Paul obviously agrees that Fluoride does not have a good standing in the mainstream scientific community). The lesson being that Xiang should have gone for the reputable journal first time around. Why publish in a journal which does not give access to “the mainstream scientific community” if one’s work is good enough to get published in a reputable journal
That is a sensible question – not a derogatory one.
Connett’s relation with Fluoride
It is instructive to look at Paul Connett’s own publications in Fluoride. He claims to have researched the issue for 17 years and I would expect that at least some of his research papers would have ended up in this journal.
A simple search for the name Connett showed me a couple of guest editorials – often coauthored with editors of the journal (see for example Professionals moblize to end water fluroidation and Misplaced trust in official reports), a book review (coauthored with editors of the journal), reports of the International Fluoride Society (IFS – owner of Fluoride) conferences. There were abstracts of papers or posters presented at IFS conferences authored by Paul, Ellen and Michael Connett – but no sign of formal papers for these. (I hope Paul will correct me and provide links if I have missed papers with full text.)
This at least tells me that Paul is on excellent terms with those editing and running this journal. Not surprising when one looks at the names in the editorial board of the journal, the western contributors to the journal and the names on the advisory board of Paul’s activist organisation Fluoride Alert.
Another thing that stands out for me about the editorial and advisory boards is the large number of retired, former, emeritus academics (around 17 from a glance). In the past I have also noticed this about the organisations and petitions of climate change climate contrarians/deniers/pseudosceptics. As a retired scientist myself I can appreciate how such issues can become hobbies, and avenues for social involvement and personal standing for people who formerly relied on their employment and professional standing for such things. I can also appreciate that retirement often also means loss of contact with current research and findings. This increases my suspicions of the journal and organisation.
There was one normal looking journal paper by Michael Connett “Vulvar paget’s disease: recovery wihtout surgery following change to very low-fluoride spring and well water.” My impression is this was simply an anecdotal history for one person – probably not normally acceptable in a scientific journal (unless at least written by the practicing medical person handling the case). A quick search of Google Scholar shows this to be Michael’s sole scientific paper – perhaps not surprising as he is not a scientist. He is the Special Projects Director for the Fluoride action network, an attorney in Philadelphia, PA, and received his law degree from Temple Law School in 2011. But now has a scientific publication record!
(Note for non-scientists wishing to show a scientific publication record. There are plenty of anecdotal stories on the internet by people claiming sensitivity to fluoride. Hell, the other day I read the personal account of one person with skeletal fluorosis which cleared up immediately he stopped drinking tap water! You could select your own “case history,” write it up as a scientific paper and submit to Fluoride. Mind you, your paper might not be all that visible to the “mainstream scientific community”).
Looking at Fluoride, Fluoride Alert and the International Society for Fluoride Research I get a strong impression of a group who take in each other’s laundry – but at the same time give publication space for some third world scientists who may not meet the standards of more reputable journals.
Paul gave it away when he reported to us that “the US National Institute of Health (NIH) has refused to cover the contents of this journal in PubMed.” Surely that tells us something about how this journal is considered by the science community (and please – if one has to resort to conspiracy theories to explain this the argument is surely already lost.)
Bones, hip fractures and the literature
Kurt Ferre’s comment about misrepresentation of the Li et al (2001) paper referred to Paul’s note on it in Fluoride Alert (Reason 29 of 50 reasons to oppose fluoridation). Here Paul did describe the data as relating to hip fractures and not over all fractures. OK, Paul in chapter 17 of his book may have been more specific but that is not what Kurt referred to. (By the way, I am still plodding through Paul’s book – on chapter 9 at the moment).
Paul claims I “prefer” an “interpretation” of the Li et al (2001) paper that there is a “sudden” appearance of hip fracture at a higher concentration rather than a linear increase from low concentrations. He is wrong – I don’t prefer any specific interpretation. I was merely pointing out what can be drawn from the statistical analysis of the data.
One of our commenters has already noted that Paul’s argument for his own intepretation of the data here amounts to special pleading – where he has to ignore, or denigrate, the statistical analysis. He is pleading when he writes that increases “appear to be ‘real’ even though they are not statistically signficant individually.” Or that the data “appear consistent with a linear regression. Statistical significance is not the final word on whether a data point or data set is real or not.”
These were the sort of statements I would put red lines through when I was reviewing papers submitted for publication.
However, this is a digression. The interpretation of the increase at higher concentrations is not important. The fact is neither overall fractures or hip fractures showed an increase at fluoride concentrations considered optimum for oral health.
It was clear to me when I originally read and wrote about Li et al’s (2001) paper (see – Is fluoride an essential dietary mineral? ) that the increased incidence of overall fractures at concentrations below optimum did not refer to hip fractures. The authors specifically brought that to readers attention – “the data show a somewhat different pattern for hip fractures in relation to the water fluoride levels. . . Instead, the prevalence of hip fractures was stable until the water concentration reached 1.45–2.19 ppm.” They qualified this with “However, it may not be appropriate to conclude that the risk of hip fracture is more sensitive to the water fluoride concentration as compared with overall fractures, because the number of hip fractures in the present study is relatively small.” And they did conclude that “our results on hip fractures support previous findings that fluoride around 1 ppm in drinking water does not increase the risk of hipfracture.”
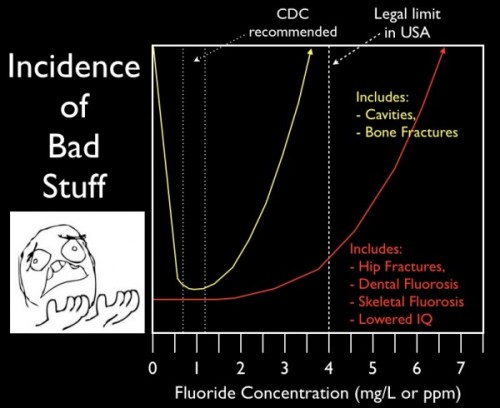
This diagram by Ethan Seigel (which I reproduced in an article earlier this year (see Getting a grip on the science behind claims about fluoridation) was clearly taking on board Li et al’s work – when perhaps it should not have been so specific.
But of course the issue of hip fractures does not rest with the work of Li et al alone. I wrote about this specifically in Fluoridation: the hip fracture deception where I also mentioned the recent paper of Näsman et al (2013) “Estimated Drinking Water Fluoride Exposure and Risk of Hip Fracture: A Cohort Study showing no significant correlation of hip fractures with fluoride in drinking water at the optimum concentrations.
Miscellaneous
Delivery systems: It seems I must respond to Paul’s suggestion of “an alternative delivery system for fluoridated water” – selling fluoridated bottled water. I guess that already happens in many places but I did not take his suggestion seriously because he is offering it as a substitute for already existing social health policies. That is not my area of expertise but I can understand how fluoridated water and fluoridated salt are effective as social policies for overcoming problems where the natural fluoride levels are deficient. Surely bottled water in the corner of a “supermarket, pharmacy or clinic” hardly measures up as a social health policy? Fluoridated salt seems to me to be a more credible alternative to water fluoridation.
Having said that, bottled water is culturally preferred in some countries and is attractive to some age groups in others. There are suggestions, therefore, that fluoridation of bottled water should be encouraged. New Zealand and Australia recently brought in regulations allowing this.
Inference from high concentrations: Paul has objected to my criticism that he often relies on extrapolation from laboratory or epidemiological studies where higher than optimum fluoride concentrations were used. He responded by discussing Xiang et al (2003) and argued that some of the studies covered by Choi et al (2012) did include lower concentrations.
However, there is still a tendency to then fall back on all the studies to give extra weight to his assertions, rather than just rely on the low concentration studies. I think the image below prepared by fellow New Zealander Andrew Sparrow helps put this issue into context. High fluoride cases in Choi et al (2012) were almost all completely out of the zone for optimum fluoridation of drinking water.

Appeal to authority with declarations: This tactic is used a lot by anti-fluoride activists. The poster below is a recent example from Fluoride Free NZ. The inclusion of a citation gives it some authority – but can anyone find that paper? No one at Fluoride free could – yet they were promoting a claim using the citation!

The Journal of Dental Medicine is now defunct and I could find no abstracts or full text on the internet. However, I did find a description at http://slweb.org – a well-known anti-fluoride activist site. This claimed adverse reactions, affecting “the dermatologic, gastro-intestinal and neurological systems,” to fluoride in 1% of the group studied! I would have liked to check out the statistical analysis used in the study as this seems a very small response. Was 1% significantly different to zero in this study?
What the hell – Fluoride Free NZ doesn’t care. They went ahead with a poster and its promotion anyway. As a political activist group they are concerned more with moulding public opinion than the facts.
Paul might argue this case is a diversion he is not responsible for. But my point is that activists do this sort of thing all the time. And Paul is no different with the way he quotes from the NRC (2006) report in his section “7. What other authorities are saying about fluoride as a neurotoxicant.”
He quotes phrases like:
- “the results appears significant enough to warrant additional research on the effects of fluoride on intelligence.”
- “These changes have a bearing on the possibility that fluorides act to increase the risk”
- “More research is needed to clarify fluoride’s biochemical effects onthe brain.”
- “studies of populations exposed to different concentrations of fluoride in drinking water should include “
- “Studies of populations exposed to different concentrations of fluoride should be undertaken”
- “Consideration should be given to assessing.”
The point is one can agree with all these suggestions for ongoing and future research and still accept the current assessment that fluoridation is safe. Just because there is a logical possibility of a suggested danger does not, in itself, make that danger real.
This ongoing research is happening and health authorities do monitor current research findings. In New Zealand the Ministry of Health set up the National Fluoride Information Service to do this specific job and it regularly reports current research findings. Similarly, a report from the NZ Parliamentary health committee just the other day recommended:
“the Government work with the Ministry of Health to ensure that the addition of fluoride to the drinking water supply is backed by strong scientific evidence and that ongoing monitoring of the scientific evidence is undertaken by, or for, the Ministry of Health, and that the Director-General of Health is required to report periodically to the Minister of Health on the status of the evidence and coverage of community water fluoridation.” (see From dental neglect to child abuse?).
It is irresponsible to use such urgings to continue research as some sort of proof that there are problems sufficiently big enough to warrant abandoning a social health policy known to help people. Or to call that social health policy “reckless,” as Paul does.
Paul Connett does the same thing with the paper by Xiang et al (2003) and other Chinese work in the area of IQ. He acknowledges himself that “there are weaknesses in many of these IQ studies.” These weakness and the speculative nature of his conclusions do not stop him from seriously claiming that there is a very low limit of sensitivity to fluoride effects on IQ. I repeat my question from my last article about the huge variability in the data and how the hell one can place any confidence on the result drawn from Xiang’s figure.
“Yet Paul uses Xiang’s paper to authoritatively claim it had “found a threshold at 1.9 ppm for this effect.” (What effect he refers to is unclear.) How reliable is that figure of 1.9 ppm (actually 1.85 or 2.32 ppm F in the paper) – considering the huge variation in the data points of the Figure 1? (Unfortunately the paper is not a lot of use in explaining that figure – reviewers should have paid more attention.)”
The final request: Paul wants me “to list the primary studies that you have read which most convinced you that fluoridation is both safe for the bottle-fed baby and for the adult over lifelong exposure.” In thinking about this I have concluded it is a strange request because I don’t think creative scientists think that mechanically.
My concepts and ideas derive from multiple sources – I never put my eggs all in one basket as it were. I can find I am impressed by something in a paper which also has something which doesn’t impress me. Consequently I take what I can from wherever I can and try to critically understand what I read.
It’s a bit like that with people. You have to accept them warts and all and avoid the immaturity of placing anyone on a pedestal – a sure way to later find they have feet of clay.
So unfortunately I cannot satisfy Paul’s request. He will have to deal with the actual arguments I put forward.
As for the issue of bottle-fed babies – I am sure this will come up at some stage. It already has in the comments discussion.
Anyone wanting to follow the debate and/or check back over previous articles in the debate can find the list of articles at Fluoride Debate.
See also:
Similar articles on fluoridation
Making sense of fluoride Facebook page




















